
Abstract
Peritoneal surface malignancy (PSM) is a heterogeneous form of cancer. A paradigm shift has occurred in the past 50 years; operative intervention in selected patients with limited peritoneal carcinomatosis (PC) is now undertaken with curative intent. Approximately 150,000 patients are diagnosed with colorectal cancer (CRC) in 2012 in the USA and one third die from the disease each year. Approximately 8,000 patients in the USA are diagnosed with synchronous PSM; 8 % with CRC have synchronous peritoneal spread of disease at time of primary resection, and up to 25 % of patients with recurrent CRC have disease confined to the peritoneal cavity. In about 30 %, PSM is the main reason for death in CRC patients, and only ~50 % of patients who develop PSM from CRC may have curative treatment by an R0 resection. The multimodal treatment approach for carefully selected patients with good performance status and limited PC consists of cytoreductive surgery (CRS), followed by hyperthermic intraperitoneal chemotherapy (HIPEC). This treatment approach represents a formidable challenge for patients and surgeons alike, as well as members of the multidisciplinary health-care team. In patients undergoing CRS + HIPEC technique not the only aim; a much broader, holistic view of care is imperative. Such an approach is emphasized in this chapter.
Contributing Author Declaration
We certify that all individuals who qualify as authors have been listed; each author has participated in one or more of the following areas: conception and design of this work, the acquisition and/or analysis of data, the writing and/or critical revision of the document, and supervision of this cooperative research effort. All contributing authors approve of the submission of this version of the manuscript and assert that the document represents valid work. If information derived from another source was used in this manuscript, we obtained all necessary approvals to use it and made appropriate acknowledgements in the document. All contributing authors take public responsibility for this work.
Copyright Protection
One of the contributing authors are military service members (or employees of the US Government: AS), and this work was prepared as part of their official duties. Title 17 U.S.C. 105 provides the “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a US Government work as a work prepared by a military service member or employee of the US Government as part of that person’s official duties.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Peritoneal Carcinomatosis
- Cytoreductive Surgery
- Intraperitoneal Chemotherapy
- Peritoneal Surface
- Peritoneal Cancer Index
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
FormalPara Key Points-
Tumor biology is an extremely important, yet difficult to quantify, factor for overall outcomes.
-
Proper patient selection is the key to cytoreductive surgery and HIPEC.
-
Understand not only good candidates but also patients with contraindications based on preoperative staging, as they will not derive any benefit.
-
Select patients with peritoneal surface malignancy can be cured.
-
Cytoreductive surgery and HIPEC is challenging and has the potential for increased morbidity.
-
A multimodality approach includes lifelong surveillance and the potential for repeated treatments.
Background, Basics, and Rationale
General Aspects, Epidemiology
Key Concept: Cytoreductive surgery and heated intraperitoneal chemotherapy prolongs survival in carefully selected patients in whom complete resection of all grossly apparent disease can be attained (completeness of cytoreduction score 0/1).
It remains controversial if patients suffering from PSM of CRC origin should be treated by a time-, labor-, and cost-intensive multimodal interdisciplinary therapeutic approach using CRS + HIPEC, or if palliative treatment remains the standard of practice. In this chapter, we try to provide a broad overview of the multifaceted considerations in order to provide a critical assessment of this controversial matter and provide guiding principles as to how best to implement such an approach.
As people worldwide grow older, common afflictions increase in incidence—coronary heart diseases, diabetes mellitus, dementia, and cancer. One of every four deaths in the USA is due to cancer [1], and cancer is the leading cause of death among Hispanics in the USA [2]. A total of 1,638,910 new cancer cases and 577,190 deaths from cancer were projected to occur in the USA in 2012 alone [1]. Of these, ~150,000 patients are diagnosed with CRC and nearly 50,000 die from this disease each year [1]. More pertinent to the present discussion, approximately 8,000 patients in the USA are diagnosed with synchronous PSM of colorectal cancer origin annually [3, 4]. An overview of disease-specific consideration in PSM is shown in Table 5.1.
Peritoneal surface malignancy of CRC origin is a frequent manifestation in the natural history of the disease, and it is associated with marked deterioration in quality of life (QOL) and very poor prognosis. Peritoneal disease spread continues to be a common mode of disease progression for intra-abdominal malignancies. Eight percent of patients with CRC have synchronous peritoneal spread of disease at time of primary resection, and up to 25 % of patients with recurrent CRC have disease confined to the peritoneal cavity [3]. In about 30 % of patients with CRC, PSM is the main reason for disease-specific mortality [9]. On the positive side, ~50 % of patients who develop PSM from CRC may have curative treatment by an R0-resection.
Confinement of disease to a limited extent of the peritoneal surface in the absence of systemic spread of disease has served as the basis for surgical eradication of disease through aggressive CRS + HIPEC. Survival during the time when patients with PSM from CRC had been treated by systemic therapy alone, typically 5-FU, was limited to approximately 6 months (range 5–7 months) [9, 10]. Among patients who suffered from PSM due to CRC and had simultaneous malignant bowel obstruction, the survival was even worse—limited to 3 months [11]. Based on recent experience, however, a paradigm shift has occurred.
Change of Paradigm
Key Concept: The results that can be obtained with cytoreduction and heated intraperitoneal chemotherapy for resectable peritoneal surface malignancy of colorectal cancer origin are similar to hepatic resection for resectable colorectal cancer metastasis, with 5-year overall survival of ~45 %.
A clear change of paradigm occurred slowly within the past 50 years, in part due to the increasing recognition that PSM is a regional disease once limited to a compartment—the abdomen. It was not, as once thought, a systemic disease for which only palliative intervention was indicated [3]. It was not until the 1980s that the generally held fatalistic view of PC gave way to a new way of thinking with regard to treatment options and treatment-specific prognosis; such options expanded beyond purely palliative and/or best supportive therapy. During the 1990s, pioneering surgeons such as Paul Sugarbaker and Francois Gilly were the principal driving forces that moved away from that fatalistic approach toward a curative treatment approach by using CRC + HIPEC in carefully selected patients that could benefit from such an aggressive treatment intervention [3, 4, 12–16]. Disease once limited to bleak outcomes of 3–6 month median survival with therapy could, in selected cases, be treated aggressively with CRS + HIPEC and have strikingly improved outcomes [9, 10]. In fact, patients undergoing complete resection of PSM from CRC followed by HIPEC could attain median survival of 21–40 months, while patients with pseudomyxoma peritonei were reported to have 20-year survival of up to 70 % [17]. However, these results clearly depended on the extent of peritoneal surface tumor burden and completeness of cytoreduction [18]. The curative treatment approach in PC is a demanding and complex interdisciplinary procedure in which surgeons, anesthetists, oncologists, gastroenterologists, dieticians, physical and occupational therapists, psychologists, and case managers, among others, should be equally involved in the patient-centered, integrative, team approach to cancer care. It must be emphasized that CRS, HIPEC, and systemic therapy are not competitive therapies, and this can be recognized by the fact that in France this therapeutic paradigm has already incorporated into French Guidelines for standards of practice [19]. In 2012, Germany integrated this approach into national treatment guidelines as a therapeutic option [20]. Surgical oncologists caring for patients with PC need a wide range of training and experience that extends well beyond the technical aspects of surgical care and includes understanding of the biology of disease, assessment of the extent of disease, careful patient selection, administration of HIPEC, and related anesthetic and safety considerations, as well as postoperative interventions for secondary surgical events. Understanding of the fundamentals of peritoneal surface disease-specific anatomy and embryology is essential.
Anatomy and Embryology
Key Concept: The pelvic–peritoneal partition serves as the anatomic basis for the delivery of dose-dense heated intraperitoneal chemotherapy.
A detailed description of the ultrastructure of the peritoneum was published by Baron in 1941 [21] and reviewed recently by us [20]. The distinct histological structure of the peritoneum is evident in a special type of vascular anatomy and also its specific function. The peritoneum consists of a single-cell layer of mesothelial cells, with a basal membrane beneath it along with five layers of connective tissue (interstitial cells and a matrix of collagen, hyaline, and proteoglycans), with a total thickness of 90 μm [3, 22]. As it also contains other cellular elements such as pericytes, parenchymal cells, and blood capillary vessels, the peritoneum is often referred to as the “peritoneal membrane.” The functions of the peritoneum include maintenance of the mobility of intra-abdominal organs relative to the abdominal wall. This is achieved through a lubricant secreted by the peritoneal membrane consisting of glycosaminoglycans and phospholipids. The membrane further fulfills an important function in defense against intra-abdominal infections. It is also thought that the peritoneum represents the principal barrier and initial line of defense against dissemination of malignant cells and establishment of peritoneal carcinomatosis [23]. This view is supported by research, which has shown that intraperitoneal injection of aggressive tumor cell lines leads to a corresponding increase in tumor cell activity in the peritoneal membrane [3]. The interaction between its single layer of mesothelial cells together with associated blood capillaries and surrounding interstitial matrix contributes to this line of defense [24]. In fact, the peritoneal membrane is regarded as an organ itself [3] and its surface area approximates 7,500 cm2 and is in direct contact with all intra-abdominal organs.
At the end of the third week of gestation, the intraembryonic mesoderm divides bilaterally into the mesoderm, the intermediate mesoderm, and the lateral plate. In the lateral plate, a mesothelial cell layer divides into the parietal and visceral mesoderm. The parietal mesoderm, which lines the intraembryonic celomic cavity, becomes the parietal peritoneum, the parietal pleura, and the pericardium. From the visceral mesodermal layer, the visceral peritoneum, visceral pleura, and epicardium develop. The dorsal mesentery, to which the intestinal tube is attached, represents the junction between the parietal and visceral peritoneum. Understanding this embryology and anatomical relationship is important in the technical execution of cytoreduction [3]. It is also important to recognize that there is practically never any tumor penetration into the underlying organ structures (e.g., kidney, spleen) in cases of PC. This is probably due to the peritoneum’s embryologically delineated barrier function.
Classification and Types of Growth of PC
Key Concept: Irrespective of the growth pattern of peritoneal surface malignancy, the predominant factor-determining outcome is the ability to achieve complete cytoreduction.
Peritoneal surface malignancy can be subdivided into primary and secondary forms [3]. Primary PSM consists of invasion by a mesothelioma or pseudomyxoma peritonei—both extremely rare tumor entities. Secondary PC originates most commonly from gastrointestinal tumors [25–27] or urogenital tumors [28]. Other forms of secondary PC involve less common primary epithelial malignancies such as malignant melanoma or breast carcinoma. There are important differences between growth types in peritoneal carcinomatosis pertaining to involvement of the bowel, supporting mesentery, and its critical vascular structures; these are important to consider when estimating likelihood of achieving complete cytoreduction with CRS, particularly when there is substantial involvement of the mesenteric pedicle, or root of the mesentery (Fig. 5.1), [3].




(a–e) Growth patterns in peritoneal carcinomatosis on the small bowel (Modified from Brücher et al. [3])
History and Rationale for Intraperitoneal Drug Therapy
Key Concept: Heated intraperitoneal chemotherapy is indicated for treatment of non-visible or <1 mm peritoneal surface tumor deposits.
