
Abstract
Since the emergence of Marburg virus in 1967 and Ebola viruses in 1976 the history of the disease, outbreaks and the viruses has been hindered by the episodic nature of their appearance and the restrictions of working with these high hazard pathogens. More recent outbreaks have facilitated more in depth study of the epidemiology of the viruses and have allowed a better understanding of the nature of transmission of the virus. Similarly more recent intensive laboratory study of the viruses and the disease they cause in laboratory animals has revealed much of the molecular basis of their high pathogenicity as well as the development of vaccines and other medical countermeasures. The reservoir host for Marburg virus has now been revealed and efforts continue to determine the zoonotic source for Ebola viruses. Tables and Maps of Marburg and Ebola virus outbreaks are presented.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Personal Protective Equipment
- Indirect Fluorescent Antibody Test
- Marburg Virus
- Medical Care Facility
- Medical Countermeasure
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Historical Overview
Because of the inordinate media attention given to the filoviruses, particularly Ebola virus, a brief historical overview is in order.
1.1 Marburg Virus
In 1967 the first known appearance of the filoviruses occurred in Germany (Marburg and Frankfurt) and Yugoslavia (Belgrade) [1, 2]. The disease was associated with the import of green monkeys (Cercopithecus aethiops, now Chlorocebus aethiops) from Uganda as a source of monkey kidney cells for the manufacture of polio virus vaccine. There were 29 cases who had direct contact with the monkeys or tissues from the monkeys and an additional 6 cases among individuals who had contact with the initial patients. Seven fatalities occurred, all among the individuals with exposure to the primates or their tissues. The disease was initially called green monkey disease and the virus named after the town, Marburg, in which the initial cases were noted.
Over the ensuing months the virus was isolated by serial passage in guinea pigs and also produced disease in two species of monkey (Chlorocebus aethiops and Macaca mulatta) [3]. Interestingly, early reports suggested that there were no cytopathic effects in a variety of cell cultures, while there was suggestion of replication in the cultures by inoculation of guinea pigs with supernatant fluids of the cultures. Later reports do indicate the presence of cytopathic effect in a number of cell lines.
The virus had a distinct, long pleomorphic appearance in electron micrographs; this trait would eventually give the name to the family to which the virus belongs, the Filoviridae, because of the filamentous appearance of the virus.
Marburg virus appeared again in 1975 when a young Australian man, touring with his female companion in Southern Africa, became ill in South Africa after visiting Rhodesia (now Zimbabwe). He was hospitalized in Johannesburg 4 days after onset of illness and died there with rash and significant bleeding after 4 days of hospitalization. His companion, who remained at the side of the initial case constantly throughout his early illness and hospitalization, became ill 2 days after the death of the index case as did a nurse caring for him, 8 days after the death of the initial case. The companion and the nurse survived their infections [4]. The exact origin of the infection of the index patient was not clearly elucidated in the subsequent investigations [5].
2 The Dawn of Ebola Virus
In 1976 two outbreaks of a disease with similar signs and symptoms occurred more or less simultaneously in north central Zaire (now the Democratic Republic of the Congo or DRC) and in southern Sudan [6–8]. The outbreaks were larger than the initial Marburg incidents and were clearly comprised of chains of person-to-person transmission following the introduction of the infection into medical care facilities. The reuse of needles and syringes without proper sterilization was eventually thought to play a role in much of the transmission from patient to patient, at least within medical care facilities, in these outbreaks.
Material from patients was sent to a number of international laboratories, and it was soon discovered to be related to Marburg virus by its similar appearance in electron micrographs. In spite of the similarity of the appearance between Marburg virus and this new virus, there was no serological cross-reaction when reference sera from Marburg virus were reacted with this newer one or laboratory animals were cross-challenged [9].
Field investigations of the Zaire and Sudan outbreaks did not yield evidence of a direct link between the outbreaks at the two locations. The virus was given the name Ebola virus after a river that is near the site of the original outbreak in Zaire. There was a single case in Zaire in 1977 [10] and another small outbreak in southern Sudan in 1979 [11, 12]. The viruses causing the outbreaks in Zaire and the outbreaks in Sudan are in fact quite distinct; however, they were not determined to be separate viruses until the early 1980s when a radioimmunoassay suggested that antibodies to the two viruses could distinguish between them [13] and then molecular biology had reached some ability to distinguish the two viruses from each other [14]. Following the 1979 outbreak in southern Sudan, there were no reported African outbreaks until 1995 when the outbreak in Kikwit, Zaire, occurred.
In 1989 Ebola virus came to the USA in, similar to the circumstances for Marburg virus in 1967 in Europe, in monkeys (cynomolgus macaques, Macaca fascicularis) in quarantine in Reston, Virginia, that were being imported for biomedical research into the USA from the Philippines. The monkeys were found to be dying of Ebola virus, although a second virus, Simian hemorrhagic fever virus, was also present [15]. By 1989, the ability of molecular biology to sequence and determine the relationships of viruses more easily indicated that this was a novel Ebola virus, given the name Ebola Reston, related but distinct from the two strains which had been the etiology of the Zaire and Sudan outbreaks in the 1970s, Ebola Zaire and Ebola Sudan. The outbreak was traced back to a facility in the Philippines where the imported monkeys had originated [16, 17]. There were to be further instances of monkeys from this same facility being infected with Ebola Reston, including 1992 into Italy [18, 19] and 1996 into the USA once more [20].
In 1994, a fourth Ebola virus, Ebola Ivory Coast, emerged when a female scientist studying mortality among chimpanzees in the Tai Forest National Park in Ivory Coast became ill following a postmortem exam that she had performed upon a chimp that had died. Her illness was a dengue-like syndrome, and the virus was isolated from her blood [21]. Serological testing at the Institute Pasteur in Paris and sequencing soon demonstrated that this was another novel Ebola virus.
