
Abstract
Much of the adult life is spent in the workplace. Working provides many benefits in terms of financial resources, social status, boosting self-esteem, and providing a social network. However, the workplace can have negative as well as positive effects on mental health and behavioral disorders. High levels of demands at work without the compensation of control over work, an imbalance between effort put in and reward received, bullying and discrimination at work, and job insecurity have been related to a greater risk of common mental disorders. Conversely, social support from supervisors and colleagues can have positive effects on mental health at work.
Health effects in the workplace vary by position in the life course and a number of markers of potential vulnerability. Research has shown that some groups are at high risk of mental health problems and the workplace can convey an additional risk. Risk markers include gender, ethnicity, sexuality, previous mental health problems, and learning disabilities. Those starting work and older people may also be vulnerable to health effects related to work.
We present the relatively few workplace organizational interventions and individual interventions tackling primary, secondary, and tertiary prevention of ill health. There are considerable limitations to current research on the workplace and health and many areas that need further development and objective measurement. There is a need for a substantial amount of further research to identify effective workplace based interventions to improve the health of the economically most important sector of the population.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Much of adult life is spent in the workplace. Working provides many benefits in terms of financial resources, social status, boosting self-esteem, and providing a social network. However, the workplace can have negative as well as positive effects on mental health and behavioral disorders. High levels of demands at work without the compensation of control over work, an imbalance between effort invested and reward received, bullying and discrimination at work, and job insecurity have been related to a greater risk of common mental disorders. Conversely, social support from supervisors and colleagues can have positive effects on mental health.
Health effects in the workplace vary according to position in the life course, and there are a number of markers of potential vulnerability. Research has shown that some groups are at high risk of mental health problems, and the workplace can convey an additional risk. Risk markers include gender, ethnicity, sexuality, previous mental health problems, and learning disabilities. Those starting work and older people may also be vulnerable.
This chapter presents the relatively few studies that have assessed organizational workplace interventions tackling primary, secondary, and tertiary prevention of ill health. There are considerable limitations to current research on the workplace and health, and many areas need further development and more robust methodology. The identification of effective workplace-based interventions to improve the mental health of the economically active is at its infancy and requires considerable further research.
The workplace is an important potential site for the prevention of ill health. In industrialized countries the majority of the population spends most of its adult life working. Thus, what happens in the workplace is influential for people’s lives and well-being. Work provides many useful benefits: financial resources, the social status of an occupation, a structure to the day, boosts to self-esteem, and a social network with whom to interact. Not working or being unemployed, carries well-recognized risks to health including increased risk of depressive and anxiety disorders, demoralization, and suicide (Bartley, 1997; Fryers, Melzer, & Jenkins, 2003).
One characteristic of the workplace is that it often implies shared exposure to positive or negative influences for health. In this chapter, we critically examine the main models that have linked the work environment to mental health and illness, the association of specific occupations with mental health, and the ways in which mental ill health may manifest itself in the workplace. We then document research that has identified populations that may be particularly vulnerable to workplace stressors. We consider research on gender, sexuality, ethnicity, age, learning disabilities, and preexisting mental health, in this context. Finally, we examine interventions in the workplace, at both the individual and the organizational levels that have been carried out with a view to preventing mental ill health. We look at the strengths and limitations of different interventions strategies, as well as the limitations of the research that has evaluated them.
Psychosocial Work Environment
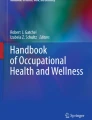
Several models have been devised to understand the hazards and benefits of the psychosocial work environment and its link to risks of physical and mental ill health. One of the most influential models has been Karasek’s Job Strain Model, also called the Demand–Control Model (Karasek & Theorell, 1990) (Fig. 10.1). This model comprises two key dimensions: psychological work demands and decision latitude. Decision latitude is made up of control over work (decision authority), the variety of work, and opportunity for use of skills (skill discretion). According to the Job Strain Model, jobs can be classified into four types:

Karasek’s job strain model
-
1.
The most risky types of job for health are high-strain jobs typified by high psychological demands and low decision latitude.
-
2.
Low-strain jobs with few psychological demands and high levels of decision latitude are predicted to have lower than average levels of psychological strain and lower risk of ill health because there are relatively few challenges, and decision latitude allows the worker to respond optimally to these few challenges.
-
3.
Active jobs with high levels of demands and high levels of decision latitude can be rewarding but also may be associated with higher levels of mental ill health because of the relatively potent effect of high demands.
-
4.
Passive jobs typified by low demands and low control can be demotivating and involve the atrophy of skills and abilities, but only average levels of psychological strain and health risk are expected.
A refinement of this model is the addition by Johnson, Hall, and Theorell (1989) of the further dimension of occupational social support. The revised model, so-called Demand–Control–Support or Iso-Strain Model, includes support received from supervisors and coworkers that may buffer the effect of high demands and low control. Within this model, decision latitude (or control over work) and social support are the positive effects that may relate to better mental health and well-being.
Indeed, there is evidence to support this model. Adverse psychosocial work characteristics have been associated with increased risk of depressive symptoms (Marchand, Demers, & Durand, 2005; Rugulies, Bültmann, Aust, & Burr, 2006) and common mental disorder (Bültmann, Kant, van den Brandt, & Kasl, 2002; Stansfeld, Bosma, Hemingway, & Marmot, 1998). A recent meta-analysis identified job strain, high demands, and low social support as consistent risk factors for common mental disorder (Stansfeld & Candy, 2006). Job strain has also been associated with increased risk of cardiovascular disease (Bosma et al., 1997; Johnson & Hall, 1988; Schnall et al., 1990).
The Effort Reward Imbalance is an alternative model of the psychosocial work environment (Siegrist, Peter, & Junge, 1990). According to this model, work offers opportunities for people to gain esteem, efficacy, and integration. It is based on the social exchange theory where workers invest effort in work and expect rewards in return. If there is an imbalance between the efforts invested and the reward received then psychological distress occurs with physiological arousal. The effort side of the equation includes both intrinsic effort, which measures people’s innate competitiveness, hostility, and involvement with work, and high extrinsic work demands, similar to those measured by Karasek’s Model. These efforts are balanced by reward in terms of salary, promotion, or esteem. An imbalance between efforts and rewards has been related to both psychological ill health and physical ill health (Bosma, Peter, Siegrist, & Marmot, 1998; van Vegchel, de Jonge, Bosma, & Schaufeli, 2005).
Other aspects of the work environment have been identified as possibly problematic for health. One involves the concept of organizational justice that has been explored by a Finnish group in a large sample of male and female hospital workers both cross-sectionally and longitudinally in relation to depression (Ylipaavalniemi et al., 2005). Organizational justice implies that issues at work are dealt with fairly without discrimination and for all employees. Lack of organizational justice has been related to an increased risk of common mental disorders for both men and women (Ybema & van den Bos, 2010). Another important workplace stressor is bullying, usually involving senior employees bullying more junior employees. In a prospective study with female and male hospital employees in Finland, a fourfold increase in risk of common mental disorder over a 2-year period was related to prolonged workplace bullying (Kivimäki et al., 2003). Furthermore, discrimination at work may be related to common mental disorders, and racial or ethnic discrimination has been found to be associated with an increased risk of common mental disorders in a UK studies (Bhui et al., 2005; Wadsworth et al., 2007). Other issues include long work hours and shift work, which have been found to be associated with common mental disorders although the results are not consistent across all studies (Tucker & Knowles, 2008). The association of evening shifts with mental ill health may also suggest a selection factor in that people who are distressed may choose certain shifts.
Criticisms of the Psychosocial Environment Model
Many of the studies that relate psychosocial work characteristics to mental health or coronary heart disease have been criticized because the assessment of work characteristics is based on self-report. Self-report is open to bias from negative affectivity where people have a tendency to report negatively about both their environment and their health. Some studies have overcome this problem by assessing mean values for psychosocial work characteristics related to work groups rather than individuals. Other studies, particularly those in relation to cardiovascular mortality, have classified types of jobs in terms of demands, control, and support and have then related mortality to occupations classified in this way (e.g., Johnson et al., 1989). Other methods to deal with this problem have been to use reports from managers on control and demands in specific posts rather than from individuals, but these have not always been successful as managers may not always be sufficiently informed about the nature of jobs (Stansfeld et al., 1995). A more successful method has been adopted by Virtanen and colleagues (2008) who used an objective measure of work demands in a cohort of hospital workers and related that to sickness absence for depression and prescription of antidepressants in the staff. The objective measure was the percentage of bed occupancy on the ward, which relates directly to the amount of work staff have to carry out and to perceptions of overcrowding and work strain. Thus, although reporting bias may be a feature of associations between the work environment and mental health, using measures that are not susceptible to bias also seems to show the same effects, albeit not as strongly. The observation of a less strong effect might be because bias does indeed contribute to the aforementioned studies of self-reported exposure or because Virtanen’s approach does not comprehensively measure environmental stressors.