The history of intraperitoneal drug therapy was reported recently [20]. The earliest report mentioned in the literature about the use of intraperitoneal “drug therapy” was by the English surgeon, Christopher Warrick in 1744 [29]. The Belgium surgeon, WP Ceelen, together with a US colleague, MF Flessner, reported on the biophysics of intraperitoneal therapy [30] that Warrick injected into the peritoneal cavity, a mixture of “Bristol” water and “claret,” a Bordeaux wine, in the female, Jane Roman, who suffered from malignant ascites. The cytotoxic nitrogen mustard, which had been in use during World War II, was investigated in the 1950s in clinical trials for the purpose of intraperitoneal therapy [31]. In 1978, Dedrick reported about the pharmacokinetics of intraperitoneal drug delivery, distribution, and clearance given the peritoneal–plasma partition. This anatomical barrier provides the fundamental rationale for intraperitoneal drug delivery, such that a much higher drug concentration can be used than administered systemically, because peritoneal drug clearance is much slower than plasma clearance [32]. Intraperitoneal drug delivery has been proven to be efficient and effective in patients with minimal (“infra-millimetric”) or microscopic residual disease following cytoreductive surgery [30]. Hence, cytoreductive surgery is intended to clear visible peritoneal surface disease, while HIPEC is indicated for treatment of non-visible or <1 mm peritoneal tumor deposits, as intraperitoneal chemotherapy penetrates only a millimeter in depth during HIPEC. The reason why intraperitoneal therapy emerged early in the history of regional therapy seems to be related to the challenge of alleviating symptomatic malignant ascites. There are various epithelial malignancies that may lead to symptomatic ascites; these are shown in Fig. 5.2 [33]. Malignant ascites reflects a symptom of peritoneal carcinomatosis, and it indicates the presence of malignant cells within the peritoneal cavity. The biodynamic effects of intraperitoneal drug administration were shown to be dependent on a number of key variables, such as diffusion and convection (dependent on molecular weight of the agent administered), and interstitial fluid pressure; malignant tumors characteristically have elevated interstitial fluid pressure, which serves as a barrier for connective drug transport. Flessner et al. showed that the structure of the peritoneal intracellular matrix is the major source of resistance to macromolecular drug transport [34]. The tumor penetration distance measured experimentally ranges from a few cell layers (generally <1 mm) to a maximum of 3–5 mm [30]. Active and passive transport across the cell membrane leads to better and somewhat worse intracellular drug concentration, and the mode of transport influences the efficacy of regional drug application. Additionally, in the case of cisplatin, the copper transport protein-1(CTR1) regulates uptake in human cancer cells [35]. Additionally, preclinical models have shown that hypotonic carrier fluids lower interstitial fluid pressure and increase intraperitoneal pressure, leading to enhanced peritoneal drug penetration [30].


Primary etiology of malignant ascites (Modified from: Avantunde and Parson [33])
Peritoneal Cancer Index (PCI)
Key Concept: A key quantitative prognostic index is the peritoneal cancer index (PCI). Cytoreductive surgery should not be undertaken with curative in patients with PCI ≥20, as the results of CRS + HIPEC are not different than systemic therapy alone.
Presurgical extent of disease evaluation should provide reliable information about the tumor location, the extent of peritoneal tumor burden, and distribution and extent of the disease so that diligent patient selection can be carried out [3]. Studies on the preoperative clinical staging of PC have shown that the reliability of computed tomography (CT) for predicting the stage of the disease is somewhat limited [36]. As reviewed earlier [3], various scoring systems are currently in use for the assessment of peritoneal surface disease burden:
-
Sugarbaker’s peritoneal cancer index (PCI) [37] (Fig. 5.3)
Fig. 5.3 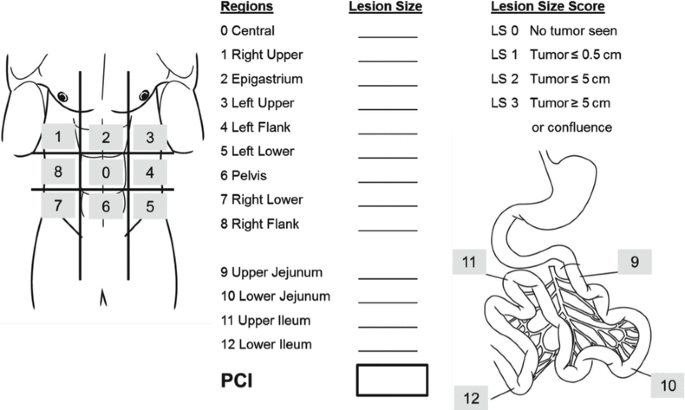
The peritoneal cancer index (PCI) (Modified from: modified according Jacquet and Sugarbaker [37])
-
Verwaal’s N score [38]
-
Gilly’s classification [16]
-
P score [39]


The PCI [37] is well established, currently in use at the major PSM centers worldwide (Fig. 5.3), and was confirmed as the preferred scoring system by a consensus conference held in Milan in 2006 [40]. Sugarbaker divides the abdominal compartment into nine regions (Regions 0 through 9), and the small bowel separately into four regions (Regions 10 through 13). After exploring the abdomen, all single regions are assigned a score corresponding to the greatest possible extent of tumor involvement by size of the largest peritoneal surface lesion within that region (lesion size from 0, no tumor seen, to 3, tumor >5 cm). Out of this, the maximum possible number of points in the PCI is thus 39, and the lowest is 0. Sugarbaker’s analyses revealed that patients with a PCI score of less than 20 have a reasonable likelihood of complete cytoreduction, thereby prognosis (in comparison with the previous approach of palliative chemotherapy alone and/or best supportive care) that may be favorably impacted by CRS + HIPEC. A challenge for the future will be reliable pre-therapeutic (before surgical exploration) prediction of tumor involvement of the small bowel and/or mesentery, as this represents one of the major limiting factors for the ability to achieve complete cytoreduction with CRS. The Society of Surgical Oncology has published surgical selection criteria for patients with PSM in 2006 [40].
Residual Tumor Classification (Completeness of Cytoreduction, CC Score)
Key Concept: Another key prognostic indicator is completeness of cytoreduction (CC) score. The goal is to attain complete removal of all grossly evident disease (CC0) or to leave behind only a few minute deposits of peritoneal surface tumor that can be treated effectively with HIPEC (CC1). Therefore, complete CRS implies both CC0 and CC1. The only way in which the patient can achieve long-term benefit is through having complete cytoreduction (CC0/1).
The major basis for prognosis in surgical oncology is completeness of resection, obtaining complete clearance of grossly apparent disease. This is usually determined by the R-classification (residual tumor classification). CRS is also based on the target criteria used in surgical oncology—achieving complete macroscopic and microscopic freedom from tumor (R0 resection). It is difficult to communicate in terms of R0 resection after multivisceral resection in the context of CRS. Therefore, the classification of “completeness of cytoreduction,” so-called CC classification [41], was developed and also affirmed at the 2006 consensus conference in Milan (Table 5.2) [40]. In patients with mucinous pseudomyxoma peritonei who undergo CRS + HIPEC, the R0 resection referred to elsewhere in the gastrointestinal tract is equivalent to CC 0 (no residual tumor) and CC1 status (<0.25 cm residual tumor tissue),whereas in invasive gastrointestinal tumors such as CRC and/or gastric carcinomas, R0 resection is only equivalent to CC 0 status. Completeness of resection is of paramount importance for patients with PC, and it has been clearly shown that patients with CC 0/CC 1 resections have a significantly improved survival period than those who do not [41–44]. In fact, there is no indication for CRS/HIPEC treatment in the setting of incomplete cytoreduction (CC2/3). Therefore, the CC classification is important not only in patient selection for CRS (only those in whom CC 0/1 status can be achieved should undergo attempted CRS) but also in estimating oncological outcome of CRS for a given CC score, which has been shown to be of significant prognostic value, serving as a surrogate marker for disease-free and overall survival after CRS for patients with PSM due to CRC [45, 46].
HIPEC: Technique, Rationale, and Drugs
Key Concept: The strategic rationale for HIPEC includes increased chemotherapeutic agent concentration/dose at the intended site of action, increased cytotoxic effect of the administered intraperitoneal agent, reduced systemic absorption and toxicity of the chemotherapeutic, homogeneous distribution of intraperitoneal chemotherapy, and direct antitumor effect of hyperthermia.
Hyperthermic intraperitoneal chemotherapy (HIPEC) can be carried out as an open (“coliseum”) or closed procedure [3]. The coliseum technique allows manual distribution of the perfusate during HIPEC that is extremely important for certain anatomical regions. The principle is that the abdomen is initially filled with a carrier solution (dialysis or Ringer’s solution). The carrier solution is then passed through the HIPEC machine to heat it. Once a steady-state temperature of minimum of 42 °C has been reached (optimally a mean temperature of 43–44 °C), the chemotherapeutic agent is added and HIPEC starts. The intra-abdominal temperature is measured every minute, and patient-specific temperatures (bladder, head, esophageal, and/or rectal temperature probe temperature assessed by the anesthetist) are also closely monitored and recorded. After 30–90 min of HIPEC, the carrier solution is drained along with the chemotherapeutic agent, and the abdomen is lavaged with approximately 8–10 L of Ringer’s solution. Both the perfusate and lavage solutions must be disposed of as potentially hazardous waste material. Locoregional (intraperitoneal) administration of chemotherapy increases the local concentration of the chemotherapeutic agent at the site of action, the peritoneal surface. This reduces the systemic toxicity of the treatment, but at the expense of potentially increased postoperative morbidity related to the surgical procedure [47]. Some institutions create the anastomosis before and some after the administration of HIPEC. One animal study showed that anastomotic insufficiency is more likely to occur when systemic 5-fluorouracil (5-FU) treatment is carried out around the time of HIPEC than when locoregional chemotherapy is used alone [48]. Another study in a rat model showed that HIPEC consistently resulted in delayed healing of colonic anastomosis [49], raising the question whether technical modifications (e.g., proximal diversion) are indicated in the setting of HIPEC.
In HIPEC, the carrier solution (dialysis or Ringer’s solution) is initially heated to a temperature of 43 °C, with instillation of the chemotherapeutic agent only being carried out afterwards. The chemotherapeutic agent is circulated in the peritoneal cavity administered for 30–90 min, depending on the preference of the peritoneal carcinomatosis center concerned and the agent being utilized. When HIPEC has been completed at a mean temperature of 43–44 °C, the abdomen may be lavaged. Postoperatively, the patient is monitored in an intensive care unit. It is important to note that cisplatin-containing substances in particular can also have direct cardiotoxic effects. As a result of the large wound surface, it is possible for cis-diaminedichloroplatinum (CDDP) to be washed into the bloodstream, leading to cardiotoxicity, for which care in a monitored setting following operation is imperative.
At present, the agents used in HIPEC are mainly mitomycin C, cisplatin (CDDP), oxaliplatin, and doxorubicin. Intraperitoneal administration of chemotherapeutic agent achieves high response rates in patients with peritoneal carcinomatosis, as the peritoneum–plasma barrier makes it possible to administer high doses of the drug [50]. On the basis of analyses conducted during peritoneal dialysis, Dedrick et al. showed in 1978 that the peritoneal permeability of hydrophilic cancer drugs is lower than the known plasma clearance of the same agents [32]. The chemotherapeutic drugs mitomycin C, cisplatin, and/or oxaliplatin are the agents of choice for HIPEC. These drugs have a relatively high molecular weight (mitomycin C, 334 Da; cisplatin, 300 Da; oxaliplatin, 397 Da). Due to reduced permeability into the plasma through the peritoneal barrier, they consequently have lower systemic concentrations and thus lower associated toxicity [51, 52]. The challenge when interpreting the international literature is that there are also centers in which systemic chemotherapy is administered simultaneously with heated agents delivered into the peritoneal cavity [3]. Another important variable aside from the type (open versus closed technique) and duration (30, 60, 90 min) of HIPEC is the temperature at which the chemotherapy is delivered into the peritoneal cavity (generally >41.5 °C). Hyperthermia above 41 °C alone produces a direct antitumor effect. However, tumor cells react through upregulation of heat shock proteins, which may be able to produce some thermal tolerance [53]. This cytotoxic effect has been demonstrated only for drugs containing platinum [54] and for mitomycin C [55]. It is also important to recognize that hyperthermia itself has deeper tissue effects [56]. The rationale for hyperthermic delivery of intraperitoneal chemotherapy immediately after CRS is summarized in Table 5.3 [3]. Deeper tissue effects of HIPEC are discussed in the following section.
