
Abstract
Military personnel are at risk for the development of posttraumatic stress disorder. Although effective treatments are available, the need for improved treatment efficacy and less stigmatizing approaches to treatment have resulted in the evolution of virtual reality exposure therapy. This chapter reviews the development and dissemination efforts of a virtual reality system supporting exposure therapy for deployment-related posttraumatic stress disorder. Specifically, the chapter will review the work done to incorporate the feedback of military personnel into the early development of a Virtual Iraq/Afghanistan system and also reviews efforts to disseminate this treatment to military and Veteran behavioral health researchers and providers.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
US military operations in Iraq and Afghanistan have resulted in the deployment of millions of military service members (American Psychiatric Association, 2007). These deployments include inherent risks of exposure to combat and other potentially traumatic events (Hoge et al., 2004). Accordingly, research has found an increased risk of mental health disorders among military personnel (Hoge et al., 2004; Hoge, Auchterlonie, & Milliken, 2006; Milliken, Auchterlonie, & Hoge, 2007; Thomas et al., 2010). Rates of posttraumatic stress disorder (PTSD) have been particularly noteworthy. Studies have found that approximately 12–20 % of Army combat soldiers and Marines screen positive for the disorder following deployment (Hoge et al., 2004; Milliken et al., 2007; Thomas et al., 2010).
Fortunately, effective treatments are available. Cognitive behavioral treatments are among the most researched interventions and have robust evidence supporting their efficacy (American Psychiatric Association, 2004; Foa, Keane, Friedman, & Cohen, 2009). Among these treatments, exposure therapy in particular has received empirical support (Institute of Medicine, 2008; Powers, Halpern, Ferenschak, Gillihan, & Foa, 2010). However, based on smaller effect sizes for survivors of combat trauma (Bradley, Greene, Russ, Dutra, & Westen, 2005) and the need for treatment choices that can mitigate stigma (Reger & Gahm, 2008), innovative treatment options for military personnel have been pursued.
One promising innovative treatment is virtual reality exposure therapy (VRET). VRET is a form of exposure therapy that builds on emotional processing theory (Foa & Kozak, 1986) by seeking to leverage multisensory virtual reality stimuli that are relevant to the patient’s trauma memory in order to activate the related fear structure and modulate emotional engagement. Previous research shows preliminary support in the use of VRET to treat Vietnam veterans (Rothbaum, Hodges, Ready, Graap, & Alarcon, 2001), survivors of 9/11 (Difede et al., 2007), motor vehicle accidents (Beck, Palyo, Winer, Schwagler, & Ang, 2007), and active duty soldiers (Reger et al., 2011). However, at the time of this writing, there are no head-to-head randomized controlled trials comparing VRET to an evidence-based treatment for PTSD. Particular interest has been paid in recent years to the development of VRET systems that could be effectively used to treat service members with PTSD following deployments to Iraq and Afghanistan.
There are specific challenges related to the development and dissemination of any computer-based psychological intervention. First, the development of a useful and effective solution requires focused consideration of the end user, in this case the soldier, sailor, airman, or marine. Doing so requires the implementation of a user-centered approach to the design of the tool. Second, the technical and clinical skill set related to the use of the tool must be disseminated to those practitioners who need it. The most effective treatment in the world is of little value if it is not used by those conducting research on the treatment of patients with the disorder. This chapter reviews work done to incorporate the feedback of military personnel into the early development of a Virtual Iraq/Afghanistan system and also reviews efforts to disseminate this promising treatment to DoD and VA researchers and behavioral health providers.
Soldiers Reactions and Feedback
The fact that software developers believe a technology solution is useful has little relevance to the prediction of what end users will think (Barnum, 2002). User-centered design places the expected user of a technology, in this case the U.S. service member, at the heart of the design process (Rubin & Chisnell, 2008). Keeping the end user in mind during development helps to ensure that the solution being considered is wanted by users, is useful, efficient, effective, and is satisfactory (Barnum, 2002). Indeed, the gathering of user feedback should be repeated in an iterative fashion; doing so helps to ensure that the limited resources available will be applied in a fashion that will meet the defined needs. The current economic landscape demands efficient use of resources and a user-centered approach is essential to cost-effective execution (Nielsen, 1994). When usability is not taken into account, technology solutions frustrate, developed health interventions are not used, resources are wasted, and ultimately, military personnel do not receive the help they need.