Occupation and Mental Health
Different occupations are associated with different risks of mental ill health and sickness absence. Many studies have shown fairly consistently high rates for workers in health-related professions, particularly those involved in direct caring, and for teachers in primary and secondary schools, sales personnel, and managers. High rates in these occupations have been shown across Danish, UK, and US studies (Eaton, Anthony, Mandel, & Garrison, 1990; Stansfeld, Rasul, Head, & Singleton, 2011; Wieclaw et al., 2008). However, there are also many variations between studies as to which occupations are most at risk. In many at-risk occupations emotional demands are evident, where people are looking after others but often have to suppress their own emotions. In some occupations low status, low pay, and poor conditions are clearly responsible for increased mental health risk (e.g., kitchen porters). Exposure to violence and public criticism may also be risk factors for mental ill health. Another issue is occupational exposure to alcohol; bar staff had high rates of common mental disorder (29 %) in the 2000 Adult Psychiatric Morbidity Survey presumably partly related to easy access to alcohol, a known risk factor for common mental disorder (Stansfeld et al., 2011). One interesting finding is that occupations within different industry sectors may be more or less at risk. For instance, clerical and secretarial staffs in health-related occupations seem to have lower risk than similar occupations in the construction industry (Stansfeld et al., 2011). There may also be some occupations with dangerous conditions that are preferentially selected by people who have special qualities of resilience and have good mental health.
Selection in Occupations
One possible alternative explanation for higher rates of mental disorders in certain occupations relates to the possibility of selection into jobs according to personality. It is possible that people with health problems, in either themselves or their families, are more likely to work in health-related occupations carrying their preexisting risk for ill health into the occupation. At the other end of the scale, people with qualities of toughness and resilience may be selected into potentially dangerous or risky jobs that they enjoy and such people may be less susceptible to mental health problems. There have been few studies to definitively answer these questions, and it is difficult to separate the effects of selection from those related to the predominant work culture. For instance, men working in predominantly female occupations and vice versa have also been found to have a higher risk for mental disorders (Wieclaw, Agerbo, Mortensen, & Bonde, 2006). In this case, it is difficult to be certain whether high risk relates to selection or to being made to feel an outsider in a particular work culture. Work culture is also particularly important in its own right and may influence the relationship between the employee and the employer and the ability of the employee to take sickness absence when ill (Johns & Nicholson, 1982). One issue that should not be discounted is the finding that childhood mental ill health predicts that the adults may find themselves in poor working conditions (Clark, Caldwell, Power, & Stansfeld, 2010; Stansfeld, Clark, Caldwell, Rodgers, & Power, 2008, Stansfeld et al., 2008). It seems likely that this represents health selection in which the disturbance of functioning associated with childhood psychological distress may impair education and mean selection into less favorable jobs.
Presenteeism, Productivity, and Sickness Absence
Mental ill health in employees can be expressed in different ways. Employees may, for instance, experience depressive and anxious symptoms but still remain at work. In this case, so-called presenteeism and their functioning and productivity may be affected but the symptoms may not be reported or treated, perhaps for fear of job loss. Alternatively, employees may take time off work with sickness absence, either short spells (usually less than 7 days) or long spells, which need medical certification. Long spells of sickness absence often indicate illness (Marmot, Feeney, Shipley, North, & Syme, 1995), but the determinants of sickness absence are complex. Mental health symptoms predict sickness absence in many studies (Bültmann et al., 2005, 2006). Occupation is also related to sickness absence (Hensing, Andersson, & Brage, 2006). However, recent studies also suggest that the roots of sickness absence may lie in childhood during which absence from school and neurotic symptoms in childhood predict longer term sickness absence and disability (Henderson, Hotopf, & Leon, 2009). Moreover, habits of work learned from parents, coping style and personality, current perceptions of health anxiety and personal vulnerability, and attitudes about work and employment may all contribute to a more complex model of the etiology of sickness absence. Thus, it is no longer satisfactory simply to blame rates of sickness absence on conditions in the workplace.
Increases in Work-Related Stress Disorders
It is interesting that in both the UK (Stansfeld, Clark, et al., 2008, Stansfeld, Woodley Jones, et al., 2008) and Norway rates of sickness absence have increased across the 1990s, possibly decreasing or plateauing slightly since then (Hensing et al., 2006). The increased rates seem to relate particularly to anxiety disorders, neurotic conditions, and depression and not psychoses (Hensing et al., 2006). There is no clear reason why this is the case, but it may be that employees have a greater readiness to report work stress and that mental health conditions are both better recognized and more acceptable as a cause of sickness absence. Although an increase in stressful working conditions has been proposed, on the whole, this does not seem a plausible explanation as rates of common mental disorders in the general community do not seem to have increased over the same period. Undoubtedly, the nature of jobs has changed in recent years, but whether occupations are generally more stressful is open to question. Certainly, the constantly evolving nature of work and workplaces means that any preventive interventions have to be fit for contemporary working conditions.
Physical Environment of the Workplace
One issue that should be considered is the physical environment of the workplace. The type of ventilation of buildings, exposure to chemicals, access to natural light, and the amount of control employees have over such things as opening windows and where their workstations are placed have all been related to symptoms (Raw, Roys, & Leaman, 1993). There is a considerable literature on sick building syndrome suggesting that certain buildings are bad for health. However, much of this literature does not take into account the psychosocial work environment. A London-based study of civil servants that included both the psychosocial work environment and physical measures of the workplace found that psychosocial variables had a greater influence on symptom measures than did the physical characteristics of the environment, although there were small effects for the ability to control the environment such as the type of ventilation (Marmot et al., 2006).
Vulnerable Groups
A large body of research has documented that some social groups are more vulnerable than others in developing mental health and behavioral problems at work. This research has mainly focused on exposure to experiences of discrimination and stigmatization (Mays & Cochran, 2001). Most of the research on vulnerable groups at work has focused on gender, ethnicity or ethnic minority status, sexuality, mental illness, and learning disability. In particular, research has shown that experiences of discrimination, harassment, and stigmatization can have deleterious effects and lead to great vulnerability to depressive and anxiety disorders, distress, low self-esteem, and alcohol and substance abuse (Mays & Cochran, 2001; Rospenda, Richman, & Shannon, 2009). Negative workplace interactions that are experienced routinely have even been linked to a greater risk of stress-induced mental health problems than major life events (Nawyn, Richman, Rospenda, & Tonda, 2000).
Researchers have focused on specific vulnerable groups to explore how harassment and/or discrimination at work affect mental health and behavioral disorders. There are a lot of similarities between different vulnerable groups on how harassment and/or discrimination impacts mental health. However, each group faces unique challenges because harassment and/or discrimination is manifested through different facets of one’s identity—for example, one’s gender in the case of sexual harassment and race or ethnicity in the case of racial harassment (Rospenda & Richman, 2005). In the following section we present a brief review of this research on specific vulnerable groups at the workplace.
Gender
As women’s participation in the labor market has been steadily increasing over the past few decades, research on the relationship between women’s occupational status in relation to their psychological and mental health has been prolific (McDermott, 2006; Nordenmark, 2002; O’Campo, Eaton, & Muntaner, 2004; Raver, 2003). Sexual harassment exists for men and women and can create a stressful environment at work for both. However, past research has consistently shown that women constitute the great majority of sexual harassment victims (e.g., Rospenda et al., 2009). Indeed, according to the US Equal Employment Opportunity Commission, more than 85 % of the sexual harassment charges across the country were filed by women (Lim & Cortina, 2005).
Numerous studies have documented a plethora of negative outcomes among targets of sexual harassment (e.g., Fitzgerald, Magley, Drasgow, & Waldo, 1999; Rospenda, Richman, Wislar, & Flaherty, 2000). These include job-related consequences (e.g., negative job attitudes, turnover intentions, decreased job satisfaction, organizational commitment), psychological problems (e.g., fear, anxiety, depression), and impaired health (e.g., psychosomatic symptoms) (Lim & Cortina, 2005; Morrow, McElroy, & Phillips, 1994; Ragins & Scandura, 1995). Research has shown that sexual harassment victims frequently suffer from the same types of problems associated with other major workplace stressors. These include increased incidence of psychosomatic illness, reduced concentration, and negative mood (Barling et al., 1996). Prolonged chronic exposure to sexual harassment may cause severe emotional strain and the subsequent disabling symptoms associated with this condition (Dekker & Barling, 1998). Female targets also experience tension, anger, and anxiety, whereas a more limited number experience depression or guilt (Baugh, 1997).
Sexuality
In terms of sexual identity, gay men, lesbians, and bisexual men and women are vulnerable to everyday negative interactions (DiPlacido, 1998), but workplace harassment has been found to be a particularly problematic work stressor for these groups. Workplace harassment can be particularly stressful for gay, lesbian, and bisexual employees because it can be compounded by (or result from) preexisting expressions of homophobia or perceived vulnerability in one’s job due to one’s sexual orientation (Nawyn et al., 2000). Studies have reported a high prevalence of verbal insults, threats of violence, and actual violence for gay and lesbian employees compared with their heterosexual counterparts (Norris, 1991) as well as much more sexually harassing behaviors reported by lesbians compared with heterosexual women (Nawyn et al., 2000). An additional workplace stressor for lesbian, gay, and bisexual men and women is related to disclosure of harassing behaviors as studies have found that they rarely report the incident of harassment out of fear of public exposure and, thus, additional harassment (Herek & Glunt, 1993).
The choice of deciding whether to disclose a harassing behavior involves psychological demands that exacerbate stress (Greene, 1994; Woods, 1993). Openness about sexual orientation at the workplace can have an impact at many different levels. It can threaten job security, which is particularly important for lesbians and bisexual women who generally have less financial support from male partners (Dunne, 1997). At its most extreme, lesbians and gay men may be refused a job or may be dismissed (Palmer, 1993) because of their known or perceived sexuality. Less severe, but often equally distressing, is workplace ostracization (Dunne, 1997; Humphrey, 1999), which can take many different forms such as refusing to speak or avoiding contact with a lesbian or a gay colleague, lack of management support for lesbian and gay workers, or refusing to share facilities, such as changing rooms, communal showers, or sleeping accommodation (Skidmore, 2004).