Multimodal Therapy in Peritoneal Carcinomatosis
Key Concept: Multimodality therapy consisting of cytoreductive surgery + HIPEC in patients with CRC peritoneal carcinomatosis is superior over systemic therapy alone.
Published randomized phase III trials in PSM and CRC had been recently reviewed in detail [4]. In this and another recent review addressing the application of the second look operation [20], it was emphasized that systemic multidrug chemotherapy alone has not altered significantly the natural history and/or prognosis of patients with PSM and CRC. First-line 5-fluorouracil-based regimens (5-FU/leucovorin (LV) including oxaliplatin (FOLFOX) and irinotecan (IFL, FOLFIRI) with or without targeted monoclnal antibody therapy using bevacizumab (IFL/bevacizumab) or cetuximab (Erbitux) have increased response rates to a range of 25–55 % and median overall survival rates from 12 to 24 months compared to the benchmark regimen applied as the standard of practice over the past 40 years (5-FU or 5-FU/LV) [57–65]. A retrospective pooled analysis of over 2,000 study subjects enrolled in the North Central Cancer Treatment Group (NCCTG) Phase III Trials N9741 and N9841 demonstrated a median survival of 12.7 months in patients with peritoneal spread of CRC [66]. Treatment-adjusted analysis showed that patients with PSM and CRC have worse survival compared to patients with advanced CRC and distant metastases without PSM (p = 0.0006). Oncological outcome in patients with PSM of CRC origin treated by second line 5-FU + leucovorin + oxaliplatin (FOLFOX) was not significantly improved. Progression-free survival was ~6 months. This is in contradistinction to reported median survival rates between 19 and 63 months in experienced centers using CRS + HIPEC to treat limited PSM of CRC origin (that can be completely resected), underscoring the advantage of this multimodality therapeutic approach [19, 67–69]. Although FOLFOX was found to be superior to irinotecan + 5-FU/leucovorin (IFL) and irinotecan + oxaliplatin (IROX) as first-line therapy in the pooled analysis of the NCCTG trials by Franko et al., no survival benefit was apparent with second line use [66]. Systemic multidrug chemotherapy has not altered the natural history of peritoneal carcinomatosis as patients suffer disease progression and functional deterioration due to visceral obstruction, malignant ascites, and cancer cachexia over a limited median survival [4].
The multimodality therapy approach, using systemic chemotherapy plus aggressive CRS and HIPEC, has shown clearly promising results. The randomized controlled trial (RCT) of Verwaal et al. demonstrated a statistically significant survival advantage for this therapeutic approach [67, 68]. This was an RCT comparing CRS + HIPEC versus 5-FU-based systemic chemotherapy, which demonstrated a significant OS benefit with median survival of 22 months versus 12 months and 2-year survival of 44 % versus 22 %, respectively [67, 68]. The study also determined that ~5 patients must undergo CRS + HIPEC for one patient to experience survival advantage at 3 years.
Other studies have shown that patients with PC from CRC treated with chemotherapy alone have a median survival of 5–19 months, whereas those treated with CRS + HIPEC for early PC from CRC have reported median survival in the range of 48–63 months and 5-year survival of ~50 % following complete cytoreduction and HIPEC [4]. This data represents significant progress over the past 20 years for what was once thought to be a preterminal condition for which only palliative intervention was previously considered. It is also important to recognize what data is needed in order to further advance and optimize this multimodality treatment approach for PC of CRC origin. This is summarized in Table 5.4. One particular interesting consideration is that of neoadjuvant systemic therapy. Response to neoadjuvant therapy can provide important insights into the biology of disease, tumor response to treatment, and surgical decision making in terms of likelihood of achieving complete cytoreduction. Future clinical trials are likely to address this important unanswered question pertaining to the role of neoadjuvant therapy as part of multimodality treatment in PC from CRC [70].
Patient selection is critical in terms of maximizing oncological benefit of multimodality treatment, with the critical determinant being likelihood of achieving complete cytoreduction (CC 0/1). Clinical decision support systems (CDSS) based on specific clinical, pathological, biomarker, and patient data will ultimately facilitate risk stratification, further enable patient selection for CRS + HIPEC, optimize selection of high-risk patients for PC to undergo second look laparotomy, and individualize multimodality therapy in patients with PSM in CRC [71]. One major problem in patients with PSM of CRC origin is that approximately 50 % will have recurrence of disease after treatment [72, 73], which serves as the fundamental basis for performing a second look operation.
Second Look Concept
Key Concept: Second look laparotomy: …a new plan for early intervention in patients with high risk for local-regional recurrence after primary colon cancer surgery…The high incidence of prolonged survival in this group of patients with early definitive intervention supports the concept of maximal benefit in patients with minimal disease.
– Paul A. Sugarbaker
We have recently reviewed this in detail and will summarize the key points here [20]. Completeness of cytoreduction (CC0/1) and limited peritoneal surface disease (PCI <20) are associated with improved survival following CRS/HIPEC. Importantly, not only is survival improved after CRS + HIPEC for limited PC but also operative morbidity and mortality is significantly reduced because surgery is less extensive. Early peritoneal carcinomatosis is undetectable by conventional imaging or through the use of biomarkers; therein lays the challenge. Second look laparotomy followed by CRS + HIPEC data could only be generated thus far because some groups have performed the so-called second look laparotomy to identify patients that could potentially benefit from second CRS + HIPEC at a time when none of the patients had clinical or radiographic evidence of recurrent PSM [74–76]. The rationale for performing second look laparotomy (generally not laparoscopy, as this modality cannot expose all relevant planes of dissection to ascertain presence of and magnitude of PC) is to identify PSM of CRC origin early in the natural history of the disease in patients at high risk of having disease recurrence. The goal is to identify at-risk patients when tumor volume is below an important clinically detectable threshold, recognizing that completeness of cytoreduction is more readily attained when peritoneal surface disease is of limited extent (PCI <20), where the oncological impact of CRS + HIPEC conducted with curative intent is greatest [37]. As pointed out before [20], the concept of second look operation in cancer is over 60 years old, was probably established in 1948, and first described by Wangensteen in 1949 [5, 77, 78]. Different groups studied the “second look approach” in different tumor types for various indications: cancer staging, palliative treatment in cancer recurrence, and other non-cancer-related diseases, such as mesenteric artery occlusion and in postoperative complication algorithms [5, 27, 72–105]. Esquivel and Sugarbaker investigated a large number of patients with PSM of appendiceal origin during a 12-year period [5, 74]. Out of 321 patients, 98 patients (31 %) underwent second look procedure followed by CRS + HIPEC. The overall 5-year survival rate in these 98 of 321 patients was 74 % compared to 68 % in the remaining 223 of 321 patients. These data clearly show that there is a subpopulation of patients that may benefit from follow-up second look laparotomy and CRS + HIPEC. On the other hand, symptomatic patients, who present with bowel obstruction as a symptom or have a large amount of tumor (PCI >20), have significantly worse survival; hence, patients with a high amount of tumor load have questionable benefit from either second look laparotomy or CRS + HIPEC. In fact, there is no overall survival benefit when CRS is undertaken for patients with PCI exceeding 20 [37]. Maggiori et al. investigated 41 patients with PSM of CRC origin who underwent second look operation and who had no clinical or radiomorphological sign of recurrence at the time of second look. Over half of the patients (23/41, 56 %) underwent subsequent CRS + HIPEC [76]. The reported 5-year overall survival rate was 90 % and 5-year disease-free survival, 44 %. An important finding in this study was that early peritoneal surface recurrence of CRC could be identified absent clinical or radiomorphological signs of disease at a time in its natural history when the oncological benefit of CRS + HIPEC could be maximized. Importantly at-risk asymptomatic patients can be diagnosed with PSM over 50 % of the time. Sugarbaker focused on clinical parameters to identify these at-risk patient in an effort to improve selection and provide clinical decision support to the surgical oncology community; he published suggestions for guidelines for second look operation [72, 73] The major aim of second look operation is to achieve complete tumor resection (R0 resection, CC 0/1 resection). The limited extent of PC that may be identified during the second look in asymptomatic patients lends itself to completeness of tumor resection, estimation of prognosis, and positively impacting patient outcomes through multimodality therapy, CRS + HIPEC. Therefore, patients with limited local–regional recurrence may have more benefit compared to possibly symptomatic patients with a high tumor burden, PCI. Recently, a group of experts in PSM suggested decision support algorithms for patients presenting for the first time with CRC and for those with recurrent CRC or already scheduled for programmed second look operation, which are discussed in the following section. Patients considered at risk for peritoneal carcinomatosis that may benefit from second look laparotomy include patients with perforated primary tumors (iatrogenic or spontaneous), completely resected synchronous limited PC at initial operation, synchronous ovarian metastases, and possibly T4 lesions that required adjacent organ resection and emergency presentation for obstructing/bleeding lesions that underwent surgery.
Decision Making/Preoperative Work-up
Indications and Interdisciplinary Tumor Board
Key Concept: An important element in patient selection for CRS + HIPEC is careful evaluation of the diagnosis and stage of disease as well as resectability of the peritoneal surface malignancy and operability of the patient; the findings of diagnostic testing must be reviewed by an interdisciplinary tumor board in order to arrive at an individualized plan of care.
A patient-centered, integrated, comprehensive, and evidence-based team approach is a “must” in individual cancer therapy. This individualized care approach to patients afflicted by cancer demands that each patient is carefully evaluated, and the findings of diagnostic testing reviewed collectively by a team that in the venue of an interdisciplinary tumor board arrive at an individualized plan of care. All prior patient reports of any treatment intervention, histopathological review, laboratory parameter dynamics during multimodal treatment, and radiomorphological imaging are mandatory elements requiring review by the team prior to treatment recommendations, which must take into account available best level evidence. In addition to such team members as surgical, medical, and radiation oncologists, radiologists, geneticists, pathologists, psychologists, rehabilitation specialists, nurses, as well as students should be involved as part of the interdisciplinary tumor board. An example of an interdisciplinary tumor board structure is shown in Fig. 5.4. Interactions with external stakeholders in academia, administration, and government are shown.


Interdisciplinary tumor board including interactions with academia, administration, and government
The indications for CRS + HIPEC in patients with PSM have been reviewed by several authors [27, 96] and are shown in Table 5.5 [96]. Factors to consider in patient selection for CRS + HIPEC include disease-free interval; extra-abdominal metastases; extent of liver metastases; histology of the primary tumor; local–regional tumor burden (PCI); expected completeness of cytoreduction (CC0/1); patient age, comorbidity, and performance status; carcinomatosis-related complications (SBO, ascites); and prior systemic therapy (toxicity, resistance). A recent expert review of CRS + HIPEC for CRC [20] suggested two clinical decision support algorithms for patients presenting with a diagnosis of CRC (Fig. 5.5) and those who present with CRC recurrence or are already planned for programmed second look laparotomy (Fig. 5.6).


Algorithm for patients with primary CRC at time of primary diagnosis including PSM risk stratification (Modified from: Brücher et al. [20])


Algorithm for patients with CRC, who had been scheduled for second look operation and/or who present with recurrence (Modified from Brücher et al. [20])
Contraindications
Key Concepts: Contraindications to CRS + HIPEC include but are not limited to patient with inability to tolerate the operation (poor performance status), PCI >19, prohibitive medical comorbidities, extra-abdominal metastases, massive retroperitoneal tumor involvement and/or root of mesentery invasion, extensive small bowel disease, >3 liver metastases, and aggressive biology (high grade, signet ring cell).