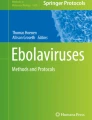
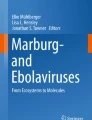
Starting in the mid-1990s the number of Ebola virus outbreaks was more frequent and precludes individual discussion. Some of these outbreaks will be discussed in the context of their contribution to our knowledge of the diseases and viruses, but a complete listing of the occurrence of known outbreaks can be found in Table 14.1 (Marburg) and Table 14.2 (Ebola viruses). The relative size of each of these outbreaks and its location can also be seen in maps provided in Fig. 14.1 (Marburg) and Fig. 14.2 (Ebola).

Map of African Marburg virus outbreaks and year in which they occurred. The circles are proportional to the number of cases in the outbreak (see Table 14.1 for the number of cases). Note that the 1980 date obscures the date of the 1987 case, both of which originated at the same location, Kitum Cave on Mt. Elgon. The 1998 outbreak in DRC was actually a series of small outbreaks associated with a mine near the village of Durba which continued through 2000

Map of African Ebola virus outbreaks and the year in which each occurred. The circles are proportional to the number of cases in the outbreak (see Table 14.2 for the number of cases). The color of circles indicates which Ebola virus caused the outbreak: Ebola Zaire (red), Ebola Sudan (burnt orange), and Ebola Bundibugyo (blue). In order to show sufficient detail of the area in which the majority of outbreaks have occurred, the 1994 single case of Ebola Ivory Coast is not shown, and the 1996 South African imported case of Ebola Zaire is not shown. The 1976, 1979, and 2004 Ebola Sudan outbreaks overlap each other and the dates are obscured in the figure
Briefly, a fifth Ebola virus was discovered in late 2007 when an outbreak in western Uganda turned out to be caused by another novel and distinct virus, now known as Ebola Bundibugyo, after the Ugandan town in which the outbreak it caused was centered. Although next-generation sequencing sped up the characterization of this new virus, its novelty was indicated when targeted PCRs for the epidemic-prone viruses Ebola Zaire and Ebola Sudan failed to react, but an antigen detection assay reacted with initial patient bloods submitted to the Special Pathogens Branch at CDC in Atlanta [61]. As is common in Ebola outbreaks, much of the transmission occurred within medical facilities, where some of the initial patients sought care, and many of those subsequently infected included health-care workers [62]. In addition, the mortality associated with infection with this virus appears to be less than the Zaire and Sudan Ebola viruses [48].
Another filovirus has been associated with deaths in insectivorous bats in Spain, but the virus has not been isolated [63]. Its genetic signature appears to be between the existing Ebola viruses and Marburg virus, but its taxonomic status remains unsettled, and the host range and pathogenicity of the virus remain unknown and will probably remain so until a virus is either isolated or reconstructed from the sequence derived from the tissues of the dead bats.
3 The Virus
The filoviruses are negative-sense single-stranded RNA viruses. They are members of the family, Filoviridae, so named after the long filamentous appearance of the virions in electron micrographs. They belong to the order Mononegavirales. Marburg virus comprises one genus of the family (Marburgvirus), while the Ebola viruses comprise the other genus (Ebolavirus). The genomes are the largest of the viruses in this order having a genome of just over 19 kilobases. The order of the seven genes is similar to other members of the Mononegavirales, the rhabdoviruses and the paramyxoviruses. The nucleoprotein is located at the 3’ end of the genome and is followed by VP35, VP40, glycoprotein, VP30, VP24, and the L (polymerase) open reading frames [64]. Several of these proteins have the ability to interfere with the immune response of the host and are believed to play a role in the high pathogenicity of the filoviruses [65–67].
4 The Disease
Infection with Marburg and Ebola viruses leads to similar diseases which are marked by inappropriate innate immune responses which both downregulate the useful antiviral effects expected in the early postinfection period and induce vigorous responses of certain cytokines and chemokines, inducing a sepsis-like syndrome with high mortality. The mortality ranges between a high of approximately 90 % seen with Ebola Zaire virus infection, followed by approximately 55 % seen with Ebola Sudan, and approximately 35 % seen with Ebola Bundibugyo, the three viruses that seem to have epidemic potential. Ebola Ivory Coast has had too few infections, one or perhaps two, to allow a useful estimate of the mortality, while Ebola Reston has so far not caused mortality in the 10s of persons that have been infected. Marburg virus outbreaks have tended to be smaller, often with only one or two individuals infected, but there also may be strain differences in the mortality. Among the three outbreaks with significant numbers infected, the initial outbreak in Germany produced an overall mortality of approximately 23 % (7 of 30 or 31) [22, 23], while the small clusters constituting the 1998–2001 composite cases in the DRC outbreak had an overall mortality of 82 % (123/149) [27], and the 2005 outbreak in Uige, Angola, had a mortality of 90 % (227/252) [29].
In human cases, there is an incubation period of 5–7 days followed by onset of fever, weakness and often muscle pains, and abdominal discomfort. Rash is also a common feature, but in dark-skinned patients, it is not always apparent. Bleeding is not the common manifestation that many believe is the hallmark of the disease. In the Kikwit outbreak of Ebola Zaire in 1995, less than 50 % of the lab-confirmed cases had bleeding signs. The viruses are considered to be pantropic, infecting many tissues and also infecting many cell lines from a great many mammalian species [68]. Among those with bleeding signs, petechiae, ecchymoses, and gastrointestinal bleeding along with failure of venipuncture sites to clot are the most common forms of bleeding. Nevertheless the disease is severe and vascular permeability, loss of fluids from the GI tract from diarrhea and vomiting, and diminished fluid intake all combine with the effects of the inappropriate immune response to induce shock and eventual multiorgan failure.
Patients who do survive often have prolonged recoveries with hair loss and desquamation of areas initially affected by rash. Weakness, myalgias, and arthralgias were also common among survivors of the Kikwit outbreak in which convalescent survivors were compared to controls. In human cases, lesions are common throughout the tissues with endothelial cells and macrophages in many organs having demonstrable virus antigens as well as histological changes and virus antigens in the parenchyma [69–71].