In both US studies and the more limited body of UK research, hostility to homosexuality in the workplace has been found to induce feelings of anxiety, fear, anger, discomfort, worry, and stress (Clarke, 1996; Sorensen & Roberts, 1997), and experiences of occupational heterosexism have been shown to be positively related to depression and psychological distress (Ingram & Smith, 2004; McDermott, 2006). Stress at the workplace can have a significant effect on the general quality of life and satisfaction with life and can lead in many cases to a number of negative behaviors; for example, studies have found that lesbians and gay and bisexual men are more likely than their heterosexual counterparts to engage in excessive alcohol consumption to cope with the stress (Nawyn et al., 2000).
Ethnicity/Race
A large volume of literature on ethnicity and mental health links mental health problems to racial discrimination (Bhui et al., 2005; McKenzie, 2003; Miller & Travers, 2005; Nazroo, 1997, 2003). Racial discrimination is known to be an important risk factor for mental illness in the US (Darity, 2003; Murray, 2003) and UK (Bhui et al., 2005; Wadsworth et al., 2007) workforces. For example, findings from the USA indicate that racial bias, in terms of both institutional and interpersonal prejudice at work, was a more important predictor of job satisfaction among African American women than other occupational stressors, such as low decision authority and heavy workload (Hughes & Dodge, 1997), and that racial discrimination affects job stress among Black women (Mays, Coleman, & Jackson, 1996). Similarly, research in the UK indicated that almost twice as many non-White respondents reported high or extremely high stress at work compared with White respondents (Smith, Johal, Wadsworth, Davey, & Peters, 2000).
Further research suggests that ethnic minorities are highly exposed to work-related stress (e.g., Miller & Travers, 2005) and that long-term illness in the working population shows significant associations with ethnicity (Census, 2001). Most studies on ethnicity and work link work-related stress to the discrimination experienced at the workplace, which can affect one’s sense of control in the work environment as well as workload and opportunities for career development (Bhui et al., 2005). Stress and common mental disorders, which are a result of racial discrimination, can further affect occupational functioning (Bhui et al., 2005). Research also suggests that the interaction between gender and ethnicity can be important when considering the groups that may be more at risk for work-related stress. For example, a well-documented finding is that Black African and Black Caribbean women may be particularly at risk of stress at work (Wadsworth et al., 2007).
Mental Illness
For people with mental health problems, being in paid employment is very important for their recovery. Employment tends to be a significant factor in rehabilitation programs as it has been shown to have a direct relationship with improvements in a number of outcomes such as self-esteem, social support and networks, and psychiatric symptoms (Cook & Razzano, 2000). It is a well-documented finding that people with mental health problems are stigmatized by society and are subjected to discrimination from employers (Stuart, 2006). For example, population surveys have shown that people with mental health problems are significantly more likely to be unemployed than people without mental health problems; in particular, a large-scale population survey found that 61 % of people with mental health problems were unemployed compared with 20 % of the general population (Cook et al., 2005). Unemployment rates also vary by diagnosis, with people suffering from severe mental health problems (e.g., schizophrenia) having the highest unemployment rates (Crowther, Marshall, Bond, & Huxley, 2001).
In addition, people with mental health problems who are in paid employment are less likely to be in prestigious and/or high-earning positions (Chandler, Meisel, Jordan, Rienzi, & Goodwin, 2005) and more likely to be doing unskilled menial jobs and/or be in part-time employment (Rosenheck et al., 2006). Employees with mental health problems may also experience stigma and discrimination from coworkers once their mental illness becomes known. Workers who return to their jobs after an illness report returning to positions of reduced responsibility with enhanced supervision where they are socially marginalized and become targets for mean-spirited or negative comments from workmates who had previously been supportive and friendly (Cook et al., 2005; Schulze & Angermeyer, 2003). Half of the competitive jobs acquired by people with a serious mental illness will end unsatisfactorily as a result of problems that occur once the job is in progress, largely as a result of interpersonal difficulties (Becker et al., 1998; Stuart, 2006).
Similar to other high-risk groups discussed in this section (e.g., lesbians and gay men, people with learning disabilities), people with mental health problems often find themselves in the stressful situation of whether to disclose their illness (Stuart, 2006). For example, research has shown that people with mental health problems who are employed may not take part in employee assistance programs and may avoid receiving treatment/medication to make sure that their illness is concealed from their colleagues, managers, and employers (Stuart, 2004). Even when people decide to disclose their mental health problems, many organizations (most likely the small ones) will not have sufficient programs in place to address such health problems (Gray, 2000; Harnois & Bagriel, 2000) and managers will not have the knowledge or the skills to effectively manage mental health problems at the workplace (Stuart, 2006).
The relationship between work and psychosis such as schizophrenia differs from that between work and common mental disorders. Many people with psychosis are severely disabled with both positive symptoms—persisting delusions and hallucinations—and often more disabling, negative symptoms such as apathy, neglect, and social withdrawal that interfere with the ability to work. For people with chronic schizophrenia there are many benefits of working in relation to social status, structure of the day, availability of social networks, and self-esteem (Velligan & Gonzalez, 2007). Regrettably there are sometimes perverse incentives that mean that potential employees have a financial incentive to remain on benefits rather than to return to work. There has been considerable success in getting unemployed people with serious mental illness back into work through the individual placement and support program that supports both the patient and the employer in placing the person with serious mental illness in open employment (Burns et al., 2007). The disadvantage of these jobs is that many are entry-level or part-time jobs where the work characteristics are fairly poor. Nevertheless, working in such jobs may be better than no job at all because lack of activity and poverty of environment can be particularly damaging to people with chronic psychotic illnesses (Wing, 1970). Because there has been fairly little research on the effect of working conditions on people with serious mental illness, this will not be a major focus of the chapter.
Learning Disabilities
A great deal of what has been discussed in relation to people with mental health problems applies to people with learning disabilities (LDs) in terms of disclosure, type of job, and earnings. A further contributing factor is that a significant proportion of people with LDs suffer from mental health problems (Smiley, 2005), which is believed to partly stem from the socioeconomic disadvantage and related social exclusion that people with LDs tend to experience. In particular, according to figures from the Office for National Statistics in the UK, only 17 % of working-age people with learning difficulties had a paying job compared with 67 % of men and 53 % of women without LDs (Emerson & Hatton, 2007). For those people with LDs in paid employment, research has shown that they are more likely to be in part-time employment and earn a lot less than people without LDs (Madaus, Foley, McGuire, & Ruban, 2002).
Although people with LDs are suggested to be one of the most vulnerable groups at the workplace, research on their experiences at work and how these experiences affect mental health is scarce. The little research that exists focuses mainly on whether people with LDs find satisfying employment as well as issues of disclosure. Self-disclosure is an intensely personal and complex decision, as the costs and benefits of disclosure must be weighed against a variety of concerns (Baldridge & Veiga, 2001; Gerber & Price, 2003; Hughes & Williams, 1994). A study found that although 80 % indicated that their LDs affected their work in some way, only 20 % self-disclosed their LD status during the interview process and 43 % self-disclosed after they were hired (Madaus, 2008).
Age
Although the term “ageism” was used to refer to the process of stereotyping and discrimination against people perceived as too old, it has now come to refer more broadly to prejudice and discrimination on the grounds of either being too old or too young (e.g., Palmore, 1990). For example, a survey of undergraduate students showed that over one-third of the participants reported experiences of age-related discrimination (Duncan & Loretto, 2004; Loretto, Duncan, & White, 2000).
Most studies on the impact of age discrimination on the employee have mainly focused on career rather than on mental health. In particular, studies of performance appraisal report older employees receive lower performance ratings than their younger counterparts (Saks & Waldman, 1998) and they are more likely than their younger counterparts to experience discrimination in access to training and development opportunities (Department of Employment, 1994) as well as promotion opportunities (Palmore, 1990). Older workers are also more likely to be selected for redundancy than are middle-age workers (Snape & Redman, 2003). Young people who by definition have little experience and skills face great difficulties in finding the right employment and are often underemployed (Barling & Kelloway, 1999; Lindley, 1996), seen as untrustworthy, and given less responsibility (Loretto et al., 2000).
The small number of studies that explored the impact of ageism on an employee’s economic and psychological well-being has largely focused on older employees. For example, on leaving the workforce, older workers find it much more difficult to reenter it (Sargeant, 2001) and experience longer periods of unemployment between jobs than their younger counterparts (McGregor & Gray, 2001). Greater prospects of redundancy are also likely to be particularly stressful for older workers if there is little likelihood of obtaining meaningful work ever again (Wood, Wilkinson, & Harcourt, 2008). Furthermore, those who feel that they have been discriminated against because of their age may feel under-rewarded in terms of pay and status, while discriminatory treatment in general may create a sense of being undervalued by the organization (Hassell & Perrewe, 1993), which can lead to mental health problems such as negative affective states (Gutek, Cohen &, Tsui, 1996) and stress (Snape & Redman, 2003). Moreover, those experiencing discrimination will feel less loyal and have a lower level of identification with the organization and will feel unsupported (Snape & Redman, 2003).