These can be divided into absolute and relative contraindications [3] (Table 5.6). CRS + HIPEC can only provide survival benefit in patients having good performance status, limited peritoneal surface disease, and those in whom complete cytoreduction is highly likely. Thus, cytoreductive surgery and HIPEC should not be pursued in patients with poor performance status (Karnofsky <70), weight loss ≥10 %, unremitting pain; carcinomatosis-related morbidity (ascites, SBO involving >1 SB segment); prohibitive medical comorbidities (cardiac, pulmonary, renal, hepatic, florid infection); extra-abdominal metastases; massive retroperitoneal involvement or root of mesentery invasion by tumor; extensive small bowel disease (high risk of short-bowel syndrome if resected); unresectable peritoneal disease (PCI ≥20); or aggressive biology (high-grade, signet ring). It is important to note that liver (≤3) metastases and peritoneal disease progression while on chemotherapy are not contraindications for CRS + HIPEC so long as complete cytoreduction can be achieved. CRS is contraindicated in patients with PCI >19, as median survival is no different after CRS/HIPEC than that obtained with systemic therapy alone (~18 months). These decisions in selecting patients for CRS + HIPEC with curative intent are best made in centers of excellence with multidisciplinary teams devoted to the care of patients with PSM.
Quantitative Prognostic Factors (QPIs)
Key Concept: Cross-sectional and functional imaging with CT and CT/positron emission tomography [PET]) is the first-choice diagnostic test in the work-up of peritoneal carcinomatosis; however, these modalities often underestimate preoperative PCI necessitating laparoscopic or open laparotomy staging of extent of disease in order to determine likelihood of CC0/1.
Clinically very important are quantitative prognostic indicators (QPIs) [3], although the quality of the evidence supporting their use in clinical practice varies from one tumor entity to another and high-level published evidence is sometimes lacking. No data are available on tumor markers as qualitative prognostic markers in PSM. With regard to histopathology, the only available data show that patients with poorer differentiation (high-grade, signet ring cell) have worse prognosis than those with well/moderately differentiated cancers. The value of preoperative cross-sectional imaging (CT, MRI) appears to be limited to patients with mucinous PSM. Our own research on the use of preoperative 18F-fluorodeoxyglucose-positron emission tomography and computed tomography (FDG-PET/CT) scanning in comparison with the intraoperative PCI score shows that it has prognostic value [36]. The Sugarbaker PCI score (P < 0.0001) and CC score (P < 0.001) are both clinically relevant prognostic factors in PSM of CRC origin [41].
Ethical Considerations
Key Concept: We must do our best to inform our patients and to enhance their comprehension about their disease and prognosis; most importantly to communicate to them our best estimate of likelihood of cure of their disease.
Independent of the underlying cancer leading to PSM, our society has a kind of Zeitgeist: that peritoneal carcinomatosis means “death soon.” This follows decades of therapeutic nihilism for this stage of cancer. Treatment of patients who suffer from peritoneal carcinomatosis is a burden for both patient and provider, for it is a formidable problem and the treatment is extensive in nature and burdensome itself. This was, is, and always will be a situation that tests our forbearance, our resolve, and at times our faith, as we are often confronted at times with malignancy and intervene at the crossroads of potentially curative and palliative treatment in the face of incompletely defined tumor biology. Combating PSM means being aware about areas of potential ethical conflict: informed consent, treatment refusal, treatment waiver, decision-making ability, capacity to consent, truth at the bedside, truth in the OR, the ICU, confidentiality, research on patients, termination of life-sustaining measures, preserving hope while communicating the actual implications of clinical findings, among others. Dealing with the diagnosis of PSM means to be aware that we must often confront life-limiting challenges. The philosopher Epikur (341–270 ante Christi) stated “Ars moriendi ars vivendi” meaning the art of dying is the art of living. This refers to the process of how to die well and can lead one to conclude that terms such as palliative care, supportive care, or terminal care are second rate and inconsistent with that ethos. Ethics has as one of its main tenets that humans have the freedom to decide. It has been shown that patients with advanced malignancy are willing to accept high-risk interventions and toxic treatments for a slight (even 1 %) chance of cancer cure; at the same time, most patients would not accept such therapy without cure, even if it may significantly increase anticipated survival [97]. A recent study of patients participating in the Cancer Care Outcomes Research and Surveillance (CanCORS) study found that over 80 % of those with CRC did not report understanding that chemotherapy was unlikely to cure their cancer. The authors concluded that “many patients receiving chemotherapy for incurable cancers may not understand that chemotherapy is unlikely to be curative, which could compromise their ability to make informed treatment decisions that are consonant with their preferences” [97]. It is our ethical obligation as human beings and physicians to do our best to inform our patients and to enhance their comprehension about their disease, even if the patient’s satisfaction with the health-care provider and or system is negatively impacted.
Intraoperative Work-up
Cytoreductive Surgery: Logistics, Strategy, and Technique
Key Concepts: High-voltage electrosurgery is utilized for cytoreduction of peritoneal surface malignancy, thereby generating a significant amount of smoke during the procedure which necessitates the use of proper operating room ventilation and a smoke evacuator system used continuously over the surgical field. Heated intraperitoneal chemotherapy is safe for the surgical team and operating room personnel as chemotherapy exposure is negligible, particularly with adherence to universal precautions, and environmental/individual protective measures.
Cytoreductive surgery is a major operation including multiple visceral resections and stripping of peritoneal surfaces. Complex surgical maneuvers such as liver mobilization or full exploration of the omental bursa including the upper recess (the area between the right crura of the diaphragm, liver, and vena cava) and the foramen of Winslow are mandatory to establish CC-0/1 [98]. Therefore, even in the face of limited peritoneal surface disease, cytoreduction is considered a complex abdominal operation and requires a dedicated team and adherence to a comprehensive, standardized preoperative preparation protocol. The HIPEC procedure puts the operating room (OR) and intensive care unit (ICU) personnel within unfamiliar territory at outside their proverbial “comfort zone.” Even in high-volume cancer centers, handling and delivering cytotoxic agents is not a routine in most ORs. Therefore, careful planning and detailed preparation, transport, administration, disposal, and safety protocols should be followed in order to avoid errors risking the patient or OR staff.
Preoperative planning is conducted in two levels. The first level is oncological and the second level is technical.
Oncological Planning
Oncological planning was outlined before (“Indications”) and includes:
-
(a)
Indication for surgery (disease type, disease status, PCI)
-
(b)
Lack of contraindications (extraperitoneal disease, PCI >20, >3 liver metastases, poor performance status)
-
(c)
Surgical history (prior surgical procedures for PSM or resection of primary tumor)
-
(d)
Oncological history (date of diagnosis, age at diagnosis, stage at primary diagnosis, prior treatments delivered, and response evaluation)
In most centers this is done in a tumor board setting and discussed by a multidisciplinary team. In patients that are found to be eligible for CRS + HIPEC, the HIPEC protocol is decided upon and the patient is then scheduled for surgery.
Technical Planning
This is done by a dedicated team including surgical oncologist, anesthesiologist, ICU specialist, medical oncology, OR nurse, nutrition nurse, stoma nurse, pharmacy, and perfusionist.
The procedure is planned according to the following parameters:
Surgical Planning
Type of Disease
Diseases such as disseminated peritoneal adenomucinosis (DPAM) or benign cystic mesothelioma tend to adhere to organs and not to penetrate into the tissue; therefore, they require less visceral resections and result in less surgical trauma and consequent operative morbidity. Other diseases such as serous papillary adenocarcinoma of the ovary or adenocarcinoma of the colon are more likely to penetrate into organs and tissues and as a result require more visceral resections, and the extent of surgical trauma and attendant morbidity are higher [99].
Extent and Location of Disease
The complexity of the procedure, its success, and the rate of postoperative complications are highly correlated with extent of disease as measured by PCI [100]. Volume of disease and location of disease require careful consideration for detailed surgical and anesthetic planning as they may impact postoperative course and recovery. For example, large volume of disease located between the right lobe of the liver and right diaphragm requires liver mobilization and retraction that may result in periods of low blood pressure as a result of vena caval compression. Full stripping of the diaphragm requires the insertion of a chest drain in order to avoid postoperative pleural effusions. Another example is tumor in the abdominal wall. Disease recurrence in surgical scars is common in patients with PSM [101]. When abdominal wall tumor masses exist, careful surgical planning of abdominal wall resection and reconstruction is required.
Approach to “Critical Lesions”
Lesions that are located in places that may have a significant impact on the course or outcome of surgery are defined as “critical lesions.” It is important to distinguish between lesions that will prevent surgery (as part of exclusion criteria or contraindications to surgery) and “critical lesions.” In surgical planning, lesions located in the following areas should be considered critical:
-
1.
Liver hilum: Dissection of the liver hilum is time-consuming and may be associated with increased risk of hemorrhage.
-
2.
Upper recess of lesser sac: Resection of lesions located in this area is technically demanding. Various solutions exist including full mobilization of the liver off the retro-hepatic vena cava and approach from the right side, distal control in the mediastinum by creating a window in the diaphragm and more.
-
3.
Third portion of the duodenum or lesions invading the head of the pancreas: Careful assessment of such lesions should be conducted in order to avoid dissection that will eventually lead to pancreaticoduodenectomy.
-
4.
Pancreatic capsule and hilum of spleen: Such lesions may lead to pancreatic injury and fistula formation.
-
5.
Retroperitoneum: Although retroperitoneal disease is a contraindication for CRS + HIPEC, in many cases, the peritoneal planes were violated by previous surgery, and as a result, peritoneal disease invades the retroperitoneum. In such cases, if complete cytoreduction is achievable, the prognosis of the patients is expected to be the same as disease limited to the abdomen/peritoneal cavity. However, in such patients, ureteral or vascular involvement should be carefully assessed and adequate measures taken including ureteral stenting, planning of ureteral resection and reimplantation, and the possibility of vascular encasement or involvement requiring vascular procedures.
-
6.
Pelvic sidewall: Much like the retroperitoneum, the pelvic sidewall is rarely invaded by tumor deposits in surgery naive patients. However, following pelvic surgery, ureteral or vascular involvement should be carefully assessed and the adequate measures taken including ureteral stenting, planning of ureteral resection and reimplantation, and the possibility of vascular encasement or involvement requiring vascular procedures.
Abdominal Wall Assessment
Abdominal wall assessment is important for surgical planning. Not only the presence, but the location and size of tumor deposits in the abdominal wall, as well as the location of previous scars including trocar sites and drain sites should be taken into consideration and excised; prior midline scar excision includes umbilicus excision. Hernias, either incisional or inguinal-femoral, may harbor tumor deposits and should be recognized and later, during surgery, addressed in a fashion that hernia sacs are completely excised and hernia defects repaired. It is not only important for the prevention of postoperative wound dehiscence, but also for those who use closed perfusion technique for HIPEC, it is important to close all incisions in a way that the chemotherapy cannot leak during perfusion. Therefore, careful history and review of operative reports, physical examination, and detailed review of all cross-sectional imaging is essential for abdominal wall assessment.
Approach to Liver Metastasis
If up to three liver metastases are present, then according to the PSOG consensus statement, the patient is eligible for CRS + HIPEC. In such cases, it is important to carefully calculate the volume of the remaining liver since a “small for size” liver will not only be the result of previous chemotherapy delivered but may also be a result of HIPEC. Intraoperative ultrasound is used to define the location of the liver lesions and to rule out additional lesions missed by the cross-sectional imaging, which can occur in up to 15–20 % of cases that would lead to reconsideration of the intended operation.
For the surgical evaluation high-resolution CT can provide sufficient data, in most cases PET-CT will provide the data required for surgical planning combined with its more important role, to rule out extraperitoneal disease. In selected cases, MRI or MR angiogram (MRA) is required. Staging laparoscopy is used routinely by some, but in most centers, it is used for selected cases both for exclusion of patients and for better operative planning [102].