User feedback may be particularly important for a trauma-focused psychological intervention. Exposure-based treatments aim to activate a theoretically optimal level of emotional engagement (Foa, Huppert, & Cahill, 2006). This is accomplished by asking the patient to confront difficult memories and feared situations/circumstances in their day-to-day lives (Foa, Hembree, & Rothbaum, 2007). Accordingly, exposure is inherently difficult for the patient. A minority of patients actually experience a temporary symptom exacerbation prior to improvement (Foa, Zoellner, Feeny, Hembree, & Alvarez-Conrad, 2002). Incorporating a poorly designed virtual reality tool that augments exposure with multisensory cues could increase emotional engagement and discomfort to the point that new learning is not taking place. Alternatively, the video game like appearance of a virtual environment may not represent the highly emotional combat trauma with enough fidelity to activate the fear structure. If unrealistic, VRET could distract the patient from their memory, decrease emotional engagement, and possibly reduce clinical outcomes. Similarly, although VRET is presumed to offer an appealing form of treatment for a young, technologically savvy population of military personnel (Reger, Gahm, Rizzo, Swanson, & Duma, 2009), without user feedback the developed environments may be judged negatively by patients, potentially impacting decisions to access care, rates of treatment compliance, or treatment satisfaction.
Feedback from Deployed Soldiers
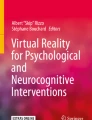
In March 2005, the first author was assigned to a combat stress control detachment that deployed in support of Operation Iraqi Freedom. Shortly after the initiation of this deployment, a portable prototype Virtual Iraq system was acquired and shipped into theater. The system included two XPS Dell notebook computers, a head-mounted display (HMD) with head orientation tracking, a USB gaming joystick, and a crossover cable to connect the two computers. One of these computers delivered the virtual environment to the HMD that the patient interacted with and the other computer enabled a clinician’s interface that allowed real time customization of the virtual environment in order to match a trauma memory. The Virtual Iraq software was at an early stage of development and the purpose of sending the system to Iraq was to obtain feedback from service members actually located in the country represented by the virtual environment. In addition, the delivery of timely, exposure-based treatments to personnel who are still deployed is of growing interest (Cigrang, Peterson, & Schobitz, 2005; McLay, McBrien, Wiederhold, & Wiederhold, 2010). Although no VRET was delivered in theater, we were interested in the durability of the computer hardware and VR peripherals in an austere environment as well as the relevance of graphic imagery delivered by the system (See Fig. 15.1).

Virtual Iraq prototype system, circa 2004–2005
Dozens of deployed soldiers used the environment (see Fig. 15.2) and were asked to provide feedback and recommendations for improvement. Initial feedback suggested general satisfaction with the realism of the auditory stimuli based on their deployment experiences. However, soldiers recommended three-dimensional sounds that would adjust according to head movements or location (e.g., when located in a virtual building interior). Soldiers also recommended that auditory stimuli representing small arms fire include a representation of impact with a vehicle or building.

SM User in Iraq experiencing virtual Iraq and providing feedback
Problematic features of the Virtual Iraq were also identified. For example, unrealistic visual intrusions distracted users from a sense of realistic participation. An Iraqi voice saying the unrealistic phrase “Go home cowboy!,” unrealistic Saddam statue, geographically dispersed building structures instead of clusters of structures with miles of vacant desert, too many destroyed vehicles, and too many clouds in the sky were all potential distractions. On the other hand, certain expected stimuli were noted to be absent. For example, soldiers reported that the Virtual Iraq would better represent their experience if it included significant civilian traffic and more pedestrians, clusters of garbage on sides of the road, and children begging. The addition of animals (dead and alive), improvised explosive devices, crowds of teenage rock throwers, and the ability to drive on the opposite side of the road were also recommended.