Conclusion
Harassment and discrimination in the workplace take many forms and can occur for a variety of reasons such as one’s gender, sexuality, race/ethnicity, or age. Furthermore, these vulnerability factors can interact. For example, age discrimination can incorporate a gender dimension, with older women being particularly negatively stereotyped (Duncan & Loretto, 2004; Schuman & Kleiner, 2001; Walker, 2005; Wood et al., 2008). Evandrou and Glaser (2004) note that, having fulfilled child-raising and other family social care obligations, older women are very much more likely to face poverty in their old age. Research has also found that African Caribbean women may be particularly at risk of work stress and its consequences because of the potential for gender and/or racial bias that may have been apparent for sometime (Wadsworth et al., 2007). While gender, race/ethnicity, and age may be at interplay, other sources of powerlessness (e.g., sexual orientation) merit future attention. For example, although sexuality is not the same as gender, it cannot be understood without reference to it in the context of organizations (Skidmore, 2004). Therefore, multiple social statuses, such as gender, sexuality, age, race/ethnicity, education, and income, may influence cumulatively specific psychiatric vulnerabilities among individuals at the workplace in ways that are not yet understood.
Interventions in the Workplace
We have already outlined theoretical models for workplace effects on mental health. It should follow that workplace interventions could be designed to prevent, screen for, or treat common mental disorders, as well as promote well-being.
Indeed, from a public health point of view, the workplace is logistically attractive for the delivery of preventive interventions in mental health, given its established infrastructure and the numbers of adults who are located there. Moreover, it is a potentially advantageous corporate strategy; research has linked depression and other mental health problems to impaired work performance, absenteeism, and premature retirement (Haslam, Atkinson, Brown, & Haslam, 2005; Sanderson & Andrews, 2006). That said, to actually make changes to improve the workplace environment can be challenging for a variety of reasons. A separate challenge is to prove the effectiveness of any specific intervention as systematically and rigorously as possible.
In this section, types of workplace interventions are categorized and related to the models of the psychosocial work environment as outlined earlier in this chapter. We then turn to studies on workplace interventions, particularly on interventions that target the workplace environment itself, for an assessment of their efficacy for mental health. Gaps in the literature, as well as the limitations of workplace intervention research, are identified, and recommendations are made regarding the future direction that research should take.
Categorizing Intervention Strategies
Preventive interventions can be categorized into primary, secondary, and tertiary strategies. These are differentiated by the timing of their implementation in the disease process (Couser, 2008). In the context of mental health in the workplace, primary prevention is the universal application of an intervention to all individuals within a defined workplace population to protect them from mental ill health; secondary prevention involves intervention after a process of selecting/screening for those with risk factors for mental health problems; and tertiary prevention are measures to treat and reduce the disability related to mental health problems of those who have already developed them.
Intervention strategies may also be categorized according to the organizational level at which the interventions are made. In relation to the workplace, they may be located at the legislative or policy level (i.e., outside the workplace itself), at the employer level, at the level of the job/task occupied by individuals, and at the level of individuals. Specific strategies for primary, secondary, and tertiary workplace interventions at these four different levels have been provided by the National Institute for Occupational Safety and Health (NIOSH), with additions made by Landsbergis (2009) (Table 10.1). For example, Europe-wide initiatives at the legislative level have included a European Union directive in 1989 to “alleviate monotonous work at predetermined pace,” a European Commission Guidance document on work-related stress in 2000, and an agreement by major employers and unions in Europe in 2004 that obliges employers to protect employees from work-related stress. Interventions at the employer level tend to target human resources policies and the working environment by making it more supportive. Interventions at the task/job level, as well as the employer level, have been responsible for introducing increased job control and participation in decision-making, job enrichment, and job redesign, whereas interventions at the individual level often involve targeted programs such as health promotion programs (Landsbergis, 2009). Of course, any one prevention strategy may involve interventions at several levels, each mutually reinforcing the other. Moreover, it may be more effective to intervene at both organizational and individual levels simultaneously.
Designing Intervention Strategies
Given this available range of intervention strategies, which one should an organization choose to improve its working environment?
Where the workplace itself is likely to generate widespread mental illness risks, it may be more efficacious to adopt primary intervention strategies. These would target the occupational- and employment-related factors responsible for increasing risk (e.g., taking steps to reduce the risk of exposure to violence in staff dealing with a potentially hostile client group). Primary prevention strategies are applied across the entirety of a defined population and, hence, could have far-reaching benefits on workforce morale. However, given their universal target, they might be thinly applied. Therefore, where risk is restricted to a few and appears in clusters, primary prevention strategies could waste resources on those who don’t need help, while not doing enough to help those who do need it.
In such a situation, it may be more efficacious to adopt a secondary prevention strategy, particularly where impact of the workplace adversity is strong and at-risk groups readily identifiable. These strategies might tackle discrimination in high-risk social groups, as discussed earlier in this chapter. However, a secondary prevention strategy can come with difficulties: it may in itself be perceived as discriminatory, invite feelings of victimization, and be ultimately counterproductive. Secondary intervention strategies must, therefore, be carefully designed to best maintain privacy and dignity.
The efficacy of interventions will also depend on whether they correctly identify the most pertinent problems and succeed in addressing them. Theories such as the Demand–Control Model, the Iso-Strain Model, the Effort Reward Imbalance Model, and “organizational justice” play a crucial role in this regard, in that they provide models against which the psychosocial environment of any workplace may be assessed and improved. Employer- and job-level approaches are theoretically best suited to make changes based on these models and may be most effective in practice, especially if sustainable improvements in working conditions are to be achieved.
Lastly, mental health problems are associated with some occupations more than others. As already discussed, this may be because individuals self-select into occupations according to their personality and predilections or may be a true effect of the job. So, for example, although the highest rates of mortality from alcohol abuse are found among bar workers and publicans (Romeri, Baker, & Griffiths, 2007), this may be due to the predisposition of individuals attracted to the industry rather than the opportunities for alcohol consumption that these occupations offer. Explanations for the high rates of substance abuse among anaesthesiologists compared with other medical specialists may be subject to a similar debate (Bryson & Silverstein, 2008). Whether a primary or secondary intervention strategy is adopted will largely depend on the strength of the evidence supporting the “opportunities” model, which invites a primary intervention strategy at the organizational/occupational level, versus the “self-selection” model, which invites a secondary intervention strategy at the individual level.
Indeed, the success or failure of interventions that have been devised under the influence of specific theoretical models may themselves be employed to lend or reduce support for the models by which they have been shaped. The questions that now concern us are what evidence exists for the success and validity of recent interventions that target the workplace? How useful are they for promoting our understanding of the links among psychosocial aspects of the work environment, mental well-being, and mental health problems? And how can they inform future policy and practice in the workplace?
The Use of Meta-analysis
Firstly, is there evidence to suggest that workplace interventions can improve mental health? To answer this question, it may be useful to consider the findings of meta-analyses that have reviewed this literature. Because they pool data from a large number of studies, meta-analyses may provide us with shortcut answers to questions of effectiveness. And because they select only those studies that meet specified scientific criteria, they may also narrow the field to those studies that are methodologically robust.
Most meta-analyses of the recent literature on interventions in the workplace do indeed find a small but statistically significant overall benefit of workplace interventions on outcome measures such as absenteeism, psychological distress, and anxiety/depression scales (Table 10.2). These meta-analyses focused on a variety of intervention strategies. What is disappointing, however, is that most meta-analyses include very few studies that directly target employer-/job-level risk factors (e.g., poor psychosocial work environment), which is the main topic of this chapter and probably the most important causal link between the workplace and poor mental health. For example, in a meta-analysis of 48 studies of interventions to reduce occupational stress between 1977 and 1996, van der Klink and colleagues (2001) found only five studies that were targeted at the employer/job level. Instead, by depending on changes at an individual level (such as stress management or cognitive behavioral therapy [CBT]), these studies are merely using the workplace to roll out healthcare interventions and not intervening in the workplace environment itself. Why is this happening? The lack of organizational interventions in meta-analyses presumably reflects the difficulty in organizing randomized and controlled versions of employer-level trials (Gardell & Gustavsen, 1980), which are therefore being omitted from meta-analyses in the pursuit of scientific rigor. One reviewer, for example, found them “difficult to interpret, causally ambiguous, inconsistent, based on small samples and/or statistically insignificant” (Parkes & Sparkes, 1998).
If meta-analyses cannot provide shortcut answers as to the efficacy of interventions at the employer/job level, we must instead look to data from individual studies.
Evaluating Organizational Interventions: Action Research
One promising organizational approach has involved and empowered those in the workplace to identify problems in, and emanating from, the workplace, as well as involved them in the development of interventions to change these problems and measure their effects. Referred to commonly as action research, it has been common in Scandinavia (International Labour Organization, 1992). For example, the involvement of bus drivers in action research to reduce stress and improve their health was responsible for identifying and changing several aspects of job design, such as lanes and routes, signal priority, and bus stops. This led to a significant decline in reported “job hassles per hour” as well as systolic blood pressure (Poulsen, Jensen, Bach, & Schostak, 2007). Indeed, a number of reviews have suggested that the most promising interventions at the organizational level are those that have included the meaningful participation of employees (LaMotagne, Keegel, Louie, Ostry, & Landsbergis, 2007; Parker, Jackson, Sprigg, & Whybrow, 1998; Semmer, 2006).
This approach might be seen to act through Karasek’s Job Control Model, since control, demand, and/or support could theoretically be improved. Egan and colleagues (2007) performed a systematic review of action research studies to test Karasek’s Model. Of 18 identified studies, nearly all evaluated interventions involving “problem-solving” or “participatory” committees of employee representatives that aimed to tackle workplace stressors. Some studies combined this with individual-level interventions, such as relaxation techniques. One should note that no studies were randomized, and many contained non-matched groups for comparison.