HIPEC Planning
Most centers use closed HIPEC and some use early postoperative IP chemotherapy (EPIC) protocols (see Table 5.7a–c for suggested protocols in adenocarcinoma of the appendix including pseudomyxoma peritonei and the colon). However, each patient should undergo individual assessment by the CRS/HIPEC team including validation of weight and height, calculation of body surface area, and careful evaluation of:
-
(a)
Prior chemotherapy regimens delivered with special attention to response and toxicity.
-
(b)
Renal, liver, and cardiac function that may necessitate dose modifications.
-
(c)
Dose adjustments should be made for age and comorbid conditions.
After the appropriate protocol is decided upon by the medical and surgical oncologists and all dose modifications are made, the pharmacist, perfusionist, anesthesiologist, and ICU specialist are all informed about the HIPEC ± EPIC protocols to be used. In our practice, the final cytotoxic prescription is written by the medical oncologist and the orders in the patient’s chart are signed by the surgical oncologist.
Anesthesia Planning
Preoperative planning of anesthesia is no different than in every major surgical procedure. By careful history and physical examination, the anesthesiologist can define the operative risk using the ASA classification. Because of the duration of the procedure, the major surgical trauma, and the delivery of chemotherapy, additional tests are routinely applied in most centers. Bell et al. from the Basingstoke group reviewed the perioperative management of patients in medical centers experienced in CRS + HIPEC [103]: anesthesiologists in 41 centers were asked to participate in a web-based questionnaire—the data was completed by 29 centers with a cumulative experience in almost 8,500 patients. In Table 5.8, we summarized the preoperative testing conducted in our center and combined it with the findings of the Basingstoke group’s international survey.
Patients with large volume pseudomyxoma peritonei may have elevated abdominal pressure resulting in reduced functional residual lung capacity leading to a difficulty in ventilation and may also have low venous return to the heart leading to drop in blood pressure during induction of anesthesia or during surgery. Therefore, they all should undergo maximal cardiac and respiratory evaluation before surgery regardless of age.
Nutritional Planning
The general underlying working hypothesis is that all patients undergoing CRS + HIPEC are malnourished. Therefore, nutritional evaluation is conducted to record the level of malnourishment. History and physical examination are the most important. Recent weight loss as percentage of current body weight is essential. Body mass index (BMI), serum albumin, and prealbumin are of less importance unless albumin or prealbumin are very low. In such cases, preoperative nutritional support is recommended. Total parenteral nutrition (TPN) is selectively used by most centers until caloric requirements can be met via the enteral route. In our practice, dedicated central venous access line (PICC line) for TPN is inserted routinely, and TPN is used in all patients until oral diet resumed.
Stoma Planning
All patients are evaluated by a stoma nurse. Detailed education is the initial step followed by physical examination and marking (with the patient in the upright position is the best location for both ileostomy and colostomy). It is of great importance to choose the location of the stoma away from old surgical scars or port sites to be resected during operation.
Perioperative Antibiotic Prophylaxis
All patients undergoing cytoreduction and HIPEC must be covered by IV broad-spectrum antibiotics. In our practice a second-generation cephalosporin + metronidazole are given with induction of anesthesia (30 min before skin incision), re-dosed intraoperatively, and given for up to 5 days if HIPEC is administered. This protocol is modified in cases of allergies or in case of in-hospital infection with bacteria resistant to one of the antibiotic drugs, with resistance documented within the past 6 months.
Venous Thromboembolism Prophylaxis
Subcutaneous low molecular heparin is administrated starting 12 h before surgery until 30 days post-discharge from the hospital.
Mechanical Bowel Preparation
Patients with PSM undergoing CRS + HIPEC are prone to infections due to multifactorial immunosuppression. Therefore, unlike many patients undergoing colonic resections, patients before CRS should undergo bowel preparation. Mechanical bowel preparation combined with oral neomycin and metronidazole is practiced by most centers.
Skin Preparation
In several centers, mainly in Europe, the patient is washed by several antiseptic solutions and following shower is dressed with a paper-sterile gown.
Operating Room
In many centers combined general and thoracic epidural are used. After the insertion of the epidural catheter and induction of anesthesia, the following invasive monitoring lines are inserted:
-
Arterial line
-
High-flow central line
-
Femoral and jugular lines for PiCCO® monitoring
-
Esophageal thermometer
-
Urinary bladder thermometer
The patient is positioned on a temperature control device (CritiCool® Systems, MTRE™, Mennen Medical Corp, Feasterville-Trevose, PA, USA). The patient is wrapped by a blanket containing fluid at a certain temperature set by the operator. By multi-temperature sensing, the temperature of the patient is managed at a level set by the anesthesiologist. During the HIPEC procedure, the device is used to cool the patient achieving a fixed temperature of 37 °C for the entire procedure. By using this microprocessor-controlled temperature management unit, using feedback from the patient’s core and skin temperature sensors, the proprietary control algorithm responds by modifying water temperature such that patient target temperature will be achieved precisely.
Induction of Anesthesia and Monitoring
In most patients, induction of anesthesia is no different than for any other major abdominal operation. However, in patients with pseudomyxoma peritonei or large intra-abdominal tumor masses, large quantity of mucin or ascites, rapid sequence intubation is recommended due to increased risk of aspiration. Another important consideration in such patients is decreased venous return to the heart due to inferior vena caval compression resulting in a sudden drop in blood pressure [104].
Following induction of general endotracheal anesthesia and multiple line placements, the patient is positioned in the lithotomy position (Fig. 5.7). Intermittent compression stockings are applied to the lower extremities of all patients and activated from entrance to the operating room until the fifth postoperative day. Positioning, padding points of pressure, and securing location of lines and devices are carefully confirmed before the patient is draped.


Patient positioning for CRS + HIPEC
Hemodynamic monitoring during the procedure is essential. Some centers use advanced hemodynamic monitoring such as LIDCO® (LidcoLtD, Cambridge, UK) [105] or NICOM® (Cheeta Medical™, Tel Aviv, Israel) [106] with less invasive nature or the pulse-induced contour cardiac output (PiCCO®, Philips Healthcare, Andover, MA, USA). This is a device that quantifies several parameters, including continuous (pulse contour) cardiac output, cardiac preload, systemic vascular resistance, and extravascular lung water (EVLW). The patient requires a central venous line and an arterial line placed in the femoral artery [107].
Surgical Technique
Key Concept: Cytoreductive surgery, heated intraperitoneal chemotherapy, and systemic chemotherapy select patients with colorectal cancer carcinomatosis are not competitive, rather complementary therapies.
After the patient is prepped and draped, a self-retaining retractor is assembled. A midline incision including the umbilicus and all previous scars is made from the xiphoid to the pubis (Fig. 5.8). Usually in case of PSM due to CRC, patients had been operated before. Scars should be excised, as tumor cells can be implanted within those. If a patient had a former median midline laparotomy from the xiphoid to the pubis, the umbilicus needs to be excised also. The completion of the laparotomy is done later to allow a complete abdominal exposure.


Midline abdominal incision
The linea alba is opened keeping the peritoneum intact. The parietal peritoneum is then stripped down to the paracolic gutters (Fig. 5.9) and a small window is created to inspect the abdomen. Adhesions are lysed and mucin, if present, is aspirated using a large-caliber suction tube (Fig. 5.10).


Extraperitoneal dissection to the paracolic gutters


Aspiration of mucin using a large-caliber suction tube
In order to have the best available exposure, large masses such as bulky ovarian metastasis or omental cake are removed first. A second exploration is then made in order to be certain to the degree possible that complete cytoreduction (CC 0/1) is achievable. Peritonectomy procedures (Table 5.9) are then performed according to the methods described by P.H. Sugarbaker and anastomoses completed prior to HIPEC per surgeon preference [108].
Cytoreductive surgery in PSM does not mean complete routine stripping of the peritoneal wall; it means to resect the tumor-involved areas only. Due to former operations, any adhesions have to be cleared, the liver as well as the mesenteric root has to be mobilized completely, and areas of potential pitfalls have to be cleared as well such as the retro-hepatic caval area, hepatoduodenal ligament, umbilical fissure, etc. as indicated. After completion of adhesiolysis, the parietal peritonectomy can be performed in parts: ventral wall, left and right upper quadrant, as well as middle right and left abdominal peritoneum and pelvis. Sugarbaker described 6 peritonectomy procedures:
-
1.
Total anterior parietal peritonectomy
-
2.
Greater omentectomy [with or without splenectomy]
-
3.
Right subphrenic peritonectomy
-
4.
Left subphrenic peritonectomy
-
5.
Pelvic peritonectomy
-
6.
Lesser omentectomy with or without cholecystectomy
The parietal peritonectomy procedures usually do not require blood replacement. Afterwards, additional visceral required cytoreductive surgical procedures can be performed. It remains the choice of the surgeon whether to perform anastomosis before or after HIPEC. We suggest a double-sutured hand anastomosis. In the case of a high-risk low rectal anastomosis, it might be necessary to perform a fecal diversion or a defunctioning stoma. This stoma can be closed within 3 months after postoperative recovery and prior to commencing further adjuvant chemotherapy, in case it is needed.
After the parietal peritonectomy and the necessary visceral resections, HIPEC is administered. For the coliseum technique, the ventral wall is sutured onto the retractor system and lifted up. Afterwards, the drains (from the HIPEC machine to the patient and those from the patient to the machine) are inserted. After the HIPEC is completed with all the necessary documentation of patient temperatures, the abdomen is usually washed out with 8–10 L of saline. A summary of the possible surgical resections in PSM differentiated into parietal and visceral procedures (when possible) is shown in Table 5.9.
Perioperative Chemotherapy
Preparation for perfusion should start 2 h before estimated time of perfusion. Urine output should be measured every 15 min with a minimum requirement of 25 mL in 15 min. Urine output may be increased by using low dose furosemide or by a drip of dopamine at a low diuretic dose. The patient’s temperature should be maintained between 35 and 37 °C. Using a standard heating device may create a challenge to keeping the temperature in this range; on the other hand, use of a multisensor temperature control device with both warming and cooling capabilities makes temperature-keeping a lot easier.
In centers that use concomitant systemic 5-FU and leucovorin, intravenous (IV) folinic acid (leucovorin) is administrated 1 h before IV administration of 5-flourouracil. Following the administration of IV 5-flourouracil, the patient is connected to the perfusion device and perfusion with 0.9 % NaCl is commenced (we use the closed method). Platinum compounds such as cisplatinum or oxaliplatinum are best preserved in D5W solution, but in the short-term (30–60 min) delivery of these compounds in the HIPEC setting, the amount of the degradation of the drug in 0.9 % NaCl is minimal. If perfusion is conducted using D5W, hyponatremia should be prevented by intravenous administration of 0.9 % NaCl solution.
Temperature is measured by five probes (Fig. 5.11):


Five-probe temperature monitoring output
-
(a)
Patient esophageal probe
-
(b)
Patient bladder probe (tissue heating probe)
-
(c)
Device (heat exchanger)
-
(d)
Inflow
-
(e)
Outflow
Average temperature is calculated as T inflow + T outflow/2
Once inflow temperature of 44 °C and average temperature is above 41 °C, chemotherapy is added to the reservoir and HIPEC commences. All team members present in the operating theater are dressed with eye protection, masks, waterproof gowns, and non-permeable gloves in accordance with institutional safety standards [109, 110].
In the closed technique, it is advised to measure intra-abdominal pressure by a catheter introduced into the peritoneal cavity before closure connected to a transducer and a monitor. Intra-abdominal pressure should not exceed 25 mmHg.
At this point antiemetics are administrated in order to prevent postoperative nausea and vomiting.
At the end of the HIPEC procedure, all waste is disposed into special containers designated for cytotoxic disposal and marked accordingly.