Similarly, deployed soldiers did not like the navigation available at that time. Soldiers found foot patrol movement in the city environment somewhat awkward as it required the user to look in the direction he or she wanted to move. This resulted in unusual and strained head positions to navigate to the desired destination. Soldiers were also frustrated by the inability to steer the vehicle in the convoy or adjust speed of movement in both scenarios. Although some of these recommendations were not surprising given the early stage of development, the soldiers’ feedback was helpful for the development team to prioritize their efforts and avoid wasting limited resources on features irrelevant to intended users.
Feedback from Previously Deployed Soldiers
Based on the need for continued, iterative soldier feedback and a desire to formalize a data collection methodology, the authors launched a study of previously deployed soldiers’ feedback (Reger et al., 2009) of the evolving Virtual Iraq/Afghanistan VRET system, the design of which was informed by the initial feedback from soldiers in Iraq. Soldiers who had been home from Iraq or Afghanistan for less than a year were recruited to use and evaluate the current system.
The Virtual Iraq/Afghanistan application developed at the time (2006–2007) comprised of a series of virtual scenarios including a Middle-East themed city and roadway environments (See Fig. 15.3). The scenarios were designed to resemble the general contexts that most SMs would have experienced during a deployment to Iraq or Afghanistan. The 18-square block City setting had a variety of elements including a marketplace, desolate streets, old buildings, ramshackle apartments, warehouses, mosques, shops, and dirt lots strewn with junk. Access to building interiors and rooftops was available and the backdrop surrounding the navigable exposure zone created the illusion of being embedded within a section of a sprawling densely populated desert city. Vehicles were active in streets and animated virtual pedestrians (civilian and military) could be added or eliminated from the scenes. Users could be teleported to specific locations within the city, based on a determination as to which environments most closely matched their experiences.

Virtual Iraq/Afghanistan system, circa 2007, Middle Eastern City and driving scenarios
The Iraq Desert road scenario consisted of a roadway through an expansive desert area with sand dunes, occasional areas of vegetation, intact and broken down structures, bridges, battle wreckage, a checkpoint, debris, and virtual human figures. The system also had an Afghanistan-themed road scenario that contained similar elements but within a more mountainous terrain context that included Afghan style architectural and cultural elements. In both the Iraq and Afghanistan roadways, the user could be positioned inside of a HUMVEE that supported the perception of travel within a convoy or as a lone vehicle with selectable positions as a driver, passenger, or from the more exposed turret position above the roof of the vehicle. Both the city and HUMVEE scenarios were adjustable for time of day or night, weather conditions, night vision, illumination, and ambient sound (wind, motors, city noise, prayer call, etc.). Users could navigate in both scenarios via the use of a standard gamepad controller.
In addition to the visual stimuli presented in the VR Head-Mounted Display (HMD), directional 3D audio, vibrotactile and olfactory stimuli could be delivered into the VR scenarios in real time by the clinician. The presentation of additive, combat-relevant stimuli in the VR scenarios could be controlled via a “Wizard of Oz” control panel, while the clinician was in full audio contact with the patient. This clinical “interface” provided the clinician with the capacity to customize the therapy experience to the individual needs of the patient. The patient could be placed by the clinician in VR scenario locations that resembled a setting relevant to their trauma experience and modify ambient light and sound conditions to match the patient’s description of their experience. The interface also allowed the clinician to gradually introduce and control trigger stimuli in real time to foster the anxiety modulation needed for therapeutic habituation and emotional processing in a customized fashion according to the patient’s past experience and treatment progress. Such options for real time stimulus delivery flexibility and user experience customization were considered to be key elements for this application. Trigger stimuli included a variety of auditory stimuli (e.g., incoming mortars, weapons fire, voices, wind), dynamic audiovisual events including helicopter flyovers, bridge attacks, exploding vehicles and IEDs, and olfactory stimuli (e.g., burning rubber, gunpowder, garbage, diesel fuel). In contrast to the VR system taken to Iraq, this study added a platform with bass shaker speakers. These speakers enabled low frequency sounds (e.g., virtual explosions or the idle of the vehicle) to also be experienced as vibrations by participants.