Nevertheless, it is interesting that of the eight studies to report overall post-intervention improvement in job control/participation, seven also reported significant overall health improvements (such as improvement in mental health questionnaire scores). Four studies reported decreased job demands after the intervention and were accompanied by improved health outcome in each instance. Improved support was also associated with improved health in the majority of studies in which it was measured. In those studies where control, demand, or support were recorded as unchanged or worsened, health outcomes often remained unchanged (Egan et al., 2007).
Collectively, these observations go some way to broadly supporting the individual components—control, demand, and support—of Karasek’s Job Control Model. However, no one study within the systematic review measured and improved on all three components in a meaningful way, and no studies correlated the association between these components and health outcomes within individuals. To follow Karasek’s Model more explicitly might benefit the design and success of future studies.
It is also worth noting that only two studies stratified outcomes by “at risk groups.” Those that did suggested that lower grade workers and employees from ethnic minorities might benefit most from interventions (Park, Schaffer, & Griffin-Blake, 2004; Parker, Chmiel, & Wall, 1997). Future studies should aim to gather such data, as they could support a role for interventions in decreasing healthcare inequalities.
Workplace Reorganization Strategies
To make a large and lasting improvement on mental health in the workplace, it might be that interventions have to target fundamental workplace reorganization.
For example, there has been a long tradition of workplace research that examined the impact of assembly line production, the dominant mode of work organization of the early twentieth century that is often referred to as “Fordism” or “Taylorism,” and reported findings of burnout, stress-related illness, alienation, and absenteeism (Landsbergis, Cahill, & Schnall, 1999). As a result, new systems of work organization have been introduced to replace the assembly line. However, evaluation of the effects of these new systems has taken various forms, appears to depend on political circumstances and the power of the labor movement, and frequently avoids examination of mental health effects altogether. For example, the Japanese lean production approach, which was devised to replace the assembly line, has been evaluated more in terms of the interests of management and shareholders, such as productivity, profitability, and product quality (Landsbergis et al., 1999) and less for its effects on employees.
In Sweden and Norway, by contrast, changes to the organization of work have not only been evaluated in terms of their health outcomes, but the interventions have been designed with this in mind. Research in the 1960s and 1970s had demonstrated the impact of the assembly line, with its monotonous and repetitive machine-paced work, on mental and physical health (Gardell & Gustavsen, 1980). Evaluations of work–life programs in Sweden and Norway reportedly provide evidence of the impact of increased job control on work and life satisfaction, as well as improvements in productivity (Levi, 2000). The work humanization interventions in the late 1980s and early 1990s at Saab and Volvo may be singled out for special mention. Instead of the 60-s cycle times of the typical assembly line, parallel teams built complete cars with cycle times of 1.5–7 h. Unfortunately, the closure of the plant prevented adequate evaluation of the parallel teams experiment for its impact on chronic illnesses and absenteeism.
Further workplace reorganization interventions have been evaluated for their impact on mental health. Bambra and colleagues (2007) performed a systematic review of workplace reorganization studies and found 19 studies with control/comparison groups, although no randomized studies. Eight of these studies aimed to introduce more job-task variety, for example, by allowing healthcare workers or production line workers more breadth in their tasks and responsibilities. Seven different studies aimed to promote teamwork and increase the collective responsibility and decision-making power of the employees. Six studies aimed to increase autonomy and collective involvement, for example, by using the “lean production” or “just-in-time” models of mass production rather than traditional assembly lines. Studies targeted diverse groups including factory workers, doctors, carers, and office workers (Bambra, Egan, Thomas, Petticrew, & Whitehead, 2007).
Results were mixed, with many studies reporting no benefit from the intervention. For example, the job-task variety interventions often failed to increase job control and job demand often increased; mental health benefits were small or not significant at best. The team working interventions did improve the work environment, by increasing support, but did little for health. The autonomous work groups actually worsened the psychosocial work environment, contrary to their aims, with decreased control and autonomy; job anxiety and depression increased in several cases (Bambra et al., 2007).
It is difficult to generalize as to the implications of these studies, because they differ markedly in terms of aim, design, intervention, and outcome measures, and many had non-matched comparison groups. Further, much of the primary literature does not specify exactly what changes were made in specific terms. One should note that many did not actually succeed in changing the psychosocial work environment, nor did they aim to (focusing instead on improving productivity). These economic-driven trials tended to cause negative or negligible health outcomes. One interesting point is that “job control” seemed to influence mental health more than “job demand” and “job support,” suggesting that this might be the most important component in Karasek’s Model in practice although demands have often been found to be more important in observational studies.
Other research has attempted to improve the physical environment, including technological improvements (Kawakami, Araki, & Kawahima, 1997) and advising on posture and lifting (Evanoff, Bohr, & Wolf, 1999). The former study showed no improvement in psychosocial environment, perhaps because the intervention was coupled with an increase in workload. The latter study did report improved musculoskeletal health and reduced absenteeism but did not report mental health outcomes.
Challenges and Future Directions
Evaluations of employer-level interventions that target the effects of workplace stressors on mental health are limited. Where they exist, the evidence has not always been positive and reviewers have found the evidence to be vague, weak, and contradictory (Parkes & Sparkes, 1998). Is this a challenge that can be met?
Firstly, it is clear that information to identify the locations and sources of high risk in the workplace must be gathered more systematically. “Work site surveillance,” as called for in the Tokyo Declaration of 1998, is required both to identify clusters of high risk and to measure work-related stressors and the health problems that result from them (Landsbergis, 2009).
Secondly, study designs must be adjusted to ensure that longer timeframes are included. Evaluations of interventions at the individual level are frequently limited in value by the absence of follow-ups (Martin et al., 2009). While a number of such studies have demonstrated substantial impact, questions have been raised as to the sustainability of these interventions, given the unchanged nature of the workplace itself. In contrast, the effects of interventions at the organizational level may appear weak because they take longer to manifest themselves (Martin et al., 2009; van der Klink et al., 2001). One of the challenges facing the researcher, therefore, is to successfully impress on funders and sponsors the long-term nature of this particular kind of evaluation project. In a climate that demands quick results, this may be more difficult than imagined.
Nevertheless, some initial steps may be taken. If researchers are to promote organizational interventions in the workplace and encourage the replication of evaluations with positive outcomes, they must provide the basic information to make replication possible. Many of the studies that have evaluated organizational interventions have lacked information about the practical details that permit replication, such as details on the nature of the interventions (their content), how they were applied (their process), and their cost to the organization. Promising interventions will only be disseminated, and their evaluation replicated, if potential sponsors and decision makers are provided with careful and detailed documentation of effective intervention initiatives.
Difficulties associated with evaluating interventions are compounded by uncertainties over the nature of the findings and what they represent. This is particularly so in the area of mental health and mental illness, where indicators of health and illness are subject to considerable debate. Hence, clarity about the nature of the effects achieved should be central to any evaluation, as should the enhancement of methodological rigor.
This is no mean task. Many of the studies reported, including interventions targeted at the individual level, rely on subjective rating skills. Some of the measures taken to deal with reporting bias have already been referred to in relation to establishing the links between the psychosocial work environment and risks to physical and mental ill health. However, additional reasons make it difficult for evaluations of interventions at the organizational level to achieve methodological rigor (Kompier, 2003). Firstly, controlled trials are possible, but there are practical difficulties associated with them. Unless there are many groups/plants/offices/work locations that are similar, with some chosen for the intervention by scientific random sampling methods and the others remaining as controls, randomization of the “population” of work sites for intervention is very difficult. Nevertheless, this difficulty is not insurmountable, as exemplified by the WellWorks Project, which conducted a randomized controlled trial on cancer prevention strategies in 24 work sites in Massachusetts (Sorensen, Stoddard, Ockene, Hunt, & Youngstrom, 1996).
Secondly, by virtue of the absence of “blinding,” interventions in the workplace are subject to the same difficulties that accompany all interventions in the social world. In any social intervention study, those subject to the intervention are likely to be aware that some changes have been made to their environment. This can have several consequences for workplace interventions that evaluate for changes in mental health. Because of the intervention, subjects may convince themselves that there have been improvements in their well-being, whether or not this is the case. Alternatively, there may be actual improvements in mental health. However, well-being may have been promoted not because of the substance of the intervention itself, but because of the fact that there was any intervention at all. Often referred to as the Hawthorne effect, after research carried out by Mayo and colleagues in the 1920s and 1930, the awareness of participants that they are subject to an intervention may “tamper” with the results of any social experiment (Landsberger, 1958; Mayo, 1949).
However, the lack of studies that evaluate interventions at the employer level is not only due to the aforementioned methodological challenges. Interventions targeted at individuals appear to be influenced by prevailing political philosophies and associated with the weakening power of labor. Only this can explain such radically different approaches to workplace interventions in Japan, the USA, and Scandinavia. Where individualism dominates, structural causes of ill health (whether mental or physical) are viewed with suspicion whereas lifestyle choices are perceived to be the key to well-being and ill health. Under these circumstances, the most crucial challenge facing researchers may be not only developing robust methods for evaluating organizational interventions but also ensuring that the topic finds itself on the research and development agenda in the first place.
References
Baldridge, D. C., & Veiga, J. F. (2001). Toward a greater understanding of the willingness to request an accommodation: Can requesters’ beliefs disable the Americans with Disabilities Act? Academy of Management Review, 26, 85–99.