5 Laboratory Diagnosis
As for all virus diseases, detection of the virus (or its antigens or nucleic acids) or detection of the resulting antibody response in patients is the primary means of confirming a specific diagnosis. Virus antigens are also found in the skin, a feature which has been exploited to allow for diagnosis using skin biopsies fixed in formalin, which may aid in surveillance for the filoviruses. Until the early 1990s, virus isolation and identification by electron microscopy or reference immune reagents remained the definitive means of definitive diagnosis. This was difficult as high-containment laboratories, of which there were very few in the world, were required to carry out this work safely. Detection of antibodies was also somewhat fraught with issues as the indirect fluorescent antibody test was prone to yield false positives in the sera of individuals who had no previous exposure to filoviruses and the antibody response requires some time to become apparent, and in many instances patients died without yet having detectable antibodies. Following the outbreak of a new Ebola virus in Reston in 1989, a number of newer technologies were applied to the diagnosis of Ebola virus infections. An antigen detection assay, utilized extensively in the Reston outbreak and its investigation, allowed for a rapid and specific identification of Ebola virus in the blood of acutely ill individuals even in remote areas [72]. Continued difficulties with the nonspecific detection of antibodies by the indirect fluorescent antibody test in primates during the Reston investigation led to the adaption of enzyme-linked immunosorbent assays to the detection of both IgM antibody in acute Ebola infections and IgG antibody in individuals surviving infection [73] and the application of these assays to human patients in the Kikwit outbreak [74]. These assays also had the advantage that they could be adapted for use in the field during outbreaks or outbreak investigations by utilizing appropriate personal protective equipment and inactivating the clinical specimens using heat and detergent. This allowed the diagnosis of patients quickly in either onsite or at a local laboratory, depending on the logistical support and demands of the particular outbreak. At about the same time that the antigen detection and serological assays were being developed, the use of reverse transcriptase-polymerase chain reactions for the detection and diagnosis of RNA viruses advanced where it too began to play a role in Ebola diagnosis [75] which eventually led to it being deployed to the field setting along with the ELISA tests [29, 76]. Another means of diagnosis, particularly useful in remote areas, was described and shown to be of utility during the Kikwit outbreak and employs the use of formalin-fixed skin snips as a means of avoiding invasive postmortem exams and the safety and convenience of using formalin for transport of the biopsy to a suitable laboratory for diagnostic testing [72].
6 Epidemiology and Ecology
6.1 Epidemiology
The epidemiology of the filoviruses is largely comprised of the person-to-person transmission that occurs once the virus has been introduced into the human population. The distribution of the virus and, for the most part, the disease is dictated by the underlying ecology of these zoonotic viruses that reside in reservoir or maintenance hosts.
The high mortality associated with filovirus infection has created an aura of fear associated with the outbreaks. At a local level, particularly in the developing world where the virus appears to be resident, this is understandable. The history of outbreaks is marked by caregivers as early victims of the disease. However, intense investigations during more recent outbreaks have provided valuable information on how transmission occurs and the level of protection that is necessary to protect caregivers and aid in stopping the chain of transmission that continues to fuel the epidemics. This was afforded by an earlier response than had occurred in the initial Ebola outbreaks of the 1970s and was particularly taken advantage of during the Kikwit outbreak in 1995.
The principle lessons are that transmission of the filoviruses is by direct contact with infectious material and that moderate infection control practices, rigorously applied and controlled, can almost immediately stop transmission [77]. In most of the endemic areas, this is a matter of providing resources and training to health-care facilities where they may be available on only a limited basis and are not routinely used in the everyday practice of health care. In the developed world, standards of care and the employment of standard precautions for patient contact have addressed the majority of the risks associated with caring for patients with these infections as has been demonstrated in a number of instances of imported cases where no, or, at worst, very limited, transmission to care givers has occurred [31, 40].
Risks to individuals in the community who do not have direct contact with infected patients are practically nonexistent. Assessment of risks during the outbreak in Kikwit gave ample testament to the association of infection to exposure to seriously ill patients or the cadavers of individuals who had died of Ebola infection [78, 79]. Nevertheless, some care and education to avoid transmission via blood-borne routes by traditional medicine practices or reuse of needles in local pharmacies remain a concern.
Even though the filoviruses can be readily transmitted by the experimental creation of small particle aerosols, the role of aerosol transmission in outbreaks is, at most, minimal as attested by the lack of transmission in the community, other than by direct contact, and by studies of family members sharing small enclosed spaces with infected patients [78].
6.2 Ecology
The reservoirs of the filoviruses are just beginning to be understood, and only recently has the primary host for Marburg virus, rousette fruit bats (Rousettus aegyptiacus), been established with a degree of certainty [80–82]. The reservoir host(s) for the Ebola viruses is less certain, but indications are that, like Marburg virus, bats are the leading candidates [83, 84]. Anecdotal accounts of outbreaks going back to the Sudan outbreaks of the 1970s, in which the initial cases in both 1976 and 1979 worked in a cotton factory in which there were resident bats [85], have suggested to many in the field that bats were leading candidates, but hard scientific data was lacking until more recent circumstances provided stronger circumstantial and scientific support for this contention.
The big break for Marburg virus came when an outbreak in Durba in the Democratic Republic of Congo (formerly Zaire) which began in 1999 provided a combination of scientific and circumstantial evidence that led to further concentration on bats as the reservoir. The outbreak in this instance was not a typical filovirus outbreak with a single introduction of the virus and a serial passage of that virus through a chain of human cases; rather, in this instance, it was a series of small outbreaks. This could be discerned because the viruses that caused each of the mini-outbreaks could be genetically differentiated and the epidemiology of each small chain leads back to a single source of the virus. This source was a former commercial mine now being exploited by free-lance miners who were at the beginning of the transmission chain for each of the small mini-outbreaks [27]. Investigation of the mine found that bats were the principal fauna and genetic evidence of Marburg virus could be found in animals collected during the investigation [86]. These findings were further advanced by investigations of cases occurring or originating in Uganda that were associated with large concentrations of bats first at the Kamwenge mines [28, 30], where miners were infected, and then at a cave in Queen Elizabeth Park, where two tourists became infected [31, 32]. Subsequent investigations of the bat populations have allowed the repeated isolation of the virus from the rousette bats that are the principal fauna of these two locations and the demonstration of the persistence of the virus in the bat populations [80, 81].