Soldiers responded to a series of likert scale items ranging from 1 (poor) to 10 (excellent), with the midpoint of 5 representing an adequate rating. Ninety-three soldiers provided feedback. Although the average evaluation was between adequate and excellent for all rated aspects (see Table 15.1), additional needed improvements were identified. For example, soldiers felt it was unrealistic to stand on a platform and navigate in a foot patrol scenario holding a gaming joystick. A number of participants reported that realism would be enhanced if they were holding their weapon. Both environments were judged too clean. Soldiers recommended more debris, dirt, and garbage. Soldiers also found it unrealistic to be seated in a virtual vehicle or walking through an Iraqi city alone. They requested the presence of additional soldiers. Additional Iraqi civilian pedestrians were requested and the possibility of more congested traffic was recommended. Soldiers also suggested the development of a library of tactical vehicles and weapons that could be selected based on the personal experience of the soldier.
The Resulting Virtual Iraq/Afghanistan System
These two efforts resulted in a number of key improvements to the Virtual Iraq/Afghanistan system. Changes included the adaptation of a mock M4 rifle with a mounted mini joystick, allowing soldiers to navigate through the virtual city in a naturalistic fashion, while holding the physical prop of a realistic weapon. Truck commanders, turret gunners, and passengers were added and both environments were improved with additional pedestrian and vehicle traffic. Among other improvements, recommendations regarding the inclusion of animal carcasses, dirt, and garbage were implemented.
Feedback received from the intended end users was essential to the development of a useful Virtual Iraq/Afghanistan system. More importantly, the development of an improved system enabled successful treatment protocol development and clinical application. The VR Iraq/Afghanistan system has been used for the effective exposure therapy treatment of members of the National Guard (Gerardi, Rothbaum, Ressler, Heekin, & Rizzo, 2008) as well as active component soldiers (Reger et al., 2011; Reger & Gahm, 2008; Rizzo et al., 2011). Well-designed randomized controlled trials are currently underway to determine the efficacy of VRET relative to existing standards of care. Based on the initial success of the use of this approach for the delivery of exposure therapy using VR, the U.S. Department of Defense has funded the development of an updated and expanded version of the Virtual Iraq/Afghanistan system built from currently available software. This work will be detailed in the chapter by Rizzo et al. (2014) in this volume.
Dissemination of Virtual Reality Exposure in the Treatment of PTSD
Change is difficult. This appears to be as true of mental health practitioners as anyone. Research has demonstrated that adoption of evidence-based psychotherapies by clinicians is slow, despite significant research supporting efficacy (Frueh, Grubaugh, Cusack, & Elhai, 2009). A survey of 207 licensed psychologists found that only 9 % reported using imaginal exposure with 50 % or more of their PTSD patients (Becker, Zayfert, & Anderson, 2004). The primary factor limiting use of imaginal exposure was limited training (Becker et al., 2004). Similarly, when 296 trauma experts were asked to what extent they agreed with the statement that they had received good training in imaginal exposure, their average response was lukewarm. On a scale from 1 to 10, with 10 representing strong agreement, the average response was 3.76 (SD = 3.03, van Minnen, Hendriks, & Olff, 2010). It is not surprising that only a minority of these therapists used exposure to treat their PTSD patients.
Development of a new, promising innovative treatment does not guarantee adoption and implementation, even by interested early adopters and researchers. Adequate training is required. Furthermore, researchers or clinicians seeking to study or implement VRET need training to build on existing best practices. In October 2008, we had received enough requests for VRET training that we began hosting clinical training workshops to assist Veterans Administration (VA) and Department of Defense (DoD) researchers and providers who were seeking to learn current best practices for this promising emerging treatment.
The training approach was carefully considered with an eye towards the likely audience, necessary prerequisite knowledge, and common factors affecting implementation (Ruzek & Rosen, 2009). According to Fixsen and colleagues, as cited in Ruzek and Rosen (2009), the impact of training workshops increases when skill demonstration and rehearsal are included. We also wanted to build in opportunities for post-training consultation and supervision to support an ethical model of new skill acquisition (American Psychological Association, 2002) and to assist with post-training consolidation of learned skills (Ruzek & Rosen, 2009).