Bambra, C., Egan, M., Thomas, S., Petticrew, M., & Whitehead, M. (2007). The psychosocial and health effects of workplace reorganisation: 2, A systematic review of task restructuring interventions. Journal of Epidemiology and Community Health, 61(12), 1028–1037.
Barling, J., Dekker, I., Loughlin, C., Kelloway, K., Fullager, C., & Johnson, D. (1996). Prediction and replication of the organisational and personal consequences of workplace sexual harassment. Journal of Managerial Psychology, 11(5), 4–25.
Barling, J., & Kelloway, E. K. (1999). Young workers: Varieties of experiences. Washington, DC: American Psychological Association.
Bartley, M. (1997). Unemployment and ill health: Understanding the relationship. Journal of Epidemiology and Community Health, 48(4), 333–337.
Baugh, S. G. (1997). On the persistence of sexual harassment in the workplace. Journal of Business Ethics, 16, 899–908.
Becker, D. R., Drake, R. E., Bond, G. R., Xie, H., Dain, B. J., & Harrison, K. (1998). Job terminations among persons with severe mental illness participating in supported employment. Community Mental Health Journal, 34, 71–82.
Bhui, K., Stansfeld, S., McKenzie, K., Karlsen, S., Nazroo, J., & Weich, S. (2005). Racial/ethnic discrimination and common mental disorders among workers: Findings from the EMPIRIC Study of Ethnic Minority Groups in the United Kingdom. American Journal of Public Health, 95, 496–501.
Bosma, H., Marmot, M. G., Hemingway, H., Nicholson, A. C., Brunner, E., & Stansfeld, S. A. (1997). Low job control and risk of coronary heart disease in Whitehall II (prospective cohort) study. British Medical Journal, 314(7080), 558–565.
Bosma, H., Peter, R., Siegrist, J., & Marmot, M. (1998). Two alternative job stress models and the risk of coronary heart disease. American Journal of Public Health, 88(1), 68–74.
Bryson, E. O., & Silverstein, J. H. (2008). Addiction and substance abuse in anesthesiology. Anesthesiology, 109(5), 905–917.
Bültmann, U., Huibers, M. J., van Amelsvoort, L. P., Kant, I., Kasl, S. V., & Swaen, G. M. (2005). Psychological distress, fatigue and long-term sickness absence: Prospective results from the Maastricht Cohort Study. Journal of Occupational and Environmental Medicine, 47(9), 941–947.
Bültmann, U., Kant, I. J., van den Brandt, P. A., & Kasl, S. V. (2002). Psychosocial work characteristics as risk factors for the onset of fatigue and psychological distress: Prospective results from the Maastricht Cohort Study. Psychological Medicine, 32, 333–345.
Bültmann, U., Rugulies, R., Lund, T., Christensen, K. B., Labriola, M., & Burr, H. (2006). Depressive symptoms and the risk of long-term sickness absence: A prospective study among 4747 employees in Denmark. Social Psychiatry and Psychiatric Epidemiology, 41(11), 875–880.
Burns, T., Catty, J., Becker, T., Drake, R. E., Fioritti, A., Knapp, M., et al. (2007). The effectiveness of supported employment for people with severe mental illness: A randomised controlled trial. Lancet, 370(9593), 114652.
Census. (2001). London: Office for National Statistics.
Chandler, D., Meisel, J., Jordan, P., Rienzi, B. M., & Goodwin, S. N. (2005). Mental health, employment, and welfare tenure. Journal of Community Psychology, 33, 587–609.
Clark, C., Caldwell, T., Power, C., & Stansfeld, S. A. (2010). Does the influence of childhood adversity on psychopathology persist across the life course? A 45-year prospective epidemiologic study. Annals of Epidemiology, 20(5), 385–394.
Clarke, G. (1996). Conforming and contesting with (a) difference: How lesbian students and teachers manage their identities. International Studies in Sociology of Education, 6(2), 191–209.
Cook, J. A., Lehman, A. F., Drake, R., McFarlane, W. R., Gold, P. B., & Leff, H. S. (2005). Integration of psychiatric and vocational services: A multisite randomized, controlled trial of supported employment. American Journal of Psychiatry, 162, 1948–1956.
Cook, A., & Razzano, L. (2000). Vocational rehabilitation for persons with schizophrenia: Recent research and implications for practice. Schizophrenia Bulletin, 26, 87–103.
Couser, G. P. (2008). Challenges and opportunities for preventing depression in the workplace: A review of the evidence supporting workplace factors and Interventions. Journal of Occupational and Environmental Medicine, 50, 411–427.
Crowther, R. E., Marshall, M., Bond, G. R., & Huxley, P. (2001). Helping people with severe mental illness to obtain work: Systematic review. British Medical Journal, 322, 204–208.
Darity, W. A., Jr. (2003). Employment discrimination, segregation, and health. American Journal of Public Health, 93, 226–231.
Dekker, I., & Barling, J. (1998). Personal and organizational predictors of workplace sexual harassment of women by men. Journal of Occupational Health Psychology, 3(1), 7–18.
Department of Employment. (1994). Training statistics. London: HMSO.
DiPlacido, J. (1998). Minority stress among lesbians, gay men, and bisexuals: A consequence of heterosexism, homophobia, and stigmatization. In G. Herek (Ed.), Stigma and sexual orientation: Understanding prejudice against lesbians, gay men, and bisexuals (Psychological Perspectives on Lesbian and Gay Issues) (Vol. 4, pp. 138–159). Thousand Oaks, CA: Sage Publications.
Duncan, C., & Loretto, W. (2004). Never the right age: Gender and age-based discrimination in employment. Gender, Work and Organization, 11(1), 95–115.
Dunne, G. A. (1997). Lesbian lifestyles: Women’s work and the politics of sexuality. Toronto, ON: University of Toronto Press.
Eaton, W. W., Anthony, J. C., Mandel, W., & Garrison, R. (1990). Occupations and the prevalence of major depressive disorder. Journal of Occupational Medicine, 32, 1079–1087.
Egan, M., Bambra, C., Thomas, S., Petticrew, M., Whitehead, M., & Thomson, H. (2007). The psychosocial and health effects of workplace reorganisation. 1. A systematic review of organisational-level interventions that aim to increase employee control. Journal of Epidemiology and Community Health, 61(11), 945–954.
Emerson, E., & Hatton, C. (2007). Mental health of children and adolescents with intellectual disabilities in Britain. British Journal of Psychiatry, 191, 493–499.
Evandrou, M., & Glaser, K. (2004). Family, work and quality of life. Ageing and Society, 24, 771–791.
Evanoff, B. A., Bohr, P. C., & Wolf, L. D. (1999). Effects of a participatory ergonomics team among hospital orderlies. American Journal of Industrial Medicine, 35, 358–365.
Fitzgerald, L. F., Magley, V. J., Drasgow, F., & Waldo, C. R. (1999). Measuring sexual harassment in the military: The sexual experiences questionnaire (SEQ-DoD). Military Psychology, 11, 243–263.
Fryers, T., Melzer, D., & Jenkins, R. (2003). Social inequalities and the common mental disorders: A systematic review of the evidence. Social Psychiatry and Psychiatric Epidemiology, 35(5), 229–237.
Gardell, B., & Gustavsen, B. (1980). Work environment research and social change: Current developments in Scandinavia. Journal of Occupational Behavior, 1, 3–17.
Gerber, P. J., & Price, L. A. (2003). Persons with learning disabilities in the workplace: What we know so far in the Americans with Disabilities Act era. Learning Disabilities Research and Practice, 18, 132–136.
Gray, P. (2000). Mental health in the workplace: Tackling the effects of stress. London: The Mental Health Foundation.
Greene, B. (1994). Lesbian and gay sexual orientations: Implications for clinical training, practice, and research. In B. Greene & G. M. Herek (Eds.), Lesbian and gay psychology: Theory, research, and clinical applications (pp. 1–24). Thousand Oaks, CA: Sage Publications.
Gutek, B. A., Cohen, A. G., & Tsui, A. (1996). Reactions to perceived sex discrimination. Human Relations, 49(6), 791–813.
Harnois, G., & Bagriel, P. (2000). Mental health and work: Impact, issues and good practices. Geneva: World Health Organization and International Labour Organization.
Haslam, C., Atkinson, S., Brown, S., & Haslam, R. (2005). Anxiety and depression in the workplace: Effects on the individual and organisation. Journal of Affective Disorders, 88(2), 209–215.
Hassell, B. L., & Perrewe, P. L. (1993). An examination of the relationship between older workers’ perceptions of age discrimination and employee psychological states. Journal of Managerial Issues, 5(1), 109–120.
Henderson, M., Hotopf, M., & Leon, D. A. (2009). Childhood temperament and long-term sickness absence in adult life. British Journal of Psychiatry, 194(3), 220–223.
Hensing, G., Andersson, L., & Brage, S. (2006). Increase in sickness absence with psychiatric diagnosis in Norway: A general population-based epidemiologic study of age, gender and regional distribution. BMC Medicine, 22(4), 19.
Herek, G. M., & Glunt, E. K. (1993). Interpersonal contact and heterosexuals attitudes toward gay men: Results from a national survey. The Social Sex Research, 30(3), 239–244.
Hughes, D., & Dodge, M. A. (1997). African American women in the workplace: Relationships between job conditions, racial bias at work and perceived job quality. American Journal of Community Psychology, 25, 581–599.