7 Prevention
Prevention of filovirus outbreaks is possible. In the first instance, now that the reservoirs of the viruses are becoming apparent, education of local populations should enable them to avoid the source of the virus. However, this may be culturally difficult in hunter-gatherer populations that have strong traditional values that may be difficult to change, particularly in economically developing areas where hunting remains an important source of nutrition.
7.1 Infection Control
Outbreaks of disease are more often the product of exposure of individuals to the primary case who is infected by interaction with the reservoir. The lesson of the last 20 years is that infection control in health-care facilities, often the source of amplification of outbreaks, can stop the transmission of the viruses from patients in these settings. Unfortunately, this does require that these facilities have the basic supplies that are part of the daily routine of medical care in the developed world, what have come to be known as standard precautions. Without the ability to use these simple measures, including routine hand washing and single use of needles and syringes, outbreaks are likely to continue to be amplified by health-care facilities in the endemic areas.
7.2 Vaccines
Vaccines are being developed and have reached a stage where nonhuman primates can be protected from infection by Ebola and Marburg viruses [87–91]. Some of these vaccines have even demonstrated their potential use as therapeutics for treatment of individuals following exposure to a filovirus if the vaccine is administered relatively soon after infection [92]. While almost all funding for the development of filovirus vaccines is driven by biodefense concerns, the vaccines are of practical use in providing protection to individuals who have occupational exposure because they work with the agents in the laboratory and to individuals who respond to outbreaks that have similar risks of exposure from caring for patients in the field. There, in reality, is probably little use for filovirus vaccines as a means of protecting populations in endemic areas because the outbreaks are so sporadic and focal that the cost of immunization would not be economically viable; at best they might be used in the midst of an outbreak to provide protection to at-risk individuals, particularly if the protection is rapid, as the postexposure treatment use of certain of these vaccines is effective as pointed out above. One added note about the use of vaccines, there is at best limited cross-protection among the Ebola virus vaccines, and no cross-protection between Marburg virus and Ebola viruses; multivalent vaccines will have to be developed or the vaccines targeted at outbreaks with known filovirus etiology.
8 Treatment
Aside from vaccines used postexposure, there have been some advances in therapeutics for filoviruses.
8.1 Monoclonal Antibodies
Monoclonal antibodies have recently been shown to protect nonhuman primates against Ebola Zaire infection [92–95]. Efforts are underway to improve the utility of some of these preparations by making them more compatible for use as human therapeutics. As was the case for the vaccines, the monoclonal preparations are directed against specific filoviruses and would be most effective when used in situations where the specific virus causing disease was known. Monoclonal antibody cocktails would be needed to broaden protection against multiple viruses.
8.2 iRNAs
Specific iRNAs have recently been shown to be effective in the treatment of Ebola virus-infected animals [96, 97]. However, like vaccines, these are targeted and exhibit specificity of action which means that a cocktail of iRNAs would be required for situations in which the virus was not yet identified or if a new filovirus were to appear. Closely related to the use of iRNAs has been the use of antisense phosphorodiamidate morpholino oligomers (PMOs) which are also targeted at specific RNA sequences but increase the stability, affinity, and access into cells of the antisense nucleotides. In a recent study, they have been used and demonstrated to successfully treat up to 75 % of rhesus macaques from Ebola Zaire infection when used either pre- or post-virus challenge [98].
8.3 Small Molecule Inhibitors
Other small molecule inhibitors of the viruses have been described from in vitro screening exercises or testing of compounds with antiviral activity with other non-filovirus viruses. However, there has only been limited screening of these compounds in in vivo screening in filovirus small animal models, which have not been great predictors of positive performance of vaccines and antiviral drugs in primates [99].
9 Unresolved Problems
Even though the reservoir of Marburg virus is now reasonably established as the cave-dwelling fruit bat, Rousettus aegyptiacus, the definitive reservoir of the Ebola viruses has remained elusive. As discussed in previous sections, although a number of species of fruit bats have been identified by RT-PCR as containing Ebola virus RNA, virus isolation and studies demonstrating persistence of the virus in reservoir populations remain lacking.
There remain a number of issues with the filoviruses. The foremost is probably the lack of approved vaccines or therapeutics for use in the rare individuals who are exposed in endemic areas during epidemics or individuals exposed during the course of lab work with the agents. Much progress has been made in finding candidate vaccines that have been effective in experimental use in primates, but the regulatory pathway for licensure of these products is dependent on the application of the so-called animal rule. This mechanism went into effect as a means of approving medical countermeasures that are unable to undergo traditional efficacy trials for ethical or practical reasons as 21 CFRParts 314 and 601 in July, 2002. However, the interpretation and implementation of the animal rule have remained a somewhat controversial pathway for product approval with much interpretation of various facets of the rule remaining illusive and resulting in only a few products being approved (and those being for medical countermeasures previously licensed for other purposes) [100, 101]. These issues will have to be resolved to provide a predictable pathway for approval of medical countermeasures for the filoviruses.
Field and laboratory research on the filoviruses have never been simple. High-containment laboratories capable of doing research have always been scarce. The post-9/11 environment has created other obstacles that are associated with these viruses being considered as “weapons of mass destruction” that have tangibly increased the practical burdens and expense of working with the agents. The public health importance of the filoviruses in endemic areas is emphasized by the number of outbreaks that have occurred recently (see Tables 14.1 and 14.2). The practical and administrative aspects of moving diagnostic specimens from suspected outbreaks, making virus isolates, curating virus strains, and clearing and training scientific personnel have all increased with the frequent advent of additional layers of security regulations that are levied on labs and personnel that work with these viruses.
References
Anonymous. Disease transmitted from monkeys to man. Lancet. 1967;2:1129–30.
Anonymous. Disease from monkeys. Br Med J. 1967;4:758–9.
Anonymous. Outbreak in laboratory personnel working with Cercopithecus monkeys from East Africa – Europe. Wkly Epidemiol Rec. 1968;43:61–2.