The resulting VRET training program included the prerequisite that attendees have prior formal training in prolonged exposure. This requirement was established because the skills necessary for the VRET treatment protocol (Rothbaum, Difede, & Rizzo, 2008) resemble many of those required by other exposure therapy protocols (Foa et al., 2007). Foundational exposure therapy skills were judged essential as a prerequisite for training competent VRET therapists. The workshops were also planned to dedicate significant time to demonstrations of VRET skills and hands-on rehearsal. Over the course of a 2-day workshop, as much as half of the training time is dedicated to hands-on experience with the Virtual Iraq/Afghanistan software, virtual reality hardware, trouble shooting, and role plays with faculty and other students. Trainees are divided into breakout groups of approximately five trainees and one faculty member to rehearse the instructed skills. Finally, from the outset we included the opportunity for 6 months of weekly telephone consultation with faculty.
At the time of writing, we have hosted seven training workshops, which have disseminated VRET to 148 individuals from 35 locations. Providers from all three military services and the VA have been trained (Fig. 15.4). Trainees have included primarily psychologists, although social workers and psychiatrists have also attended. All workshops included student evaluations as part of the continuing education program evaluation. Over this period of time, the institutional survey items have unfortunately changed but 6 of the 7 workshops had key items that remained constant.

Organizational and service representation of VRET trainees (N = 148)
As is evident in Table 15.2, the trainings have been very well regarded by the trained clinicians. The vast majority of workshop attendees found the training relevant, worthwhile, and well instructed. The fact that 96 % of attendees “strongly agreed” (5/5 on a 5-point likert item) that they would recommend the training to their peers speaks volumes about the perceived value by those in attendance.
To support the program evaluation of the longer term impact of the workshops, attendees were provided a brief survey 6 months following each training. Specifically, we were interested in whether trained clinicians were using or planning to use VRET in research or clinical practice. To date, we have followed up with 107 of the 148 trained clinicians. Of these, we received responses from 67 (63 % response rate). The results were somewhat disheartening (see Table 15.3). Although slightly more than half of the previous participants who responded had the computer hardware and peripherals to use VRET, only a small percentage of prior trainees had used VRET in research or clinical practice 6-month post-training. Relative to their reported current use, prior trainees reported moderately higher rates of planned VRET use. It is not known what proportion of these plans were carried out.
Our program evaluation did not ask providers to identify barriers to implementation. However, our experience across these training efforts suggests a number of likely factors that could be considered. First, VRET requires acquisition of computer hardware and related VR equipment. The cost of this equipment has decreased significantly in recent years (Rizzo et al., 2011). Regardless, in a challenging economic landscape, implementation of VRET in a VA or DoD organization requires purchasing equipment within a context of already strained budgets. Indeed, our program evaluation found that 39 % of previous trainees did not have the equipment necessary for VRET 6-month post-training. It is possible that current requests for budget increases are not likely to be supported and some managers may have been unwilling to invest in VRET.
Second, the current absence of randomized controlled trials of VRET relative to other PTSD treatment options impedes evaluations of the return on investment for this treatment choice. Although research has demonstrated the effectiveness of VRET (Difede et al., 2007; Reger et al., 2011; Reger & Gahm, 2008; Rizzo, Difede, Rothbaum, & Reger, 2010; Rothbaum et al., 2001) and VRET appears to be a more appealing treatment than traditional approaches for some soldiers (Wilson, Onorati, Mishkind, Reger, & Gahm, 2008), responsible cost-benefit analysis cannot currently be conducted based on the existing literature. Quality head-to-head clinical trials are needed.
Third, based on the requests for VRET training we received, we expected research to make up a significant proportion of post-training VRET use. The fact that this was not the case within 6-months is perhaps not surprising. The writing, review, and approval of research grants and protocols by funding agencies and Institutional Review Boards can be a lengthy process. We understand that this is particularly true for some VA and DoD researchers. Several former trainees who reported planned research noted that the process had been started but was early in development or still under review. Such administration processes can be a particularly time consuming process for providers who are not allocated any dedicated research hours.