The patient is transferred to the ICU where cytotoxic isolation of all secretions is maintained for additional 72 h.
Early Postoperative Intraperitoneal Chemotherapy (EPIC)
Administration of EPIC is done in most centers in the ICU or in step-down units. Delivery of EPIC can be performed either through the HIPEC inflow and outflow tubes left at the time of surgery or through a peritoneal port inserted at the time of surgery. EPIC protocols vary between institutions; though in most cases, 5-day protocols incorporating an agent such as 5-flourouracil are different then when the cytotoxic agents perfused during HIPEC are selected.
Complete CRS Not Achievable: What Now?
The completeness of cytoreduction is classified according to the CC score [41] and CC 0/1 is the goal of CRS. If it is clear that a CC 0/1 resection cannot be achieved, then there is certainly no role for HIPEC. The outcome of CC 2/3 resection for PSM of CRC origin, in terms of overall survival, is no different than with systemic therapy alone. Hence, no major cytoreductive procedure should be undertaken. If visceral obstruction is present, a stoma should be avoided if possible and bypass operation should be considered. Any kind of additional operation, particularly splenectomy, cholecystectomy, or other multivisceral operation is not indicated when complete cytoreduction cannot be attained. If there is diffuse gastric involvement by tumor, a percutaneous gastrostomy tube should be considered along with jejunostomy feeding tube placement.
Postoperative Considerations
Key Concept: Cytoreductive surgery and HIPEC requires an experienced and dedicated team within a center of excellence committed to the care of patients with peritoneal surface malignancy. In the best of hands, operative morbidity (Grade 3 and 4) and mortality are ~30 and 3 %, respectively.
Morbidity and Mortality
Key Concept: The goal is to identify patients with peritoneal carcinomatosis early in the course of their disease, as postoperative morbidity and mortality are significantly lower when the extent of peritoneal disease is low, because operation is less extensive on this basis. CRS + HIPEC is a very complex surgical endeavor with a steep learning curve (~150 cases for attaining acceptable competence including adequate radicality of resection and acceptable operative morbidity and mortality). These complex operations should be conducted in dedicated centers of excellence with adequate experience in CRS + HIPEC.
According to the literature, the postoperative morbidity rates ranges from 14 to 40 % [38, 111–115]. The major concern in the postoperative morbidity of patients after CRS + HIPEC is that it is substantially different from the familiar morbidity/mortality associated with other so-called traditional surgical procedures. Pain as one of the major signs of perioperative morbidity typically does not occur after peritonectomy when complications develop. Patients with complications are usually identified clinically due to fatigue, failure to progress, fever, tachycardia, or leukocytosis or thrombocytosis. Simultaneous pancytopenia occurring after HIPEC may aggravate the situation even more. A heightened awareness and index of suspicion as well as aggressive postoperative diagnostic approach are absolutely necessary, because the central symptom of potential postoperative morbidity “pain” is seldom reported after peritonectomy.
Cytoreductive surgery with HIPEC is associated with high morbidity and mortality in the range 0–12 % (Table 5.10). The high morbidity and mortality are related to the extent of surgery, the effects of perioperative chemotherapy, effects of hyperthermia, and to the impaired immune response of patients with metastatic disease and prior systemic chemotherapy. In a recent publication, Glehen et al. [118] presented data from 25 French-speaking institutions reporting morbidity and mortality after 1,344 cytoreductive surgery and HIPEC procedures or early EPIC conducted in 1,290 patients with peritoneal carcinomatosis from non-gynecologic malignancies. They found Grades 3 and 4 complications in 403 patients (34 %) with reoperation rate of 14 %, enterocutaneous fistula in 10 %, bleeding in 8 %, intra-abdominal abscess in 7 %, and sever neutropenia in 13 % of patients. The mean hospital stay was 24 ± 17 days. They identified three significant risk factors for complication: age, extent of disease (PCI), and institution (low volume). A report from an international registry of 506 patients reported a mortality of 4 % and severe morbidity of 23 %, with GI fistula occurring in 8 % [119]. Another recent report of 2,298 patients treated at 16 high-volume centers with CRS + HIPEC for pseudomyxoma peritonei [120] cited treatment-related mortality in 2 % and major operative complications in 24 %.
There are many reports of complications associated with CRS + HIPEC, with some variability of the major morbidity between 20–40 % and mortality of 0–12 %. This variability stems from the different definitions of major complications, lack of uniform reporting system for surgical complications, variability in patients, disease types, and individual center’s volume and expertise [45, 100, 116, 121–132]. Like in any other complex surgical technique, there is a learning curve [133]. Learning and assimilating a new technology is a complex process; therefore, there are two learning curves to consider: a surgeon’s learning curve and an institution’s learning curve—reaching a plateau after 100–140 cases within a single center [134]. Learning curve and the rate of morbidity and mortality associated with it can be significantly reduced in a new HIPEC program with close mentorship of a high-volume center as was shown by the Milan group [135–137].
Complication Management and Patient Follow-Up
Since the morbidity of CRS + HIPEC is high, in order to reduce mortality, several topics should be addressed before initiating a HIPEC program:
-
1.
Nursing staff acquainted with complex gastrointestinal surgery that may alert the surgeon of any clinical deterioration in a timely manner.
-
2.
Mid-high level residents (postgraduate year 3–5) or available staff on call that can address any clinical issue early on.
-
3.
Availability of a high-quality invasive radiology service.
-
4.
Availability of an operating theater for emergency 24 h a day, 7 days a week.
-
5.
Availability of ICU beds for readmission of the patient with major complication if needed.
Most complications are related to the operative procedure and should be addressed the same way surgical complications are addressed in every patient following abdominal surgery. In addition, most common complications associated with HIPEC include paralytic ileus related not only to the surgical procedure but also to the impact of heat on the enteric nervous system [138], neutropenia associated with systemic absorption of some of the HIPEC agents with bone marrow suppression ability, and hepatotoxicity of some agents such as mitomycin C or oxaliplatinum [123]. Renal failure is a known adverse event of cisplatinum and can be prevented by perioperative administration of IV sodium thiosulfate. Wound necrosis and infection may be associated with cytotoxic effect of the HIPEC or EPIC agents. Many of the abdominal wall closures require synthetic or biological graft placement, and there is only scarce data regarding the impact of cytotoxic agents on these materials [139].
Pearls and Practical Tips in Peritoneal Cytoreductive Surgery
-
1.
Low lithotomy position is preferred for CRS.
-
2.
Strong suction apparatus is necessary to control the spoke resulting from high-energy cautery used for cytoreduction.
-
3.
The preferred anastomotic technique is hand-sewn anastomosis in two layers. We recommend outer layer with 3.0 sutures (PDS or Vicryl) and internal layer with 4.0 PDS.
-
4.
Generally, chromic sutures are not used for anastomosis. The best results in our experimental and clinical experience are attained with PDS or Prolene suture. Some groups use Vicryl for the outer layer of the double-sutured anastomosis.
-
5.
Do not use anti-adhesive barriers around an anastomosis if cytoreductive surgery includes an anastomosis.
-
6.
We use 10 L of water irrigation after HIPEC to reduce postoperative intra-abdominal infection.
-
7.
We recommend against irrigating the peritoneal cavity with saline after HIPEC. Patients receiving peritoneal irrigation with saline following oxaliplatin/HIPEC tend to get hyponatremic after the operation. What’s more, the oxaliplatin will precipitate in saline, whereas it is diluted in D5W.
-
8.
Major hepatobiliary or pancreatic resections, though generally regarded as contraindications to cytoreductive surgery, can be safely undertaken in selected cases when all grossly apparent disease can be cleared (CC0/1) surgically.
-
9.
If major liver resection is undertaken with cytoreductive surgery, early liver dysfunction is common, but liver failure is uncommon in patients with normal preoperative liver function.
-
10.
If we perform a major liver resection during CRS, we place topical hemostatic over the cut surface and then leave a moist lap pad against the cut surface during the HIPEC because of the negative pressure exerted by the outgoing tube, which can generate bleeding from the liver surface.
-
11.
We are especially mindful of this bleeding risk and pay close attention to the appearance of the peritoneal fluid return early in the course of HIPEC for signs of liver hemorrhage.
-
12.
Prior to major liver resection, it is our practice to administer vitamin C, 1.0 g twice daily, for at least a week prior to operation.
-
13.
Furthermore, we continue intravenous vitamin C postoperatively, including zinc and multivitamin supplementation in an effort to improve surgical wound healing.
-
14.
In patients that receive intraoperative chemotherapy, we administer prophylactic antibiotics for 5 days following operation.
-
15.
Patients are kept on strict contact precautions until the leukopenia and thrombocytopenia commonly encountered after perioperative chemotherapy resolves.
-
16.
The critical parameter in assessing the impact of cytoreductive surgery and patient prognosis is postoperative PCI.
-
17.
Cytoreductive surgery is complex and places a significant burden on both the patient and the surgeon. If it is possible to render the patient free of all grossly apparent disease (CC0/1), then all reasonable efforts should be undertaken to that end.
-
18.
Even in the presence of extensive miliary disease with 1–2 mm lesions implanted throughout the peritoneal cavity, we endeavor to take the time it takes to meticulously remove all apparent disease, one lesion at a time using low voltage argon beam coagulator with short bursts. Furthermore, we gently scrape to the lesion from the bowel with the back of a scalpel, and if needed place one or two seromuscular stitches at the ablated site to reduce the risk of consequent fistula formation.
-
19.
Some groups of experts prefer performing selective peritonectomy and some a complete peritonectomy (including peritoneum with and without grossly evident tumor implants) at time of cytoreductive surgery.
-
20.
It is our practice to resect the ovaries, greater omentum, and lesser omentum-hepatogastric ligament during cytoreductive surgery.
-
21.
We prefer to perform cytoreduction before the HIPEC and to complete the reconstruction/anastomoses after the HIPEC. Bowel edema with 30 min of oxaliplatin/HIPEC does not appear to be clinically significant. This is different if groups perform 90 min of HIPEC.
-
22.
Prior to anastomosis following HIPEC, we trim back the bowel edges to get rid of any potential malignant cells along the stapled edge that were exposed to HIPEC.
-
23.
For prolonged cytoreductive cases (>8 h), we keep patients intubated on mechanical ventilation overnight in the ICU.
-
24.
For patients requiring subtotal colectomy, we prefer to retain the cecum and preserve the ileocecal valve whenever possible, as fluid and electrolyte management for the next 1 year while on systemic chemotherapy is so much simpler than in cases where the ileocecal valve is resected. In cases where the cecum appears diseased, we make every effort to ablate as much of the disease as possible and bring most of the cecum outside the abdomen as a matured stoma, leaving the ileocecal valve within the peritoneal cavity.
-
25.
As we plan a second look laparotomy within 1 year following CRS/HIPEC in all our patients, we prefer anastomosis when colectomy is performed.
-
26.
If in the course of peritoneal stripping off the hemidiaphragm, we breach the diaphragm and identify it only after the HIPEC, we then insert a small chest tube to treat the inevitable effusion that ensues.
-
27.
Our suture of choice for diaphragmatic repair is Prolene monofilament.
-
28.
Great care must be taken when performing peritoneal stripping in the region of the pericardium so as to avoid a breach of that membrane.
-
29.
If one can avoid splenectomy during the course of CRS, then one should. In cases where splenectomy is anticipated, vaccination is administered prior to operation.
-
30.
If resection of the pancreas is required during CRS for clearance of all apparent disease, then we leave peripancreatic drains to closed, low-pressure suction.
