
Abstract
A limited number of studies using differing imaging approaches suggest that there are regional variation in the cerebrovascular response to hypercapnia and hypoxia. However there are limitations to these studies. In particular, it is not clear if existing studies of hypoxia have fully accounted for the confounding effects of the changes in arterial PCO2 on cerebral perfusion that, if uncontrolled, will accompany the hypoxic stimulus. We determined quantitative maps of grey matter cerebral blood flow using a multi-slice pulsed arterial spin labelling MRI method at 3 T at rest, during conditions of isocapnic euoxia, hypercapnia, and mild isocapnic hypoxia. From these data, we determined grey matter cerebrovascular reactivity maps which show the spatial distribution of the responses to these interventions. Whilst, overall, cerebral perfusion increased with hypercapnia and hypoxia, hypoxia cerebrovascular reactivity maps showed very high variation both within and between individuals: most grey matter regions exhibiting a positive cerebrovascular reactivity, but some exhibiting a negative reactivity. The physiological explanation for this variation remains unclear and it is not known if these local differences will vary with state or with regional brain activity. The potential interaction between hypoxic or hypercapnic cerebrovascular changes and neurally related changes in brain perfusion is of particular interest for functional imaging studies of brain activation in which arterial blood gases are altered. We have determined the interaction between global hypoxia and hypercapnia-induced blood oxygen level-dependent (BOLD) MRI signal and local neurally related BOLD signal. Although statistically significant interactions were present, physiologically the effects were weak and, in practice, they did not change the statistical outcome related to the analysis of the neurally related signals. These data suggest that such respiratory-related confounds can be successfully accounted for in functional imaging studies.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
1 Introduction
It is well known that the cerebral circulation is sensitive to changes in arterial blood gas tensions; hypercapnia and hypoxia both, independently, increase cerebral blood flow . There is therefore a close linkage between the regulation of breathing and the regulation of cerebral blood flow; changes in breathing will alter the concentrations of oxygen and carbon dioxide in arterial blood, and thus cerebral blood flow. The cerebral vascular response to hypercapnia has been used to assess the integrity of the cerebral circulation and has been shown to be altered in different physiological and pathophysiological states. For example, the cerebrovascular reactivity to hypercapnia is reduced in the morning compared to the evening [17] and is lower during slow wave sleep than during the waking state [16]. It is also modified in patients with sleep disordered breathing [23] and with heart failure [18]. These disease states, along with other cardiorespiratory conditions, are also associated with reduced levels of arterial oxygen (hypoxia). Hypoxia is of clinical significance as the brain is particularly vulnerable to the effects of low oxygen [5]. The physiological response of cerebral blood flow to hypoxia has been less extensively studied than that to hypercapnia. However, the consensus is that cerebral blood flow increases in response to moderate and severe hypoxia; the response to mild hypoxia is more equivocal (e.g. [17, 25]); like hypercapnia, the response to hypoxia is altered in certain physiological states, e.g. sleep [16]. Most investigations of the cerebral blood flow response to hypercapnia and hypoxia have been performed using transcranial Doppler ultrasound ; this method has high temporal resolution but is limited to the study of flow velocity changes in individual arteries. Relatively little is known about the regional responses of the cerebral circulation to these stimuli. However, any differences in such responses may be significant as they may determine the relative degree of protection afforded to different brain areas in response to such insults.
2 Determination of Regional Cerebral Perfusion
A number of methodologies can be used to determine regional cerebral perfusion in humans. Single photon emission computed tomography (SPECT) determines the distribution of a gamma emitting radionucleotide across the brain. Usually for perfusion-related studies the ligand 99mTc-HMPAO (hexamethylpropylene amine oxime) is used (e.g. [21]); this will distribute around the brain in proportion to blood flow. The method is limited in application as it has relatively low spatial resolution and the relatively long half-life of ligands means that repeated measurements can be made relatively infrequently. The total number of measurements are limited by radiation dose. Regional cerebral blood flow can be determined using positron emission tomography (PET) using the H2 15O as the radioligand (e.g. [26]). As with SPECT the ligand distributes around the brain in proportion to brain blood flow. The positrons emitted during the decay of the 15O are each annihilated in collision with an electron producing two co-incident gamma rays at 180° to each other. This results in a greater spatial resolution than that of SPECT and the short half-life of 15O allows measurements to be repeated every few minutes. Concomitant arterial sampling allows an accurate calibration of measurements and H2 15O PET is regarded as the “gold standard” for measurements of regional cerebral blood flow. However, like SPECT the scope of such studies are limited by increasingly stringent regulations limiting total radiation doses.