Fourth, implementation of new PTSD training is often impacted by system factors (Ruzek & Rosen, 2009). Previous researchers identified barriers to the implementation of PTSD treatments in public sector settings (Frueh et al., 2009), which may be relevant to the current discussion. For example, high patient case loads, too few clinicians, and inadequate knowledge of PTSD and its treatment among supervisors and administrators can all affect implementation (Frueh et al., 2009). Although we do not have an assessment of trainee’s system support for VRET, it is noteworthy that the opportunity for weekly consultation with the faculty was only rarely accessed. It was not unusual to have only one or two trainees take advantage of this consultation, even though the vast majority of trainees rated the teaching of the faculty as excellent (see Table 15.2). It may be that the priority for rapid access to care for service members and veterans and a shortage of behavioral health providers in these organizations resulted in clinician schedules dedicated to patient care as opposed to consolidation of new skills.
Finally, although it may be surprising to some readers, a number of trained clinicians reported limited opportunities to treat PTSD. Service-related differences in mission may affect the population risk of exposure to deployment-related trauma. Several Air Force clinicians stated that they had not encountered many cases of PTSD in their clinic and had not been able to use VRET despite their intentions.
Conclusions
Virtual reality opens up revolutionary potential to transform psychological education, training, assessment, and treatment. Military personnel are active consumers of personal technologies (Bush, Fullerton, Crumpton, Metzger-Abamukong, & Fantelli, 2012) and service members present a patient population that is well suited to the adoption of innovative technology treatments. VRET in particular offers the promising capability to deliver customized virtual environments to support the exposure therapy of service members with PTSD. This innovative tool is consistent with current theories of PTSD acquisition and treatment (Foa & Kozak, 1986) and is showing promise in the research literature. However, as a relatively new technology tool, it faces a mix of new and old challenges.
Psychologists are not software developers or engineers and the discussion of user feedback above highlights the inherently multidisciplinary nature of work in VRET. As innovative psychologists continue to seek creative solutions that leverage virtual reality, they must reach out to partner with others that have a range of skill sets, including expertise in interface design, user experience, software development, usability, and ergonomics to name a few. Overlooking this need could be costly. Failure to incorporate end user considerations into the design from the outset will result in frustrations, delays, and failures. Engaging this challenge, however, can create new, better ideas and improved tools and solutions. This engagement will push creative behavioral health providers and researchers out of their clinics and labs and into the realms of other disciplines. This requires a teachable spirit and humility. The expert behavioral health provider is a neophyte in these new disciplines. However, the synergy potentially created by these multidisciplinary collaborations sets the stage for a new era in the psychological support of service members.
Unfortunately, the longstanding challenge of dissemination and implementation of any PTSD treatment also persists. To date, dissemination of VRET has been primarily to support early adopters of an emerging treatment and to support researchers seeking to study this promising, innovative approach. If current randomized controlled trials find VRET to be as effective as existing standards of care (or more effective), dissemination could become a more urgent issue. If this comes to pass, the dissemination efforts discussed above suggest the need for careful attention to prior lessons learned in PTSD treatment dissemination (Frueh et al., 2009; Karlin et al., 2010; Ruzek & Rosen, 2009).
References
American Psychiatric Association. (2002). Ethical principles of psychologists and code of conduct. Retrieved September 28, 2011, from http://www.apa.org/ethics/code/index.aspx
American Psychiatric Association. (2004). Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder. Washington, D.C.: American Psychiatric Association.
American Psychiatric Association. (2007). The psychological needs of U.S. military service members and their families: A preliminary report. Retrieved September 30, 2011, from http://www.ptsd.ne.gov/publications/military-deployment-task-force-report.pdf
Barnum, C. M. (2002). Usability testing and research. New York: Longman.
Beck, J. G., Palyo, S. A., Winer, E. H., Schwagler, B. E., & Ang, E. J. (2007). Virtual reality exposure therapy for PTSD symptoms after a road accident: An uncontrolled case series. Behavior Therapy, 38(1), 39–48.