Gear JS, Cassel GA, Gear AJ, Trappler B, Clausen L, Meyers AM, Kew MC, Bothwell TH, Sher R, Miller GB, et al. Outbreak of Marburg virus disease in Johannesburg. Br Med J. 1975;4(5995):489–93.
Conrad JL, Isaacson M, Smith EB, Wulff H, Crees M, Geldenhuys P, Johnston J. Epidemiologic investigation of Marburg virus disease, Southern Africa, 1975. Am J Trop Med Hyg. 1978;27(6):1210–5.
Anonymous. Viral hemorrhagic fever: Sudan and Zaire. Morb Mortal Wkly Rep. 1977;26(26):209–10.
Anonymous. Ebola haemorrhagic fever in Sudan, 1976. Report of a WHO/International Study Team. Bull World Health Organ. 1978;56(2):247–70.
Anonymous. Ebola haemorrhagic fever in Zaire, 1976. Bull World Health Organ. 1978;56(2):271–93.
Simpson DI, Zuckerman AJ. Marburg and Ebola: viruses in search of a relation. Nature. 1977;266(5599):217–8.
Heymann DL, Weisfeld JS, Webb PA, Johnson KM, Cairns T, Berquist H. Ebola hemorrhagic fever: Tandala, Zaire, 1977–1978. J Infect Dis. 1980;142(3):372–6.
Anonymous. Ebola hemorrhagic fever – Southern Sudan. Morb Mortal Wkly Rep. 1979;28(47):557–9.
Anonymous. Viral haemorrhagic fever – Sudan. Wkly Epidemiol Rec. 1979;54:319.
Richman DD, Cleveland PH, McCormick JB, Johnson KM. Antigenic analysis of strains of Ebola virus: identification of two Ebola virus serotypes. J Infect Dis. 1983;147(2):268–71.
Cox NJ, McCormick JB, Johnson KM, Kiley MP. Evidence for two subtypes of Ebola virus based on oligonucleotide mapping of RNA. J Infect Dis. 1983;147(2):272–5.
Jahrling PB, Geisbert TW, Dalgard DW, Johnson ED, Ksiazek TG, Hall WC, Peters CJ. Preliminary report: isolation of Ebola virus from monkeys imported to USA. Lancet. 1990;335(8688):502–5.
Miranda ME, White ME, Dayrit MM, Hayes CG, Ksiazek TG, Burans JP. Seroepidemiological study of filovirus related to Ebola in the Philippines. Lancet. 1991;337:425–6.
Hayes CG, Burans JP, Ksiazek TG, Del Rosario RA, Miranda ME, Manaloto CR, Barrientos AB, Robles CG, Dayrit MM, Peters CJ. Outbreak of fatal illness among captive macaques in the Philippines caused by an Ebola-related filovirus. Am J Trop Med Hyg. 1992;46(6):664–71.
Anonymous. Viral haemorrhagic fever in imported monkeys. Wkly Epidemiol Rec. 1992;67(19):142–3.
Perini L. Outbreak of Ebola virus in Italy. Folia Primatol. 2000;71(4):280.
Rollin PE, Williams J, Bressler D, Pearson S, Cottingham M, Pucak G, Sanchez A, Trappier S, Peters RL, Greer PW, et al. Isolated cases of Ebola (subtype Reston) virus among quarantined non-human primates recently imported from the Philippines to the United States. J Infect Dis. 1999;179 suppl 1:S108–14.
Le Guenno B, Formenty P, Wyers M, Gounon P, Walker F, Boesch C. Isolation and partial characterisation of a new strain of Ebola virus. Lancet. 1995;345:1271–4.
Siegert R. Marburg virus, vol. 11. New York: Springer; 1972.
Feldmann H, Slenczka W, Klenk HD. Emerging and reemerging of filoviruses. Arch Virol. 1996;11(suppl):77–100.
Anonymous. Marburg virus disease – South Africa. Wkly Epidemiol Rec. 1975;50(12):124–25.
Smith DH, Johnson BK, Isaacson M, Swanepoel R, Johnson KM, Kiley M, Bagshawe A, Siongok T, Keruga WK. Marburg-virus disease in Kenya. Lancet. 1982;1(8276):816–20.
Johnson ED, Johnson BK, Silverstein D, Tukei P, Geisbert TW, Sanchez AN, Jahrling PB. Characterization of a new Marburg virus isolated from a 1987 fatal case in Kenya. Arch Virol. 1996;11(suppl):101–14.
Bausch DG, Nichol ST, Muyembe-Tamfum JJ, Borchert M, Rollin PE, Sleurs H, Campbell P, Tshioko FK, Roth C, Colebunders R, et al. Marburg hemorrhagic fever associated with multiple genetic lineages of virus. N Engl J Med. 2006;355:909–19.
Anonymous. Outbreak of Marburg haemorrhagic fever: Uganda, June–August 2007. Wkly Epidemiol Rec. 2007;82(43):381–84.
Towner JS, Khristova ML, Sealy TK, Vincent MJ, Erickson BR, Bawiec DA, Hartman AL, Comer JA, Zaki SR, Stroher U, et al. Marburgvirus genomics and association with a large hemorrhagic fever outbreak in Angola. J Virol. 2006;80(13):6497–516.
Adjemian J, Farnon EC, Tschioko F, Wamala JF, Byaruhanga E, Bwire GS, Kansiime E, Kagirita A, Ahimbisibwe S, Katunguka F, et al. Outbreak of Marburg hemorrhagic fever among miners in Kamwenge and Ibanda districts, Uganda, 2007. J Infect Dis. 2011;204 suppl 3:S796–9.
Anonymous. Imported case of Marburg hemorrhagic fever – Colorado, 2008. MMWR Morb Mortal Wkly Rep. 2009;58(49):1377–81.
Timen A, Koopmans MPG, Vossen ACTM, van Doornum GJJ, Gunther S, van den Berkmortel F, Verduin KM, Dittrich S, Emmerich P, Osterhaus ADME, et al. Response to imported case of Marburg hemorrhagic fever, the Netherland. Emerg Infect Dis. 2009;15(8):1171–5.