Considerable information on cerebral perfusion has been obtained using blood oxygen level-dependent functional magnetic resonance imaging (BOLD fMRI) , a method that is safe and repeatable and has high spatial and temporal resolutions. The methodology relies on using deoxyhaemoglobin, a paramagnetic compound, as an endogenous contrast agent. In particular, changes in the concentration of deoxyhaemoglobin alter the magnetic susceptibility of the blood and produce local inhomogeneities in the magnetic field that are evident in MRI T2* images. The change in the BOLD signal can be used as a marker of the change in regional brain perfusion that accompanies changes in brain activity [32]. The phenomenon is now widely exploited as the basis for functional neuroimaging. However, the relationship between the BOLD T2* signal and brain perfusion is not straightforward; local changes in the signal will reflect changes in both local haemoglobin saturation (i.e. the ratio of HbO2 to Hb) and local blood volume (i.e. the concentration of Hb) [4]. The relationship to local blood flow will further depend on the rate of oxygen extraction in the local tissues.
Other MRI approaches offer more direct measurements of local cerebral perfusion. In particular pulsed arterial spin labelling (PASL) methods allow repeated and non-invasive determination of the cerebral blood flow or perfusion [7, 8]. PASL determines brain perfusion by monitoring the transit of magnetically labelled blood through a region of interest. It is well known that PASL methods for determination of cerebral blood flow suffer from low SNR compared to dynamic susceptibility contrast methods using paramagnetic contrast agents; the latter, however, are not feasible for applications requiring repeated determinations of cerebral blood flow as a full elimination of the contrast agent is necessary before repeating the scan. For this reason PASL methods are increasingly used to investigate and monitor brain perfusion under normal and pathological conditions [9, 11, 33] and where changes in cerebral blood flow related to physiological stimuli [13, 30, 31] or brain activation [14, 29, 31, 34] are of interest.
3 Regional Cerebrovascular Response to Hypercapnia
The first study of the regional cerebral blood flow responses to hypercapnia using H2 15O PET was performed by Pinard et al. [22], who determined responses in three anaesthetized baboons . The authors reported good reproducibility in the measurements of regional cerebral blood flow using hypercapnia and no notable differences in response were reported across 12 regions of interest. Subsequently, Ramsay et al. [26] determined differences in H2 15O PET regional cerebral blood flow in cortical grey and white matter regions of interest in humans using hypercapnic and hypocapnic stimuli . The study, however, did not explore differences between different cortical sites. Ito et al. [10] specifically tested the heterogeneity of the response the hypercapnia and hypocapnia with H2 15O PET in humans and reported significant relative hyperperfusion during hypercapnia in the pons, cerebellum, thalamus, and putamen.
Kastrup et al. [12] investigated the regional variability of the BOLD response to breath-hold-induced hypercapnia in five predetermined regions of interest. They reported that BOLD signal changes in the cerebellum and visual cortex were significantly higher than in the frontal cortex and basal ganglia. BOLD signal changes in the cerebellum were also significantly higher than in the sensorimotor cortex.
Our own unpublished data show significant heterogeneity in the BOLD response to hypercapnia (produced by increasing inspired CO2) across the cortex. However, MRI angiography suggests that the sites of the largest signal changes to BOLD include large veins and venous sinuses which are particularly evident at the boundaries of both the visual cortex and cerebellum (Fig. 11.1).

Influence of large veins on inhomogeneities in the regional cerebrovascular response to hypercapnia. MRI angiography of venous vessels (a) has been superimposed upon anatomical (T1 weighted) MRI section of (b) the whole brain in sagittal section and (c) the cerebellum in transverse section. (d) Magnitude of BOLD signal change in response to hypercapnia in three contiguous sagittal sections of the cerebellum anatomically close to the section in (c). Increasing signal change is indicated in an arbitrary scale from grey to white. Note that the areas of greatest signal change in response to hypercapnia are anatomically similar to the location of large veins
A further note of caution must be made that all such mapping studies inducing hypercapnia by breath holding or by modulating inhaled gas concentrations, will necessarily include changes in neural activity associated with changes in the sensory motor task and with the “experience” associated with the changing blood gases. These neurally related signal changes must, at least in part, contribute to any observed differences in the regional cerebrovascular responses.