Abbreviations
- BMI:
-
Body mass index
- CC score:
-
Completeness of cytoreduction score
- CDSS:
-
Clinical decision support systems
- CRC:
-
Colorectal cancer
- CRS:
-
Cytoreductive surgery
- CT:
-
Computed tomography
- CTR-1:
-
Copper transport protein-1
- DPAM:
-
Disseminated peritoneal adenomucinosis
- EPIC:
-
Early postoperative IP chemotherapy
- HIPEC:
-
Hyperthermic intraperitoneal Chemotherapy
- ICU:
-
Intensive care unit
- IV:
-
Intravenous
- NCCTG:
-
North Central Cancer Treatment Group
- OR:
-
Operating room
- PC:
-
Peritoneal carcinomatosis
- PCI:
-
Peritoneal cancer index
- PSM:
-
Peritoneal surface malignancy
- QOL:
-
Quality of life
- RCT:
-
Randomized controlled trial
- TPN:
-
Total parenteral nutrition
References
Siegel R, Naishadham D, Jemal A. Cancer statistics 2012. CA Cancer J Clin. 2012;62(1):10–29. doi:10.3322/caac.20138. Epub 2012 Jan 4.
Siegel R, Naishadam D, Jemal A. Cancer statistics for Hispanics/Latinos 2012. CA Cancer J Clin. 2012;62(5):2883–98. doi:10.3322/caa.21153.
Brücher BLDM, Piso P, Verwaal V, Esquivel J, Derraco M, Yonemura Y, Gonzalez-Moreno S, Pelz J, Königsrainer A, Ströhlein M, Levine EA, Morris D, Bartlett D, Glehen O, Garofalo A, Nissan A. Peritoneal carcinomatosis: cytoreductive surgery and HIPEC–overview and basics. Cancer Invest. 2012;30(3):209–24.
Itzhak A, Brücher BLDM, Nissan A, Stojadinovic A. Randomized clinical trials for colorectal cancer peritoneal surface malignancy. Surg Clin North Am. 2012;21:665–88.
Griffen Jr WO, Gilbertsen VA, Wangensteen OH. The second look operation for abdominal malignancies 1948–1963. Natl Cancer Inst Monogr. 1964;15:267–76.
Brücher BLDM, Roder JD, Fink U, Stein HJ, Busch R, Siewert JR. Prognostic factors in resected primary small bowel tumors. Digestive Surgery. 1998;15:42–51.
Xu DZ, Zhan YQ, Sun XW, Cao SM, Geng QR. Meta-analysis of intraperitoneal chemotherapy for gastric cancer. W J Gastroenterol. 2004;15(10):2727–30.
Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, Copeland LJ, Walker JL, Burger RA. Gynecologic Oncology Group. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med. 2006;354(1):34–43.
Jayne DG, Fook S, Loi C, Seow-Choen F. Peritoneal carcinomatosis from colorectal cancer. Br J Surg. 2002;89(12):1545–50.
Chu DZ, Lang NP, Thompson C, et al. Pertoneal carcinomatosis in nongynecological malignancy: a prospective study of prognostic factors. Cancer. 1989;63:364–7.
Blair SL, Chu DZ, Schwarz RE. Outcome of palliative operations for malignant bowel obstruction in patients with peritoneal carcinomatosis from nongynecological cancer. Ann Surg Oncol. 2001;8:632–7.
Sugarbaker PH, Gianola FJ, Speyer JC, Wesley R, Barofsky I, Meyers CE. Prospective randomized trial of intravenous versus intraperitoneal 5-fluorouracil in patients with advanced colon and rectal cancer. Surgery. 1985;98(3):414–22.
Sugarbaker PH, Gianola FJ, Speyer JC, Wesley R, Barofsky I, Myers CE. Prospective randomized trial of intravenous versus intraperitoneal 5-FU in patients with advanced colon and rectal cancer. Semin Oncol. 1985;12(3 Suppl 4):1–11.
Gilly F, Carry PY, Sayag AC, Braillon GB, Volloch AA, Panteix GG, James IM, Chatelard PA. Treatment of peritoneal carcinomatosis by intraperitoneal chemot-hyperthermia with Mtomycin C. Initial experience. Ann Chir. 1990;44(7):545–51.
Gilly FN, Beaujard A, Glehen O, Grandclement E, Caillot JL, Francois Y, Sadeghi-Looyeh B, Gueugniaud PY, Garbit F, Benoit M, Bienvenu J, Vignal J. Peritonectomy combined with intraperitoneal chemohyperthermia in abdominal cancer with peritoneal carcinomatosis: phaseI-II study. Anticancer Res. 1999;19(3B):2317–21.
Gilly FN, Carry PY, Sayag AC, Brachet A, Panteix G, Salle B, Bienvenu J, Burgard G, Guibert B, Banssillon V, Braillon G. Regional chemotherapy and intraoperative hyperthermia for digestive cancers with peritoneal carcinomatosis. Hepatogastroenterology. 1994;41:124–9.
Sugarbaker PH. New standard of care for appendiceal epithelial malignancies and pseudomyxomaperitonei syndrome. Lancet Oncol. 2006;7:69–76.
Sadeghi B, Arvieux C, Glehen O, Beaujard AC, Rivoire M, Baulieux J, Fontaumard E, Brachet A, Caillot JL, Faure JL, Porcheron J, Peix JL, Francois Y, Vignal J, Gilly FN. Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study. Cancer. 2000;88(2):358–63.
Elias D, GIlly F, Boutitie F, Quenet F, Bereder JM, Manavelt B, Lorimier G, Dube P, Glehen O. Peritoneal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: retrospective analysis of 523 patients from a multicentric French study. J Clin Oncol. 2010;28(1):63–8.
Brücher BLDM, Stojadinovic A, Bilchik A, Nissan A, Avital I. Identifying patient at risk of peritoneal surface malignancy of colorectal cancer origin. The role of 2nd look laparotomy. J Cancer. 2013;4:262–9.
Baron MA. Structure of the intestinal peritoneum in man. Am J Anat. 1941;69:439–97.
Flessner M, Henegar J, Bigler S, Genous L. Is the peritoneum a significant transport barrier in peritoneal dialysis. Perit Dial Int. 2003;23:542–9.
Sugarbaker PH. Peritoneum as the first line of defense in carcinomatosis. J Surg Oncol. 2007;95:93–6.
Stelin G, Rippe B. A phenomenological interpretation of the variation in dialysate volume with dwell time in CAPD. Kidney Int. 1990;38:465–72.
Sugarbaker PH, Schellinx ME, Chang D, Koslowe P, von Meyerfeldt M. Peritoneal carcinomatosis from adenocarcinoma of the colon. World J Surg. 1996;5:585–91.
Yonemura Y, Bandou E, Kawamura T, Endou Y, Sasaki T. Quantitative prognostic indicators of peritoneal dissemination of gastric cancer. Eur J Surg Oncol. 2006;32:602–6.
Gonzalez-Moreno S, Ortega-Perez G, Gonzalez-Bayon L. Indications and patient selection for cytoreductive surgery and perioperative intraperitoneal chemotherapy. J Surg Oncol. 2009;100:287–92.
Rufián S, Muñoz-Casares FC, Briceño J, Diaz CJ, Rubio MJ, Ortega R, Ciria R, Morillo M, Aranda E, Muntane J, Pera C. Radical surgery–peritonectomy and intraoperative intraperitoneal chemotherapy for the treatment of peritoneal carcinomatosis in recurrent or primary ovarian cancer. J Surg Oncol. 2006;94:316–24.
Warrick C. An improvement on the practice of tapping; whereby that operation instead of a relief of symptoms, becomes an absolute cure for an ascites, exemplified in the case of Jane Roman; and recommended to the consideration of the Royal Society, by Christopher Warrick, of Turo, Surgeon. Philos Trans R Soc Lond B Biol Sci. 1744;43:12–9.
Ceelen WP, Flessner MF. Intraperitoneal therapy for peritoneal tumors: biophysics and clinical evidence. Nat Rev Clin Oncol. 2010;7:108–15.
Weisberger AS, Levine B, Storaasli JP. Use of nitrogen mustard in treatment of serous effusions of neoplastic origin. J Am Med Assoc. 1955;159:1704–7.
Dedrick RL, Myers CE, Bungay PM, De Vita VT. Pharmacokinetic rationale for peritoneal drug administration in the treatment of ovarian cancer. Cancer Treat Rep. 1978;62:1–11.
Avantunde AA, Parson SL. Pattern and prognostic factors in patients with malignant ascites: a retrospective study. Ann Oncol. 2007;18(5):945–9.
Flessner M, Choi J, Credit K, Deverkadra R, Henderson K. Resistance of tumor interstitial pressure to the penetration intraperitoneally delivered antibodies into metastatic ovarian tumors. Clin Cancer Res. 2005;11:3117–25.
Holzer AK, Samimi G, Katano K, Naerdemann W, Lin X, Safaei R, Howell SB. The cooper influx transporter human cooper transport protein 1 regulates the uptake in human ovarian carcinoma cells. Mol Pharmacol. 2004;66(4):817–23.
Pfannenberg C, Konigsrainer I, Aschoff P, Öksüz M, Zieker D, Beckert S, Symons S, Nieselt K, Glatzle J, Brücher BLDM, Claussen CD, Konigsrainer A. 18F-FDG-PET/CT to select patients with peritoneal carcinomatosis for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2009;16(5):1295–303.
Jacquet P, Sugarbaker PH. Current methodologies for clinical assessment of patients with peritoneal carcinomatosis. J Exp Clin Cancer Res. 1996;15:49–58.
Verwaal VJ, Van Tinteren H, Van Ruth S, Zoetmulder FAN. Predicting the survival of patients with peritoneal carcinomatosis of colorectal origin treated by aggressive cytoreduction and hyperthermic intraperitoneal chemotherapy. Br J Surg. 2004;91:739–46.
Kajitani T, Japanese Research Society for Gastric Cancer. The general rules for the gastric cancer study in surgery and pathology. Part I. Clinical classification. Jpn J Surg. 1981;11:127–39.
Esquivel J, Sticca R, Sugarbaker P, Levine E, Yan TD, Alexander R, Baratti D, Bartlett D, Barone R, Barrios P, Bieligk S, Bretcha-Boix P, Chang CK, Chu F, Chu Q, Daniel S, de Bree E, Deraco M, Dominguez-Parra L, Elias D, Flynn R, Foster J, Garofalo A, Gilly FN, Glehen O, Gomez-Portilla A, Gonzalez-Bayon L, Gonzalez-Moreno S, Goodman M, Gushchin V, Hanna N, Hartmann J, Harrison L, Hoefer R, Kane J, Kecmanovic D, Kelley S, Kuhn J, LaMont J, Lange J, Li B, Loggie B, Mahteme H, Mann G, Martin R, Misih RA, Moran B, Morris D, Onate-Ocana L, Petrelli N, Philippe G, Pingpank J, Pitroff A, Piso P, Quinones M, Riley L, Rutstein L, Saha S, Alrawi S, Sardi A, Schneebaum S, Shen P, Shibata D, Spellman J, Stojadinovic A, Stewart J, Torres-Melero J, Tuttle T, Verwaal V, Villar J, Wilkinson N, Younan R, Zeh H, Zoetmulder F, Sebbag G. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in the management of peritoneal surface malignancies of colonic origin: a consensus statement. Society of Surgical Oncology. Ann Surg Oncol. 2007;14:128–33.
Sugarbaker PH. Peritonectomy procedures. Surg Oncol Clin N Am. 2003;12:703–27.
Sugarbaker PH. Successful management of microscopic residual disease in large bowel cancer. Cancer Chemother Pharmacol. 1999;43(Suppl):S15–25.
Sugarbaker PH, Chang D. Results of treatment of 385 patients with peritoneal surface spread of appendiceal malignancy. Ann Surg Oncol. 1999;6:727–31.
Glehen O, Cotte E, Kusamura S, Deraco M, Baratti D, Passot G, Beaujard AC, Noel GF. Hyperthermic intraperitoneal chemotherapy: nomenclature and modalities of perfusion. J Surg Oncol. 2008;98:242–6.