Case of Marburg haemorrhagic fever imported into the Netherlands from Uganda. http://www.who.int/csr/don/2008_07_10/en/index.html
Green A. Uganda battles Marburg fever outbreak. Lancet. 2012;380(9855):1726.
Emond RT, Evans B, Bowen ET, Lloyd G. A case of Ebola virus infection. Br Med J. 1977;2(6086):541–4.
Baron RC, McCormick JB, Zubeir OA. Ebola virus disease in southern Sudan: hospital dissemination and intrafamilial spread. Bull World Health Organ. 1983;61(6):997–1003.
Anonymous. Update: filovirus infection in animal handlers. MMWR Morb Mortal Wkly Rep. 1990;39(13):221.
Georges AJ, Leroy EB, Renaut AA, Tevi-Benissan C, Nabias RJ, Ngoc MT, Obiang PI, Mba-Bekale S, Bertherat EJ, Benoni DD, et al. Ebola hemorrhagic fever outbreaks in Gabon, 1994–1997: epidemiologic and health control issues. J Infect Dis. 1999;179 suppl 1:S65–75.
Khan AS, Tshioko FK, Heymann DL, Le Guenno B, Nabeth P, Kerstiens B, Fleerackers Y, Kilmarx PH, Rodier GR, Nkuku O, et al. The reemergence of Ebola hemorrhagic fever, Democratic Republic of the Congo, 1995. Commission de Lutte contre les Epidemies a Kikwit. J Infect Dis. 1999;179 suppl 1:S76–86.
Anonymous. Ebola haemorrhagic fever – South Africa. Wkly Epidemiol Rec. 1996;71(47):359.
Miranda ME, Ksiazek TG, Retuya TJ, Khan AS, Sanchez A, Fulhorst CF, Rollin PE, Calaor AB, Manalo DL, Roces MC, et al. Epidemiology of Ebola (subtype Reston) virus in the Philippines, 1996. J Infect Dis. 1999;179 suppl 1:S115–9.
Okware SI, Omaswa FG, Zaramba S, Opio A, Lutwama JJ, Kamugisha J, Rwaguma EB, Kagwa P, Lamunu M. An outbreak of Ebola in Uganda. Trop Med Int Health. 2002;7(12):1068–75.
Anonymous. Outbreak(s) of Ebola haemorrhagic fever, Congo and Gabon, October 2001-July 2002. Wkly Epidemiol Rec. 2003;78(26):223–28.
Formenty P, Libama F, Epelboin A, Allarangar Y, Leroy E, Moudzeo H, Tarangonia P, Molamou A, Lenzi M, Ait-Ikhlef K, et al. Outbreak of Ebola hemorrhagic fever in the Republic of the Congo, 2003: a new strategy? Med Trop (Mars). 2003;63(3):291–5.
Ebola haemorrhagic fever in the Republic of the Congo – Update 6. http://www.who.int/csr/don/2004_01_06/en/print.html
Anonymous. Outbreak of Ebola hemorrhagic fever in Yambio, south Sudan, April–June 2004. Wkly Epidemiol Rec. 2005;80(43):370–75.
Anonymous. Marburg haemorrhagic fever, Democratic Republic of the Congo (Should be Ebola). Wkly Epidemiol Rec. 2007;82(38):329.
MacNeil A, Farnon EC, Wamala JF, Okware S, Cannon DL, Reed ZD, Lutwama J, Downing R, Nichol ST, Ksiazek TG, et al. Proportion of deaths and clinical features in Bundibugyo Ebola virus infection, Uganda. Emerg Infect Dis. 2010;16(12):1969–72.
Macneil A, Farnon EC, Morgan OW, Gould P, Boehmer TK, Blaney DD, Wiersma P, Tappero JW, Nichol ST, Ksiazek TG, et al. Filovirus outbreak detection and surveillance: lessons from Bundibugyo. J Infect Dis. 2011;204 suppl 3:S761–7.
Outbreak news. Ebola Reston in pigs and humans, Philippines. Wkly Epidemiol Rec. 2009;84(7):49–50.
Barrette RW, Metwally SA, Rowland JM, Xu L, Zaki SR, Nichol ST, Rollin PE, Towner JS, Shieh WJ, Batten B, et al. Discovery of swine as a host for the Reston ebolavirus. Science. 2009;325(5937):204–6.
End of Ebola outbreak in the Democratic Republic of the Congo. http://www.who.int/csr/don/2009_02_17/en/
Shoemaker T, Macneil A, Balinandi S, Campbell S, Wamala JF, McMullan LK, Downing R, Lutwama J, Mbidde E, Stroher U, et al. Reemerging Sudan ebola virus disease in Uganda, 2011. Emerg Infect Dis. 2012;18(9):1480–3.
Anonymous. Outbreak news. Ebola haemorrhagic fever, Uganda. Wkly Epidemiol Rec. 2012;87(36):339.
Anonymous. Outbreak news. Ebola haemorrhagic fever, Democratic Republic of the Congo. Wkly Epidemiol Rec. 2012;87(36):338–9.
Anonymous. Outbreak news. Ebola, Democratic Republic of Congo – update. Wkly Epidemiol Rec. 2012;87(38):357.
Anonymous. Outbreak news. Ebola, Democratic Republic of the Congo. Wkly Epidemiol Rec. 2012;87(44):421.
Anonymous. Ebola haemorrhagic fever, Uganda – update. Wkly Epidemiol Rec. 2012;87(36):493–508.
Anonymous. (2014, 20140426). Ebola virus disease, West Africa – update–20140428. WHO – GAR: disease outbreak news. Retrieved 0430, 2014. http://www.who.int/csr/don/2014_04_28_ebola/en/
Anonymous. (2014, 20140425). Ebola virus disease, West Africa – update–20140425. WHO – GAR: disease outbreak news. Retrieved 0430, 2014. http://www.who.int/csr/don/2014_04_25_ebola/en/
Towner JS, Sealy TK, Khristova ML, Albarino CG, Conlan S, Reeder SA, Quan PL, Lipkin WI, Downing R, Tappero JW, et al. Newly discovered ebola virus associated with hemorrhagic fever outbreak in Uganda. PLoS Pathog. 2008;4(11):e1000212.