As described above, PASL is being increasingly used to determine regional cerebral blood flow. Typically, MRI scanners of different field strengths will be utilised for clinical investigations and the effects that this will have on quantification is uncertain . Therefore we determined cerebral blood flow at 1.5 and 3.0 T, under normo- and hypercapnia, using a pulsed arterial spin labelling technique [19]. To improve grey matter cerebral blood flow quantification white matter was excluded by using a high-resolution grey matter mask. The cerebral vascular reactivity to hypercapnia was derived from the quantitative grey matter cerebral blood flow maps. For both field strengths, the grey matter cerebral blood flow was significantly higher under hypercapnia compared to normocapnia. For both conditions, there was no significant difference of grey matter cerebral blood flow for 1.5 and 3.0 T; the same applied to the determination of cerebral vascular reactivity, which was 4.3 and 4.5 %/mmHg at 1.5 and 3.0 T, respectively. These data indicate that, with appropriate approaches, field strength will not affect quantitative determinations of cerebral perfusion.
4 Regional Cerebrovascular Response to Hypoxia
A limited number of studies have used perfusion-sensitive MRI to investigate the cerebral blood flow response to hypoxia. Some studies suggest that the response to hypoxia may be uniform across the brain, others indicate some inhomogeneity. However, it is not clear if these existing studies have fully accounted for the confounding effects of changes in arterial PCO2 on cerebral blood flow that, if uncontrolled, will accompany the hypoxic stimulus [27, 28, 31].
Our laboratory determined quantitative cerebral blood flow maps of cortical grey matter with a pulsed arterial spin labelling technique at 3 T in a group of 19 subjects [20]. From these grey matter cerebral blood flow maps cerebrovascular reactivity maps to isocapnic hypoxia were calculated showing the regional distribution of the cerebrovascular reactivity (Fig. 11.2). Cerebrovascular reactivity maps of isocapnic hypoxia showed very high intra-subject variations, some grey matter regions exhibiting a positive others a negative cerebrovascular reactivity. Seventy percent of subjects showed an overall positive cerebrovascular reactivity and the remaining 30 % of subjects an overall negative cerebrovascular reactivity (Fig. 11.3); per 10 % decrease in arterial oxygen saturation, cerebrovascular reactivity to isocapnic hypoxia resulted in a 10.7 ± 2.5 % increase in cerebral blood flow in positive and in a 9.0 ± 2.6 % decrease in negative responders.

(a) Quantitative grey matter cerebral blood flow maps from a single subject under isocapnia (ic) and isocapnic hypoxia (hx). Values are % change in cerebral blood flow per mmHg increase in PetCO2. (b) Quantitative map of cerebrovascular reactivity to hypoxia for the same subject as (a). Values are % change in cerebral blood flow per 10 % decrease in SaO2. Note both positive and negative values for cerebrovascular reactivity are present across the region. Modified from [20]

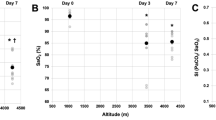
Grey matter cerebral blood flow values for individual subjects under normocapnia and hypercapnia (left) and isocapnia and hypoxia (right). Positive and negative responders are shown with solid and dotted lines respectively. The group mean ± cerebral blood flow values for all subjects (including both positive and negative responders) are also indicated (Reproduced from [20])
The high variability in hypoxic cerebrovascular reactivity between subjects could be due to conflicting physiological effects caused by hypoxia: vasodilatation and vasoconstriction. With low-level hypoxia, as applied in this study, both effects compete resulting either in an increase or a decrease of cerebral blood flow in single subjects depending on the overall dominant physiological effect in the subject studied. Also within individual subjects, there is a high variability in hypoxic cerebrovascular reactivity in grey matter; in some areas it is positive possibly indicating predominantly vasodilatation, in other regions it is negative indicating a vasoconstriction. At levels of hypoxia greater than those studied here, the vasodilator effect appears to dominate resulting in an increase in cerebral blood flow. We have also noted a vasoconstrictor effect of hypoxia in other studies from our laboratory that appear to be state dependent—this effect being prominent during slow wave sleep [16] and in the morning on awakening [17].