Hughes, C., & Williams, G. J. (1994). To disclose or not to disclose: That is the question. Transition LINC, 2, 1–6.
Humphrey, J. (1999). Organizing sexualities, organized inequalities: Lesbians and gay men in public service occupations. Gender, Work and Organization, 6(3), 134–351.
Ingram, K. M., & Smith, N. G. (2004). Workplace heterosexism and adjustment among lesbian, gay, and bisexual individuals: The role of unsupportive social interactions. Journal of Counselling Psychology, 51(1), 57–67.
International Labour Organization. (1992). Conditions of work digest: Preventing stress at work. Geneva: ILO.
Johns, G., & Nicholson, N. (1982). The meanings of absence: New strategies for theory and research. Research in Organizational Behavior, 4, 127–172.
Johnson, J. V., & Hall, E. M. (1988). Job strain, work place social support, and cardiovascular disease: A cross-sectional study of a random sample of the Swedish working population. American Journal of Public Health, 78, 1336–1342.
Johnson, J. V., Hall, E. M., & Theorell, T. (1989). Combined effects of job strain and social isolation on cardiovascular disease morbidity and mortality in a random sample of the Swedish male working population. Scandinavian Journal of Work, Environment and Health, 15, 271–279.
Karasek, R., & Theorell, T. (1990). Healthy work: Stress, productivity and the reconstruction of working life. New York, NY: Basic Books.
Kawakami, N., Araki, A., & Kawahima, M. (1997). Effects of work-related stress reduction on depressive symptoms among Japanese blue-collar workers. Scandinavian Journal of Work, Environment and Health, 23, 54–59.
Kivimäki, M., Virtanen, M., Vartia, M., Elovainio, M., Vahtera, J., & Keltikangas-Järvinen, L. (2003). Workplace bullying and the risk of cardiovascular disease and depression. Occupational and Environmental Medicine, 60(10), 779–783.
Kompier, M. (2003). Job design and well-being. In M. J. Schabracq, J. A. M. Winnubst, & C. L. Cooper (Eds.), The handbook of work and health psychology (2nd ed., pp. 429–454). Chichester, UK: Wiley & Sons Ltd.
LaMotagne, A., Keegel, T., Louie, A., Ostry, A., & Landsbergis, P. (2007). A systematic review of the job stress intervention literature 1990–2005. International Journal of Occupational and Environmental Health, 13, 268–280.
Landsberger, H. A. (1958). Hawthorne revisited. Ithaca, NY: Cornell University Press.
Landsbergis, P. A. (2009). Interventions to reduce job stress and improve work organization and worker health. In P. L. Schnall, M. Dobson, & E. Rosskam (Eds.), Unhealthy work: Causes, consequences and cures (pp. 193–209). Amityville, NY: Baywood Publishing.
Landsbergis, P. A., Cahill, J., & Schnall, P. (1999). The impact of “lean” production and related new systems of worker organisation on worker health. Journal of Occupational Health Psychology, 4(2), 108–130.
Levi, L. (2000). Legislation to protect worker CV health in Europe. In P. Schnall, K. Belkic, P. Landsbergis, & D. Baker (Eds.), The workplace and cardiovascular disease (pp. 269–273). Philadelphia, PA: Hanley & Belfus.
Lim, S., & Cortina, L. M. (2005). Interpersonal mistreatment in the workplace: The interface and impact of general incivility and sexual harassment. Journal of Applied Psychology, 90(3), 483–496.
Lindley, R. M. (1996). The school-to-work transition in the United Kingdom. International Labour Review, 135(2), 159–170.
Loretto, W., Duncan, C., & White, P. (2000). Ageism and employment: Controversies, ambiguities and younger people’s perceptions. Ageing and Society, 20(3), 279–302.
Madaus, J. W. (2008). Employment self-disclosure rates and rationales of university graduates with learning disabilities. Journal of Learning Disabilities, 41(4), 291–299.
Madaus, J. W., Foley, T. E., McGuire, J. M., & Ruban, L. (2002). Employment self-disclosure of postsecondary graduates with learning disabilities: Rates and rationales. Journal of Learning Disabilities, 35, 364–369.
Marchand, A., Demers, A., & Durand, P. (2005). Do occupation and work conditions really matter? A longitudinal analysis of psychological distress experiences among Canadian workers. Sociology of Health and Illness, 27, 602–627.
Marine, A., Ruotsalainen, J., Serra, C., & Verbeek, J. (2006). Preventing occupational stress in healthcare workers. Cochrane Database System Review, 18(4), CD002892.
Marmot, A. F., Eley, J., Stafford, M., Stansfeld, S. A., Warwick, E., & Marmot, M. G. (2006). Building health: An epidemiological study of “sick building syndrome” in the Whitehall II study. Occupational and Environmental Medicine, 63(4), 283–289.
Marmot, M., Feeney, A., Shipley, M., North, F., & Syme, S. L. (1995). Sickness absence as a measure of health status and functioning: From the UK Whitehall II study. Journal of Epidemiology and Community Health, 49(2), 124–130.
Martin, A., Sanderson, K., & Cocker, F. (2009). Meta-analysis of the effects of health promotion intervention in the workplace on depression and anxiety symptoms. Scandinavian Journal of Work and Environmental Health, 35(1), 7–18.
Mayo, E. (1949). Hawthorne and the Western Electric Company: The social problems of an industrial civilisation. London: Routledge.
Mays, V. M., & Cochran, S. D. (2001). Mental health correlates of perceived discrimination among lesbian, gay, and bisexual adults in the United States. American Journal of Public Health, 91(11), 1869–1876.
Mays, V. M., Coleman, L. M., & Jackson, J. S. (1996). Perceived race-based discrimination, employment status and job stress in a national sample of Black women: Implications for health outcomes. Journal of Occupational Health Psychology, 1, 319–329.
McDermott, E. (2006). Surviving in dangerous places: Lesbian identity performances in the workplace, social class and psychological health. Feminism and Psychology, 16(2), 193–211.
McGregor, J., & Gray, L. (2001). The mature job seeker. Palmerston North, New Zealand: Massey University.
McKenzie, K. (2003). Racism and health. British Medical Journal, 326, 65–66.
Miller, G. V. F., & Travers, C. J. (2005). Ethnicity and the experience of work: Job stress and satisfaction of minority ethnic teachers in the UK. International Review of Psychiatry, 17, 317–327.
Morrow, P. C., McElroy, J. C., & Phillips, C. M. (1994). Sexual harassment behaviors and work related perceptions and attitudes. Journal of Vocational Behavior, 45, 295–309.
Murray, L. R. (2003). Sick and tired of being sick and tired: Scientific evidence, methods, and research implications for racial and ethnic disparities in occupational health. American Journal of Public Health, 93, 221–226.
Nawyn, S. J., Richman, J. A., Rospenda, K. M., & Tonda, L. H. (2000). Sexual identity and alcohol-related outcomes: Contributions of workplace harassment. Journal of Substance Abuse, 11(3), 289–304.
Nazroo, J. Y. (1997). Ethnicity and mental health: Findings from a National Community Survey. London: Policy Studies Institute.
Nazroo, J. Y. (2003). The structuring of ethnic inequalities in health: Economic position, racial discrimination and racism. American Journal of Public Health, 93, 277–284.
Nordenmark, M. (2002). Multiple social roles—Resource or a burden: Is it possible for men and women to combine paid work with family life in a satisfactory way? Gender, Work and Organization, 9(2), 125–145.
Norris, W. P. (1991). Liberal attitudes and homophobic acts: The paradoxes of homosexual experience in a liberal institution. Journal of Homosexuality, 22, 81–120.
O’Campo, P., Eaton, W., & Muntaner, C. (2004). Labor market experience, work organization, gender inequalities and health status: Results from a prospective analysis of U.S. employed women. Social Science and Medicine, 58(2), 585–594.
Palmer, A. (1993). Some are more equal than others. London: Stonewall.
Palmore, E. (1990). Ageism: Negative or positive? New York, NY: Springer.
Park, K. O., Schaffer, B. S., & Griffin-Blake, C. S. (2004). Effectiveness of a healthy work organization intervention: Ethnic group differences. Journal of Occupational and Environmental Medicine, 46, 623–634.
Parker, S. K., Chmiel, N., & Wall, T. D. (1997). Work characteristics and employee well‐being within a context of strategic downsizing. Journal of Occupational Health Psychology, 2(4), 289–303.
Parker, S. K., Jackson, P. R., Sprigg, C. A., & Whybrow, A. C. (1998). Organisational interventions to reduce the impact of poor work design. Sheffield: University of Sheffield/Health & Safety Executive.
Parkes, K. R., & Sparkes, T. J. (1998). Organisational interventions to reduce work stress: Are they effective? A review of the literature. Sudbury, ON: HSE Books.
Parks, K. M., & Steelman, L. A. (2008). Organizational wellness programs: A meta-analysis. Journal of Occupational Health Psychology, 13(1), 58–68.
Poulsen, K., Jensen, S., Bach, E., & Schostak, J. (2007). Using action research to improve health and the work environment for 3500 municipal bus drivers. Educational Action Research, 15(1), 75–106.
Ragins, B. R., & Scandura, T. A. (1995). Antecedents and work-related correlates of sexual harassment: An empirical investigation of competing hypotheses. Sex Roles, 32, 429–455.
Raver, C. C. (2003). Does work pay psychologically as well as economically? The role of employment in predicting depressive symptoms and parenting among low-income families. Child Development, 74(6), 1720–1736.