Wamala JF, Lukwago L, Malimbo M, Nguku P, Yoti Z, Musenero M, Amone J, Mbabazi W, Nanyunja M, Zaramba S, et al. Ebola hemorrhagic fever associated with novel virus strain, Uganda, 2007–2008. Emerg Infect Dis. 2010;16(7):1087–92.
Negredo A, Palacios G, Vázquez-Morón S, González F, Dopazo H, Molero F, Juste J, Quetglas J, Savji N, de la Cruz MM, et al. Discovery of an ebolavirus-like filovirus in Europe. PLoS Pathog. 2011;7(10):e1002304.
Feldmann H, Mühlberger E, Randolf A, Will C, Kiley MP, Sanchez A, Klenk HD. Marburg virus, a filovirus: messenger RNAs, gene order, and regulatory elements of the replication cycle. Virus Res. 1992;24(1):1–19.
Basler CF, Mikulasova A, Martinez-Sobrido L, Paragas J, Muhlberger E, Bray M, Klenk H-D, Palese P, Garcia-Sastre A. The Ebola virus VP35 protein inhibits activation of interferon regulatory factor 3. J Virol. 2003;77(14):7945–56.
Valmas C, Basler CF. Marburg virus VP40 antagonizes interferon signaling in a species-specific manner. J Virol. 2011;85(9):4309–17.
Mateo M, Reid SP, Leung LW, Basler CF, Volchkov VE. Ebolavirus VP24 binding to karyopherins is required for inhibition of interferon signaling. J Virol. 2010;84(2):1169–75.
Bwaka MA, Bonnet M-J, Calain P, Colebunders R, De Roo A, Guimard Y, Katwiki KR, Kibadi K, Kipasa MA, Kuvula KJ, et al. Ebola hemorrhagic fever in Kikwit, Democratic Republic of Congo (former Zaire): clinical observations. J Infect Dis. 1999;179 suppl 1:S1–7.
Peters CJ, Zaki SR, and Rollin P. Viral hemorrhagic fevers. In: Mandell GL, and Fekety R, (ed.). Atlas of Infectious Diseases. Volume VIII. External manifestations of systemic infections. Philadelphia: Chruchill Livingstone; 1997. p. 10.2–10.26.
Zaki SR, Kilmarx PH. Ebola virus hemorrhagic fever, vol. Chap 17. Washington: ASM Press; 1997.
Zaki SR, Peters CJ. Viral hemorrhagic fevers. In: Connor DH, Chandler FW, Schwartz DA, Manz HJ, and Lack EE, (ed.). The Pathology of Infectious Diseases, vol. 2. Norwalk: Appleton & Lange; 1997. p. 347–364.
Zaki SR, Shieh W-J, Greer PW, Goldsmith CS, Ferebee T, Katshitshi J, Tchioko K, Bwaka MA, Swanepoel R, Calain P, et al. A novel immunohistochemical assay for detection of Ebola virus in skin: implications for diagnosis, spread, and surveillance of Ebola hemorrhagic fever. J Infect Dis. 1999;179 suppl 1:S36–47.
Ksiazek TG, West CP, Rollin PE, Jahrling PB, Peters CJ. ELISA for the detection of antibodies to Ebola viruses. J Infect Dis. 1999;179 suppl 1:S192–8.
Ksiazek TG, Rollin PE, Williams AJ, Bresler DS, Martin ML, Swanepoel R, Burt FJ, Leman PA, Khan AS, Rowe AK, et al. Clinical virology of Ebola hemorrhagic fever (EHF): virus, virus antigen, and IgG and IgM antibody findings among EHF patients in Kikwit, Democratic Republic of the Congo, 1995. J Infect Dis. 1999;179 suppl 1:S177–87.
Sanchez A, Feldmann H. Detection of Marburg and Ebola virus infections by polymerase chain reaction assays. Berlin/Heidelberg: Springer; 1995.
Towner JS, Rollin PE, Bausch DG, Sanchez A, Crary SM, Vincent M, Lee WF, Spiropoulou CF, Ksiazek TG, Lukwiya M, et al. Rapid diagnosis of Ebola hemorrhagic fever by reverse transcription-PCR in an outbreak setting and assessment of patient viral load as a predictor of outcome. J Virol. 2004;78(8):4330–41.
Khan AS, Kweteminga TF, Heymann DH, Le Guenno B, Nabeth P, Kerstiens B, Freerackers Y, Kilmarx PH, Rodier GR, Nkuku O, et al. The reemergence of Ebola hemorrhagic fever (EHF), Democratic Republic of the Congo, 1995. J Infect Dis. 1999;179 suppl 1:S76–86.
Dowell SF, Mukunu R, Ksiazek TG, Khan AS, Rollin PE, Peters CJ, Kikwit ftCdLclEà. Transmission of Ebola hemorrhagic fever: a study of risk factors in family members, Kikwit, Democratic Republic of the Congo, 1995. J Infect Dis. 1999; 179 (suppl 1):S87–91.
Roels TH, Bloom AS, Buffington J, Muhungu GL, MacKenzie WR, Khan AS, Ndambi R, Noah DL, Rolka HR, Peters CJ, et al. Ebola hemorrhagic fever, Kikwit, Democratic Republic of Congo, 1995: risk factors for patients without a reported exposure. J Infect Dis. 1999;179 suppl 1:S92–7.
Amman BR, Carroll SA, Reed ZD, Sealy TK, Balinandi S, Swanepoel R, Kemp A, Erickson BR, Comer JA, Campbell S, et al. Seasonal pulses of Marburg virus circulation in juvenile Rousettus aegyptiacus bats coincide with periods of increased risk of human infection. PLoS Pathog. 2012;8(10):e1002877.
Towner JS, Amman BR, Sealy TK, Carroll SA, Comer JA, Kemp A, Swanepoel R, Paddock CD, Balinandi S, Khristova ML, et al. Isolation of genetically diverse Marburg viruses from Egyptian fruit bats. PLoS Pathog. 2009;5(7):e1000536.