Recently Binks et al. [2] determined regional differences in the cerebrovascular response to moderate isocapnic hypoxia in cortical and subcortical grey matter using PET. Rather than applying an anatomical mask, white matter was excluded by applying an absolute threshold to the cerebral blood flow measurements. They reported that generally regions of interest with higher baseline perfusion exhibited increased responses to hypoxia. Interestingly, cortical grey matter showed below average increases in response to hypoxia and phylogenetically older regions of the brain (including the putamen, brain stem, thalamus, caudate nucleus, nucleus accumbens, and pallidum) tended to show larger vascular responses.
These two complementary studies strongly indicate that there are marked differences in the cerebrovascular responses to hypoxia, within and between brain regions and across subjects, The underlying reasons for these differences remains unclear but may well determine the pathophysiological responses to hypoxia and the degree of detriment to brain tissue.
5 Implications for Functional Brain Imaging Studies
Neuronal activation studies using functional brain imaging are problematic when the task or stimulus is associated with any changes in the arterial blood gases : any change in arterial blood gases will change global brain blood flow such that the local neurally related change in cerebral blood flow are correlated with the global change (see Fig. 11.4). In such circumstances it is therefore not possible to uniquely assign the change in local perfusion to being of neural origin. To address this we have developed paradigms for BOLD fMRI studies that dissociate the time course of the blood gas changes from the paradigm of interest and so dissociate the global perfusion signal from the local activation-related signals. This approach has had particular success in our study to determine the neural basis for voluntary breath holding [15]. Breath holding increases arterial PCO2, which consequently leads to a vasodilation of the cerebral circulation and a concomitant increase in whole-brain BOLD signal that is highly correlated with local, neurally induced, BOLD signal changes of interest. To address this caveat, PCO2 levels were manipulated throughout the experiment to dissociate the time course of the whole-brain BOLD signal from the time course of the local, neural-related BOLD signal; this allowed local activity associated with breath holding to be determined independent of whole-brain BOLD effects.

Flow diagram summarising the effect of increased arterial PCO2 and decreased arterial PO2 on the local BOLD fMRI signal , which in this example is associated with an increase in ventilation
This approach is generally applicable to studies in which either CO2 or O2 blood gas levels change. However, one assumption for this is that there are no substantial interactions between the blood gas changes and the vascular response to activation. Changes in such neurovascular coupling could over or under estimate the degree of activation associated with a particular experimental activation. A number of studies have investigated this issue for hypercapnia and as yet the relationship between whole-brain and regional blood flow is incompletely characterised. Some studies propose that the two signals are independent and additive [6, 13, 26], while others report an interaction with an attenuation [1, 3] or augmentation [24] of the regional BOLD signal.
We have tested for an interaction between hypoxia and hypercapnia and a visual stimulus that would produce robust BOLD signal increases within the occipital lobe (visual cortex). Statistical analyses were performed in order to characterize the presence of any interactions between the effects of hypercapnia and hypoxia on whole-brain blood flow, with local changes in cerebral blood flow associated with the visual stimulus (Fig. 11.5). A first analysis determined the main effects of the visual stimulus and included components to model the presence of an interaction between whole-brain BOLD signal fluctuations with the visually induced changes in regional BOLD signal. A second analysis modelled only the main effects of the visual stimulus and omitted the interaction terms of the first model. These analyses identified significant interactions between whole-brain BOLD signal changes induced by hypercapnia and hypoxia and the local neurally related BOLD signal associated with the visual stimulus. Hypercapnia decreased the response to the visual stimulus and hypoxia increased the response. However, physiologically the effects were weak and, in practice, they did not change the statistical outcome related to the analysis of the neurally related signals.

“Glass brain” projections (viewed from above) of statistically significant changes in the BOLD signal (SPM{f} corrected for multiple comparisons p < 0.05, n = 9). (a) main effect of hypercapnia, (b) main effect of hypoxia, (c) main effect of visual stimulation accounting for the effects of hypercapnia and hypoxia, (d) interaction of hypercapnia and the visual stimulus (e) interaction of hypoxia with the visual stimulus and (f) main effect of visual stimulation without accounting for the effects of hypercapnia and hypoxia. Note the substantial similarity of (c) and (e) indicating that the interaction between global vascular effects and the neurally related effects has a negligible effect on the determination of the functionally related changes
6 Conclusions
The regional grey matter cerebrovascular responses to hypercapnia and hypoxia both show regional variation. However, this variation appears to be substantially greater for hypoxia. The reasons underlying these regional differences are unclear but may determine local neuroprotective responses to perfusion-related insults. Correlation and interactions between global vascular changes due to hypoxia and hypercapnia and local neurally related vascular changes are a challenge to functional imaging studies. However, with appropriate study design, such respiratory-related confounds can be successfully accounted for.