Becker, C. B., Zayfert, C., & Anderson, E. (2004). A survey of psychologists’ attitudes towards and utilization of exposure therapy for PTSD. Behaviour Research and Therapy, 42(3), 277–292.
Bradley, R., Greene, J., Russ, E., Dutra, L., & Westen, D. (2005). A multidimensional meta-analysis of psychotherapy for PTSD. The American Journal of Psychiatry, 162(2), 214–227.
Bush, N., Fullerton, N., Crumpton, R., Metzger-Abamukong, M., & Fantelli, E. (2012). Soldiers’ personal technologies on deployment and at home. Telemedicine and e-Health, 18, 253–263.
Cigrang, J. A., Peterson, A. L., & Schobitz, R. P. (2005). Three American troops in Iraq: Evaluation of a brief exposure therapy treatment for the secondary prevention of combat-related PTSD. Pragmatic Case Studies in Psychotherapy, 1(2), 1–25.
Difede, J., Cukor, J., Jayasinghe, N., Patt, I., Jedel, S., Spielman, L., et al. (2007). Virtual reality exposure therapy for the treatment of posttraumatic stress disorder following September 11, 2001. Journal of Clinical Psychiatry, 68(11), 1639–1647.
Foa, E. B., Huppert, J. D., & Cahill, S. P. (2006). Emotional processing theory: An update, In B.O. Rothbaum (Ed.), Pathological Anxiety (3–24). New York: Guilford.
Foa, E. B., Hembree, E. A., & Rothbaum, B. O. (2007). Prolonged exposure therapy for PTSD: Emotional processing of traumatic experiences: Therapist guide. New York, NY: Oxford University Press.
Foa, E. B., Keane, T. M., Friedman, M. J., & Cohen, J. A. (Eds.). (2009). Effective treatments for PTSD: Practice guidelines from the international society for traumatic stress studies. New York: Guilford Press.
Foa, E. B., & Kozak, M. J. (1986). Emotional processing of fear: Exposure to corrective information. Psychological Bulletin, 99(1), 20–35.
Foa, E. B., Zoellner, L. A., Feeny, N. C., Hembree, E. A., & Alvarez-Conrad, J. (2002). Does imaginal exposure exacerbate PTSD symptoms? Journal of Consulting and Clinical Psychology, 70(4), 1022–1028.
Frueh, B. C., Grubaugh, A. L., Cusack, K. J., & Elhai, J. D. (2009). Disseminating evidence-based practices for adults with PTSD and severe mental illness in public-sector mental health agencies. Behavior Modification, 33(1), 66–81.
Gerardi, M., Rothbaum, B. O., Ressler, K., Heekin, M., & Rizzo, A. (2008). Virtual reality exposure therapy using a virtual Iraq: Case report. Journal of Traumatic Stress, 21(2), 209–213.
Hoge, C. W., Auchterlonie, J. L., & Milliken, C. S. (2006). Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. Journal of the American Medical Association, 295(9), 1023–1032.
Hoge, C. W., Castro, C. A., Messer, S. C., McGurk, D., Cotting, D. I., & Koffman, R. L. (2004). Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. The New England Journal of Medicine, 351(1), 13–22.
Institute of Medicine. (2008). Treatment of posttraumatic stress disorder: An assessment of the evidence. Washington, DC: National Academies Press.
Karlin, B. E., Ruzek, J. I., Chard, K. M., Eftekhari, A., Monson, C. M., Hembree, E. A., et al. (2010). Dissemination of evidence-based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. Journal of Traumatic Stress, 23(6), 663–673.
McLay, R. N., McBrien, C., Wiederhold, M. D., & Wiederhold, B. K. (2010). Exposure therapy with and without virtual reality to treat PTSD while in the combat theater: A parallel case series. Cyberpsychology, Behavior and Social Networking, 13(1), 37–42.
Milliken, C. S., Auchterlonie, J. L., & Hoge, C. W. (2007). Longitudinal assessment of mental health problems among active and reserve component soldiers returning from the Iraq war. Journal of the American Medical Association, 298(18), 2141–2148.