Towner JS, Pourrut X, Albarino CG, Nkogue CN, Bird BH, Grard G, Ksiazek TG, Gonzalez JP, Nichol ST, Leroy EM. Marburg virus infection detected in a common African bat. PLoS ONE. 2007;2(1):e764.
Leroy EM, Epelboin A, Mondonge V, Pourrut X, Gonzalez JP, Muyembe-Tamfum JJ, Formenty P. Human Ebola outbreak resulting from direct exposure to fruit bats in Luebo, Democratic Republic of Congo, 2007. Vector Borne Zoonotic Dis. 2009;9(6):723–8.
Leroy EM, Kumulungui B, Pourrut X, Rouquet P, Hassanin A, Yaba P, Delicat A, Paweska JT, Gonzalez J-P, Swanepoel R. Fruit bats as reservoirs of Ebola virus. Nature. 2005;438:575–6.
Smith DH, Francis DP, Simpson DIH, Highton RB. The Nzara outbreak of viral haemorrhagic fever. Amsterdam: Elsevier/North-Holland Biomedical Press; 1978.
Swanepoel R, Smit SB, Rollin PE, Formenty P, Leman PA, Kemp A, Burt FJ, Grobbelaar AA, Croft J, Bausch DG, et al. Studies of reservoir hosts for Marburg virus. Emerg Infect Dis. 2007;13(12):1847–51.
Sullivan NJ, Sanchez A, Rollin PE, Yang Z-Y, Nabel GJ. Development of a preventive vaccine for Ebola virus infection in primates. Nature. 2000;408(6812):605–9.
Jones SM, Feldmann H, Ströher U, Geisbert JB, Fernando L, Grolla A, Klenk H-D, Sullivan NJ, Volchkov VE, Fritz EA, et al. Live attenuated recombinant vaccine protects nonhuman primates against Ebola and Marburg viruses. Nat Med. 2004;11(7):786–90.
Jones SM, Feldmann H, Stroher U, Geisbert JB, Fernando L, Grolla A, Klenk HD, Sullivan NJ, Volchkov VE, Fritz EA, et al. Live attenuated recombinant vaccine protects nonhuman primates against Ebola and Marburg viruses. Nat Med. 2005;11(7):786–90.
Geisbert TW, Daddario-Dicaprio KM, Geisbert JB, Reed DS, Feldmann F, Grolla A, Stroher U, Fritz EA, Hensley LE, Jones SM, et al. Vesicular stomatitis virus-based vaccines protect nonhuman primates against aerosol challenge with Ebola and Marburg viruses. Vaccine. 2008;26(52):6894–900.
Geisbert TW, Geisbert JB, Leung A, Daddario-DiCaprio KM, Hensley LE, Grolla A, Feldmann H. Single-injection vaccine protects nonhuman primates against infection with marburg virus and three species of ebola virus. J Virol. 2009;83(14):7296–304.
Feldmann H, Jones SM, Daddario-DiCaprio KM, Geisbert JB, Stroher U, Grolla A, Bray M, Fritz EA, Fernando L, Feldmann F, et al. Effective post-exposure treatment of Ebola infection. PLoS Pathog. 2007;3(1):e2.
Qiu X, Audet J, Wong G, Pillet S, Bello A, Cabral T, Strong JE, Plummer F, Corbett CR, Alimonti JB, et al. Successful treatment of ebola virus-infected cynomolgus macaques with monoclonal antibodies. Sci Transl Med. 2012;4(138):138ra181.
Olinger Jr GG, Pettitt J, Kim D, Working C, Bohorov O, Bratcher B, Hiatt E, Hume SD, Johnson AK, Morton J, et al. Delayed treatment of Ebola virus infection with plant-derived monoclonal antibodies provides protection in rhesus macaques. Proc Natl Acad Sci U S A. 2012;109(44):18030–5.
Marzi A, Yoshida R, Miyamoto H, Ishijima M, Suzuki Y, Higuchi M, Matsuyama Y, Igarashi M, Nakayama E, Kuroda M, et al. Protective efficacy of neutralizing monoclonal antibodies in a nonhuman primate model of ebola hemorrhagic Fever. PLoS One [Electronic Resource]. 2012;7(4):e36192.
Geisbert TW, Hensley LE, Kagan E, Yu EZ, Geisbert JB, Daddario-Dicaprio K, Fritz EA, Jahrling PB, McClintock K, Phelps JR, et al. Postexposure protection of guinea pigs against a lethal ebola virus challenge is conferred by RNA interference. J Infect Dis. 2006;193(12):1650–7.
Geisbert TW, Lee ACH, Robbins M, Geisbert JB, Honko AN, Sood V, Johnson JC, de Jong S, Tavakoli I, Judge A, et al. Postexposure protection of non-human primates against a lethal Ebola virus challenge with RNA interference: a proof-of-concept study. Lancet. 2010;375(9729):1896–905.
Warfield KL, Swenson DL, Olinger GG, Nichols DK, Pratt WD, Blouch R, Stein DA, Aman MJ, Iversen PL, Bavari S. Gene-specific countermeasures against Ebola virus based on antisense phosphorodiamidate morpholino oligomers. PLoS Pathog. 2006;2(1):5–13.
Friedrich BM, Trefry JC, Biggins JE, Hensley LE, Honko AN, Smith DR, Olinger GG. Potential vaccines and post-exposure treatments for filovirus infections. Viruses. 2012;4(9):1619–50.
Aebersold P. FDA experience with medical countermeasures under the animal rule. Adv Prev Med. 2012;2012:507571.
Dolgin E. Animal rule for drug approval creates a jungle of confusion. Nat Med. 2013;19(2):118–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Ksiazek, T.G. (2014). Filoviruses: Marburg and Ebola. In: Kaslow, R., Stanberry, L., Le Duc, J. (eds) Viral Infections of Humans. Springer, Boston, MA. https://doi.org/10.1007/978-1-4899-7448-8_14
Download citation
DOI: https://doi.org/10.1007/978-1-4899-7448-8_14
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4899-7447-1
Online ISBN: 978-1-4899-7448-8
eBook Packages: MedicineMedicine (R0)