References
Bandettini PA, Wong EC. A hypercapnia-based normalization method for improved spatial localization of human brain activation with fMRI. NMR Biomed. 1997;10:197–203.
Binks AP, Cunningham VJ, Adams L, Banzett RB. Gray matter blood flow change is unevenly distributed during moderate isocapnic hypoxia in humans. J Appl Physiol. 2008;104:212–7.
Bruhn H, Kleinschmidt A, Boecker H, Merboldt KD, Hanicke W, Frahm J. The effect of acetazolamide on regional cerebral blood oxygenation at rest and under stimulation as assessed by MRI. J Cereb Blood Flow Metab. 1994;14:742–8.
Buxton RB, Wong EC, Frank LR. Dynamics of blood flow and oxygenation changes during brain activation: the balloon model. Magn Reson Med. 1998;39:855–64.
Choi DW. Cerebral hypoxia—some new approaches and unanswered questions. J Neurosci. 1990;10:2493–501.
Corfield DR, Murphy K, Josephs O, Adams L, Turner R. Does hypercapnia-induced cerebral vasodilation modulate the hemodynamic response to neural activation? Neuroimage. 2001;13:1207–11.
Detre JA, Leigh JS, Williams DS, Koretsky AP. Perfusion imaging. Magn Reson Med. 1992;23:37–45.
Edelman RR, Siewert B, Darby DG, Thangaraj V, Nobre AC, Mesulam MM, Warach S. Qualitative mapping of cerebral blood-flow and functional localization with echo-planar MR-imaging and signal targeting with alternating radio-frequency. Radiology. 1994;192:513–20.
Hendrikse J, van Osch MJP, Rutgers DR, Bakker CJG, Kappelle LJ, Golay X, van der Grond J. Internal carotid artery occlusion assessed at pulsed arterial spin-labeling perfusion MR imaging at multiple delay times. Radiology. 2004;233:899–904.
Ito H, Yokoyama I, Iida H, Kinoshita T, Hatazawa J, Shimosegawa E, Okudera T, Kanno I. Regional differences in cerebral vascular response to PaCO2 changes in humans measured by positron emission tomography. J Cereb Blood Flow Metab. 2000;20:1264–70.
Johnson NA, Jahng GH, Weiner MW, Miller BL, Chui HC, Jagust WJ, Gorno-Tempini ML, Schuff N. Pattern of cerebral hypoperfusion in Alzheimer disease and mild cognitive impairment measured with arterial spin-labeling MR imaging: Initial experience. Radiology. 2005;234:851–9.
Kastrup A, Kruger G, Glover GH, Neumann-Haefelin T, Moseley ME. Regional variability of cerebral blood oxygenation response to hypercapnia. Neuroimage. 1999;10:675–81.
Li TQ, Kastrup A, Moseley ME, Glover GH. Changes in baseline cerebral blood flow in humans do not influence regional cerebral blood flow response to photic stimulation. J Magn Reson Imaging. 2000;12:757–62.
Luh WM, Wong EC, Bandettini PA, Ward BD, Hyde JS. Comparison of simul-taneously measured perfusion and BOLD signal increases during brain activation with T-1-based tissue identification. Magn Reson Med. 2000;44:137–43.
McKay LC, Adams L, Frackowiak RSJ, Corfield DR. A bilateral cortico-bulbar network associated with breath holding in humans, determined by functional magnetic resonance imaging. Neuroimage. 2008;40:1824–32.
Meadows GE, O’Driscoll DM, Simonds AK, Morrell MJ, Corfield DR. Cerebral blood flow response to isocapnic hypoxia during slow-wave sleep and wakefulness. J Appl Physiol. 2004;97:1343–8.
Meadows GE, Kotajima F, Vazir A, Kostikas K, Simonds AK, Morrell MJ, Corfield DR. Overnight changes in the cerebral vascular response to isocapnic hypoxia and hypercapnia in healthy humans—protection against stroke. Stroke. 2005;36:2367–72.
Morrell MJ, Meadows GE, Hastings P, Vazir A, Kostikas K, Simonds AK, Corfield DR. The effects of adaptive servo ventilation on cerebral vascular reactivity in patients with congestive heart failure and sleep-disordered breathing. Sleep. 2007;30:648–53.