Raw, G. J., Roys, M. S., & Leaman, A. (1993, August). Sick building syndrome, productivity and control. Property Journal, 17–19.
Romeri, E., Baker, A., & Griffiths, C. (2007). Alcohol-related deaths by occupation, England and Wales, 2001–5, Office for National Statistics. Health Statistics Quarterly, 35. Retrieved from http://www.statistics.gov.uk/downloads/theme_health/HSQ35.pdf
Rosenheck, R., Leslie, D., Keefe, R., McEvoy, J., Swartz, M., & Perkins, D. (2006). Barriers to employment for people with schizophrenia. American Journal of Psychiatry, 163, 411–417.
Rospenda, K. M., & Richman, J. A. (2005). Harassment and discrimination. In J. Barling, E. K. Kelloway, & M. R. Frone (Eds.), Handbook of work stress (pp. 149–188). Thousand Oaks, CA: Sage.
Rospenda, K. M., Richman, J. A., & Shannon, C. A. (2009). Prevalence and mental health correlates of harassment and discrimination in the workplace: Results from a national study. Journal of Interpersonal Violence, 24(5), 819–843.
Rospenda, K. M., Richman, J. A., Wislar, J. S., & Flaherty, J. A. (2000). Chronicity of sexual harassment and generalized work-place abuse: Effects on drinking outcomes. Addiction, 95, 1805–1820.
Rugulies, R., Bültmann, U., Aust, B., & Burr, H. (2006). Psychosocial work environment and incidence of severe depressive symptoms: Prospective findings from a 5-year follow-up of the Danish work environment cohort study. American Journal of Epidemiology, 163(10), 877–887.
Saks, A., & Waldman, D. (1998). The relationship between age and job performance evaluations for entry-level professionals. Journal of Organizational Behavior, 19(4), 409–419.
Sanderson, K., & Andrews, G. (2006). Common mental disorders in the workforce: Recent findings from descriptive and social epidemiology. Canadian Journal of Psychiatry, 51(2), 63–75.
Sargeant, M. (2001). Lifelong learning and age discrimination in employment. Education and the Law, 13(2), 141–154.
Saunders, T., Driskell, J. E., Johnston, J. H., & Salas, E. (1996). The effect of stress inoculation training on anxiety and performance. Journal of Occupational Health and Psychology, 1(2), 170–186.
Schnall, P. L., Pieper, C., Schwartz, J. E., Karasek, R. A., Schlussel, Y., Devereux, R. B., et al. (1990). The relationship between “job strain”, workplace diastolic blood pressure, and left ventricular mass index: Results of a case-control study. JAMA, 263(14), 1929–1935.
Schulze, B., & Angermeyer, M. C. (2003). Subjective experiences of stigma: A focus group study of schizophrenia patients, their relatives and mental health professionals. Social Science & Medicine, 56, 299–312.
Schuman, E., & Kleiner, B. (2001). Is age a handicap in finding employment? Equal Opportunities International, 20(5–7), 48–52.
Semmer, N. (2006). Job stress interventions and the organisation of work. Scandinavian Journal of Work, Environment and Health, 32(6), 515–527.
Siegrist, J., Peter, R., & Junge, A. (1990). Low status control, high effort at work and ischemic heart disease: Prospective evidence from blue collar men. Social Science and Medicine, 31, 1127–1134.
Skidmore, P. (2004). A legal perspective on sexuality and organization: A lesbian and gay case study. Gender, Work and Organization, 11(3), 229–253.
Smiley, E. (2005). Epidemiology of mental health problems in adults with learning disability: An update. Advances in Psychiatric Treatment, 11, 214–222.
Smith, A., Johal, S., Wadsworth, E., Davey, S. G., & Peters, T. (2000). The scale and impact of occupational stress: The Bristol Stress and Health at Work Study. London: Health & Safety Executive Research Report No. 265.
Snape, E., & Redman, T. (2003). Too old or too young? The impact of perceived age discrimination. Human Resource Management Journal, 13(1), 78–89.
Sorensen, L., & Roberts, S. J. (1997). Lesbian uses of and satisfaction with mental health services: Results from Boston Lesbian Health Project. Journal of Homosexuality, 33(1), 35–49.
Sorensen, G., Stoddard, A., Ockene, J. K., Hunt, M. K., & Youngstrom, R. (1996). Worker participation in an integrated health promotion/health protection program: Results from the WellWorks Project. Health Education Quarterly, 23, 191–203.
Stansfeld, S. A., North, F. M., White, I., & Marmot, M. G. (1995). Work characteristics and psychiatric disorder in civil servants in London. Journal of Epidemiology and Community Health, 49(1), 48–53.
Stansfeld, S. A., Bosma, H., Hemingway, H., & Marmot, M. G. (1998). Psychosocial work characteristics and social support as predictors of SF-36 health functioning: The Whitehall II study. Psychosomatic Medicine, 60, 247–255.
Stansfeld, S. A., & Candy, B. (2006). Psychosocial work environment and mental health: A meta-analytic review. Scandinavian Journal of Work and Environmental Health, 36(6), 443–462.
Stansfeld, S. A., Clark, C., Caldwell, T., Rodgers, B., & Power, C. (2008). Psychosocial work characteristics and anxiety and depressive disorders in midlife: The effects of prior psychological distress. Occupational and Environmental Medicine, 65(9), 634–642.
Stansfeld, S. A., Rasul, F. R., Head, J., & Singleton, N. (2011). Occupation and mental health in a national UK survey. Social Psychiatry and Psychiatric Epidemiology, 46(2), 101–110.
Stansfeld, S. A., Woodley Jones, D., Rasul, F., Head, J., Clarke, S., & Mackay, C. (2008). Work related distress in the 1990s: A real increase in ill health? Journal of Public Mental Health, 7, 26–31.
Stuart, H. (2004). Stigma and work. Healthcare Papers, 5, 100–111.
Stuart, H. (2006). Mental illness and employment discrimination. Current Opinion in Psychiatry, 19(5), 522–526.
Tucker, P., & Knowles, S. R. (2008). Review of studies that have used the Standard Shiftwork Index: Evidence for the underlying model of shiftwork and health. Applied Ergonomics, 39(5), 550–564.
van der Klink, J. J., Blonk, R. W., Schene, A. H., & van Dijk, F. J. (2001). The benefits of interventions for work-related stress. American Journal of Public Health, 91, 270–276.
van Vegchel, N., de Jonge, J., Bosma, H., & Schaufeli, W. (2005). Reviewing the effort-reward imbalance model: Drawing up the balance of 45 empirical studies. Social Science and Medicine, 60(5), 1117–1131.
Velligan, D. I., & Gonzalez, J. M. (2007). Rehabilitation and recovery in schizophrenia. Psychiatric Clinics of North America, 30(3), 535–548.
Virtanen, M., Pentti, J., Vahtera, J., Ferrie, J. E., Stansfeld, S. A., Helenius, H., et al. (2008). Overcrowding in hospital wards as a predictor of antidepressant treatment among hospital staff. American Journal of Psychiatry, 165(11), 1482–1486.
Wadsworth, E., Dhillon, K., Shaw, C., Bhui, K., Stansfeld, S., & Smith, A. (2007). Racial discrimination, ethnicity and work stress. Occupational Medicine (London), 57(1), 18–24.
Walker, A. (2005). Towards and international political economy of ageing. Ageing and Society, 25, 815–839.
Wieclaw, J., Agerbo, E., Mortensen, P. B., & Bonde, J. P. (2006). Risk of affective and stress related disorders among employees in human service professions. Occupational and Environmental Medicine, 63(5), 314–519.
Wieclaw, J., Agerbo, E., Mortensen, P. B., Burr, H., Tuchsen, F., & Bonde, J. P. (2008). Psychosocial working conditions and the risk of depression and anxiety disorders in the Danish workforce. BMC Public Health, 7(8), 280.
Wing, J. K. (1970). Unemployment among chronic psychotic patients in Camberwell: Their need for rehabilitation. Proceedings of the Royal Society of Medicine, 63(12), 1329–1332.
Wood, G., Wilkinson, A., & Harcourt, M. (2008). Age discrimination and working life: Perspectives and contestations—A review of the contemporary literature. International Journal of Management Reviews, 10(4), 425–442.
Woods, J. D. (1993). The corporate closet: The professional lives of gay men in America. New York, NY: The Free Press.
Ybema, J. F., & van den Bos, K. (2010). Effects of organizational justice on depressive symptoms and sickness absence: A longitudinal perspective. Social Science and Medicine, 70(10), 1609–1617.
Ylipaavalniemi, J., Kivimäki, M., Elovainio, M., Virtanen, M., Keltikangas-Järvinen, L., & Vahtera, J. (2005). Psychosocial work characteristics and incidence of newly diagnosed depression: A prospective cohort study of three different models. Social Science and Medicine, 61(1), 111–122.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Stansfeld, S., Dinos, S., Raffel, J. (2014). Environmental Influences: The Workplace and Mental Health—Models, Vulnerability Factors, and Interventions. In: Sloboda, Z., Petras, H. (eds) Defining Prevention Science. Advances in Prevention Science. Springer, Boston, MA. https://doi.org/10.1007/978-1-4899-7424-2_10
Download citation
DOI: https://doi.org/10.1007/978-1-4899-7424-2_10
Published:
Publisher Name: Springer, Boston, MA
Print ISBN: 978-1-4899-7423-5
Online ISBN: 978-1-4899-7424-2
eBook Packages: MedicineMedicine (R0)