Nielsen, J. (1994). Guerrilla HCI: Using discount usability engineering to penetrate the intimidation barrier. Retrieved September 15, 2011, from http://www.useit.com/papers/guerrilla_hci.html
Powers, M. B., Halpern, J. M., Ferenschak, M. P., Gillihan, S. J., & Foa, E. B. (2010). A meta-analytic review of prolonged exposure for posttraumatic stress disorder. Clinical Psychology Review, 30(6), 635–641.
Reger, G. M., & Gahm, G. A. (2008). Virtual reality exposure therapy for active duty soldiers. Journal of Clinical Psychology, 64(8), 940–946.
Reger, G. M., Gahm, G. A., Rizzo, A. A., Swanson, R., & Duma, S. (2009). Soldier evaluation of the virtual reality Iraq. Telemedicine Journal and E-Health: The Official Journal of the American Telemedicine Association, 15(1), 101–104.
Reger, G. M., Holloway, K. M., Candy, C., Rothbaum, B. O., Difede, J., Rizzo, A. A., et al. (2011). Effectiveness of virtual reality exposure therapy for active duty soldiers in a military mental health clinic. Journal of Traumatic Stress, 24(1), 93–96.
Rizzo, A., Difede, J., Rothbaum, B. O., & Reger, G. (2010). Virtual Iraq/Afghanistan: Development and early evaluation of a virtual reality exposure therapy system for combat-related PTSD. Annals of the New York Academy of Sciences, 1208, 114–125.
Rizzo, A., Parsons, T. D., Lange, B., Kenny, P., Buckwalter, J. G., Rothbaum, B., et al. (2011). Virtual reality goes to war: A brief review of the future of military behavioral healthcare. Journal of Clinical Psychology in Medical Settings, 18(2), 176–187.
Rothbaum, B. O., Difede, J., & Rizzo, A. A. (2008). Therapist treatment manual for virtual reality expsoure therapy: Posttraumatic stress disroder in Iraq combat vetnerans. Atlanta: Virtually Better.
Rothbaum, B. O., Hodges, L. F., Ready, D., Graap, K., & Alarcon, R. D. (2001). Virtual reality exposure therapy for Vietnam veterans with posttraumatic stress disorder. Journal of Clinical Psychiatry, 62(8), 617–622.
Rubin, J., & Chisnell, D. (2008). Handbook of usability testing. Indianapolis: Wiley.
Ruzek, J. I., & Rosen, R. C. (2009). Disseminating evidence-based treatments for PTSD in organizational settings: A high priority focus area. Behaviour Research and Therapy, 47(11), 980–989.
Thomas, J. L., Wilk, J. E., Riviere, L. A., McGurk, D., Castro, C. A., & Hoge, C. W. (2010). Prevalence of mental health problems and functional impairment among Active Component and National Guard soldiers 3 and 12 months following combat in Iraq. Archives of General Psychiatry, 67(6), 614–623.
van Minnen, A., Hendriks, L., & Olff, M. (2010). When do trauma experts choose exposure therapy for PTSD patients? A controlled study of therapist and patient factors. Behaviour Research and Therapy, 48(4), 312–320.
Wilson, J. A. B., Onorati, K., Mishkind, M., Reger, M. A., & Gahm, G. A. (2008). Soldier attitudes about technology-based approaches to mental health care. CyberPsychology and Behavior, 11(6), 767–769.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Additional information
DOD Disclaimer:
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Department of the Army or the Department of Defense.
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Reger, G.M., Rizzo, A.A., Gahm, G.A. (2015). Initial Development and Dissemination of Virtual Reality Exposure Therapy for Combat-Related PTSD. In: Safir, M., Wallach, H., Rizzo, A. (eds) Future Directions in Post-Traumatic Stress Disorder. Springer, Boston, MA. https://doi.org/10.1007/978-1-4899-7522-5_15
Download citation
DOI: https://doi.org/10.1007/978-1-4899-7522-5_15
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4899-7521-8
Online ISBN: 978-1-4899-7522-5
eBook Packages: Behavioral ScienceBehavioral Science and Psychology (R0)