Noeth U, Meadows GE, Kotajima F, Deichmann R, Corfield DR, Turner R. Cerebral vascular response to hypercapnia: determination with perfusion MRI at 1.5 and 3.0 Tesla using a pulsed arterial spin labeling technique. J Magn Reson Imaging. 2006;24:1229–35.
Noeth U, Kotajima F, Deichmann R, Turner R, Corfield DR. Mapping of the cerebral vascular response to hypoxia and hypercapnia using quantitative perfusion MRI at 3T. NMR Biomed. 2008;21:464–72.
Pagani M, Ansjon R, Lind F, Uusijarvi J, Sumen G, Jonsson C, Salmaso D, Jacobsson H, Larsson SA. Effects of acute hypobaric hypoxia on regional cerebral blood flow distribution: a single photon emission computed tomography study in humans. Acta Physiol Scand. 2000;168:377–83.
Pinard E, Mazoyer B, Verrey B, Pappata S, Crouzel C. Rapid measurement of regional cerebral blood-flow in the baboon using 15O-labeled water and dynamic positron emission tomography. Med Biol Eng Comput. 1993;31:495–502.
Placidi F, Diomedi M, Cupini LM, Bernardi G, Silvestrini M. Impairment of daytime cerebrovascular reactivity in patients with obstructive sleep apnoea syndrome. J Sleep Res. 1998;7:288–92.
Posse S, Kemna LJ, Elghahwagi B, Wiese S, Kiselev VG. Effect of graded hypo- and hypercapnia on fMRI contrast in visual cortex: quantification of T-2* changes by multiecho EPI. Magn Reson Med. 2001;46:264–71.
Poulin MJ, Robbins PA. Indexes of flow and cross-sectional area of the middle cerebral artery using Doppler ultrasound during hypoxia and hypercapnia in humans. Stroke. 1996;27:2244–50.
Ramsay SC, Murphy K, Shea SA, Friston KJ, Lammertsma AA, Clark JC, Adams L, Guz A, Frackowiak RSJ. Changes in global cerebral blood-flow in humans—effect on regional cerebral blood-flow during a neural activation task. J Physiol. 1993;471:521–34.
Rostrup E, Larsson HBW, Toft PB, Garde K, Henriksen O. Signal changes in gradient-echo images of human brain induced by hypoxia and hyperoxia. NMR Biomed. 1995;8:41–7.
Sicard KM, Duong TQ. Effects of hypoxia, hyperoxia, and hypercapnia on baseline and stimulus-evoked BOLD, CBF, and CMRO2 in spontaneously breathing animals. Neuroimage. 2005;25:850–8.
Silva AC, Kim SG. Perfusion-based functional magnetic resonance imaging. Concepts Magn Reson A. 2003;16A:16–27.
St Lawrence KS, Ye FQ, Lewis BK, Weinberger DR, Frank JA, McLaughlin AC. Effects of indomethacin on cerebral blood flow at rest and during hypercapnia: an arterial spin tagging study in humans. J Magn Reson Imaging. 2002;15:628–35.
Tuunanen PI, Kauppinen RA. Effects of oxygen saturation on BOLD and arterial spin labelling perfusion MRI signals studied in a motor activation task. Neuroimage. 2006;30:102–9.
Villringer A, Dirnagl U. Coupling of Brain activity and cerebral blood-flow—basis of functional neuroimaging. Cerebrovasc Brain Metab Rev. 1995;7:240–76.
Warmuth C, Gunther M, Zimmer C. Quantification of blood flow in brain tumors: comparison of arterial spin labeling and dynamic susceptibility-weighted contrast-enhanced MR imaging. Radiology. 2003;228:523–32.
Yang YH. Perfusion MR, imaging with pulsed arterial spin-labeling: basic principles and applications in functional brain imaging. Concepts Magn Reson. 2002;14:347–57.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York
About this chapter
Cite this chapter
Corfield, D.R., McKay, L.C. (2016). Regional Cerebrovascular Responses to Hypercapnia and Hypoxia. In: Roach, R., Hackett, P., Wagner, P. (eds) Hypoxia. Advances in Experimental Medicine and Biology, vol 903. Springer, Boston, MA. https://doi.org/10.1007/978-1-4899-7678-9_11
Download citation
DOI: https://doi.org/10.1007/978-1-4899-7678-9_11
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4899-7676-5
Online ISBN: 978-1-4899-7678-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)