Chua TC, Yan TD, Saxena A, Morris DL. Should the treatment of peritoneal carcinomatosis by cytoreductive surgery and hyperthermic intraperitoneal chemotherapy still be regarded as a high morbid procedure ? Ann Surg. 2009;249:900–7.
Gonzalez-Moreno S, Kusamura S, Baratti D, Deraco M. Postoperative residual disease evaluation in the locoreginal treatment of peritoneal surface malignancy. J Surg Oncol. 2008;98:237–41.
Sugarbaker PH. Observations concerning cancer spread within the peritoneal cavity and concepts supporting an ordered pathophysiology. In: Sugarbaker PH, editor. Peritoneal carcinomatosis: principles of management. Boston: Kluwer; 1996. p. 79–100.
Ozel L, Ozel MS, Toros AB, Kara M, Ozkan KS, Tellioglu G, Krand O, Koyuturk M, Berber I. Effect of early preoperative 5-fluorouracil on the integrity of colonic anastomoses in rats. World J Gastroenterol. 2009;15(33):4156–62.
Pelz JO, Doerfer J, Decker M, Dimmler A, Hohenberger W, Meyer T. Hyperthermic intraperitoneal chemoperfusion (HIPEC) decrease wound strength of colonic anastomosis in a rat model. Int J Colorectal Dis. 2007;22:941–7.
Van der Speeten K, Stuart OA, Sugarbaker PH. Using pharmacologic data to plan clinical treatments for patients with peritoneal surface malignancy. Curr Drug Discov Technol. 2009;6:72–81.
Sugarbaker PH, Graves T, DeBruijn EA, Cunliffe WJ, Mullins RE, Hull WE, Oliff L, Schlag P. Rationale for early postoperative intraperitoneal chemotherapy (EPIC) in patients with advanced gastrointestinal cancer. Cancer Res. 1990;50:5790–4.
Sugarbaker PH, Mora JT, Carmignani P, Stuart OA, Yoo D. Update on chemotherapeutic agents utilized for perioperative intraperitoneal chemotherapy. Oncologist. 2005;10:112–22.
Lepock JR. How do cells respond to their thermal environment? Int J Hyperthermia. 2005;21:681–7.
Kusumoto T, Holden SA, Teicher BA. Hyperthermia and platinum complexes: time between treatments and synergy in vitro and in vivo. Int J Hyperthermia. 1995;11:575–86.
Barlogie B, Corry PM, Drewinko B. In vitro thermochemotherapy of human colon cancer cells with cis-dichlorodiammineplatinum (II) and mitomycin C. Cancer Res. 1980;40:1165–8.
Jacquet P, Averbach A, Stuart OA, Chang D, Sugarbaker PH. Hyperthermic intraperitoneal doxorubicin: pharmacokinetics, metabolism, and tissue distribution in a rat model. Cancer Chemother Pharmacol. 1998;41:147–54.
Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med. 2000;343(13):905–14.
Douillard JY, Cunningham D, Roth AD, et al. Irinotecan combined with fluorouracil compared with fluorouracil alone as first-line treatment for metastatic colorectal cancer: a multicentre randomised trial. Lancet. 2000;355(9209):1041–7.
Giacchetti S, Perpoint B, Zidani R, et al. Phase III multicenter randomized trial of oxaliplatin added to chronomodulated fluorouracil-leucovorin as first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2000;18(1):136–47.
Rothenberg ML, Oza AM, Bigelow RH, et al. Superiority of oxaliplatin and fluorouracil-leucovorin compared with either therapy alone in patients with progressive colorectal cancer after irinotecan and fluorouracil-leucovorin: interim results of a phase III trial. J Clin Oncol. 2003;21(11):2059–69.
Goldberg RM, Sargent DJ, Morton RF, et al. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol. 2004;22(1):23–30.
Tournigand C, Andre T, Achille E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol. 2004;22(2):229–37.
Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335–42.
Colucci G, Gebbia V, Paoletti G, et al. Phase III randomized trial of FOLFIRI versus FOLFOX4 in the treatment of advanced colorectal cancer: a multicenter study of the Gruppo Oncologico Dell’Italia Meridionale. J Clin Oncol. 2005;23(22):4866–75.
Goldberg RM, Sargent DJ, Morton RF, et al. Randomized controlled trial of reduced-dose bolus fluorouracil plus leucovorin and irinotecan or infused fluorouracil plus leucovorin and oxaliplatin in patients with previously untreated metastatic colorectal cancer: a North American Intergroup Trial. J Clin Oncol. 2006;24(21):3347–53.
Franko J, Shi Q, Goldman CD, Pockaj BA, Nelson GD, Goldberg RM, Pitot HC, Grothey A, Alberts SR, Sargent DJ. Treatment of colorectal peritoneal carcinomatosis with systemic chemotherapy: a pooled analysis of North Central Cancer Treatment Group Phase III Trials N971 and N9841. J Clin Oncol. 2012;30:263–76.
Verwaal V, Ruth S, Bree E, et al. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol. 2003;21:3737–43.
Verwaal VJ, van Ruth S, Witkamp A, Boot H, van Slooten G, Zoetmulder FA. Long-term survival of peritoneal carcinomatosis of colorectal origin. Ann Surg Oncol. 2005;12(1):65–71.
Glehen O, Kwiatkowski F, Sugarbaker PH, Elias D, Levine EA, De Simone M, Barone R, Yonemura Y, Caaliere F, Quente F, Gutman M, Tentes AA, Lorimier G, Bernard JL, Bereder JM, Porcheron J, Gomez-Portilla A, Shen P, Deraco M, Rat P. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol. 2004;22(16):3284–92.
Brücher BL, Bilchik A, Nissan A, Avital I, Stojadinovic A. Tumor response criteria: are they appropriate? Future Oncol. 2012;8(8):903–6.
Stojadinovic A, Bilchik A, Smith D, Eberhardt JS, Ward EB, Nissan A, Johnson EK, Protic M, Peoples GE, Avital I, Steele SR. Clinical decision support and individualized prediction of survival in colon cancer: bayesian belief network model. Ann Surg Oncol. 2013;20:161–74.
Sugarbaker PH. Revised guidelines for second-look surgery in patients with colon and rectal cancer. Clin Transl Oncol. 2010;12(9):621–8.
Sugarbaker P. Second-look surgery for colorectal cancer: revised selection factors and new treatment options for greater success. Int J Surg Oncol. 2011;2011:915078. Epub 2010 Dec 5.
Esquivel J, Sugarbaker PH. Second-look surgery in patients with peritoneal dissemination from appendiceal malignancy: analysis of prognostic factors in 98 patients. Ann Surg. 2001;234(2):198–205.
Elias D, Honoré C, Dumont F, Ducreux M, Boige V, Malka D, Burtin P, Dromain C, Goéré D. Results of systematic second-look surgery plus HIPEC in asymptomatic patients presenting a high risk of developing colorectal peritoneal carcinomatosis. Ann Surg. 2011;254(2):289–93.
Maggiori L, Elias D. Curative treatment of colorectal peritoneal carcinomatosis: current status and future trends. Eur J Surg Oncol. 2010;36(7):599–603.
Wangensteen OH. Cancer of the colon and rectum; with special reference to earlier recognition of alimentary tract malignancy; secondary delayed re-entry of the abdomen in patients exhibiting lymph node involvement; subtotal primary excision of the colon; operation in obstruction. Wis Med J. 1949;48:591–7.
Wangensteen OH, Lewis FJ, Tongen LA. The second look in cancer surgery: a patient with colic cancer and involve lymph nodes negative on the sixth look. J Lancet. 1951;71(8):303–7.
Bleday R, Steele Jr G. Second-look surgery for recurrent colorectal carcinoma: is it worthwhile? Semin Surg Oncol. 1991;7(3):171–6.
Bucci L, Benassai G, Santoro GA. Second look in colorectal surgery. Dis Colon Rectum. 1994;37(2 Suppl):S123–6.
Elias D, Goéré D, Di Pietrantonio D, Boige V, Malka D, Kohneh-Shahri N, Dromain C, Ducreux M. Results of systematic second-look surgery in patients at high risk of developing colorectal peritoneal carcinomatosis. Ann Surg. 2008;247(3):445–50.
Gilbertsen VA, Wangensteen OH. A summary of thirteen years’ experience with the second look program. Surg Gynecol Obstet. 1962;114:438–42.
Grotz RL, Pemberton JH. Second look surgery–a shell game? Am J Gastroenterol. 1992;87(6):804–5.
Lefevre JH, Elias DM. Cytoreductive surgery plus intraperitoneal chemohyperthermia in patients with colorectal cancer at high risk for local-regional recurrence. Cancer J. 2009;15(3):200–3.
Martin Jr EW, James KK, Hurtubise PE, Catalano P, Minton JP. The use of CEA as an early indicator for gastrointestinal tumor recurrence and second-look procedures. Cancer. 1977;39(2):440–6.
Martin Jr EW, Carey LC. Second-look surgery for colorectal cancer. The second time around. Ann Surg. 1991;214(3):321–5; discussion 326–7.
Minton JP, Hoehn JL, Gerber DM, Horsley JS, Connolly DP, Salwan F, Fletcher WS, Cruz Jr AB, Gatchell FG, Oviedo M, et al. Results of a 400-patient carcinoembryonic antigen second-look colorectal cancer study. Cancer. 1985;55(6):1284–90.
Osteen RT, Guyton S, Steele Jr G, Wilson RE. Maligant intestinal obstruction. Surgery. 1980;87:611–5.
Portilla AG, Sugarbaker PH, Chang D. Second-look surgery after cytoreduction and intraperitoneal chemotherapy for peritoneal carcinomatosis from colorectal cancer: analysis of prognostic features. World J Surg. 1999;23(1):23–9.
Ripley RT, Davis JL, Kemp CD, Steinberg SM, Toomey MA, Itzhak A. Prospective randomized trial evaluating mandatory second look surgery with HIPEC and CRS vs. standard of care in patients at high risk of developing colorectal peritoneal metastases. Trials. 2010;11:62.
Rittgers RA, Steele Jr G, Zamcheck N, Loewenstein MS, Sugarbaker PH, Mayer RJ, Lokich JJ, Maltz J, Wilso RE. Transient carcinoembryonic antigen (CEA) elevations following resection of colorectal cancer: a limitation in the use of serial CEA levels as an indicator for second-look surgery. J Natl Cancer Inst. 1978;61(2):315–8.
Santoro BT, Griffen Jr WO, Wangensteen C. The second look procedure in the management of ovarian malignancies and pseudomyxoma peritonei. Surgery. 1961;50:354–8.
Spears H, Petrelli NJ, Herrera L, MItelman A. Treatment of bowel obstruction after operation for colorectal carcinoma. Am J Surg. 1998;155:383–6.
Walsh HPJ, Schofield PF. Is laparotomy for small bowel obstruction justified in patients with previously treated malignancy? Br J Surg. 1984;71:933–5.
Zivanovic O, Barakat RR, Sabbatini PJ, Brown CL, Konner JA, Aghajanian CA, Abu-Rustum NR, Levine DA. Prognostic factors for patients with stage IV epithelial ovarian cancer receiving intraperitoneal chemotherapy after second-look assessment: results of long-term follow-up. Cancer. 2008;112(12):2690–7.
Brücher BLDM, Königsrainer A. Peritonealcarcinose. Chirurgische Allgemeine Zeitung. 2010;11(1):17–31.
Weeks JC, Catalano PJ, Cronin A, Finkelman MD, Mack JW, Keating NL, Schrag D. Patients’ expectations about effects of chemotherapy for advanced cancer. N Engl J Med. 2012;367(17):1616–25.
Sugarbaker PH. Peritonectomy procedures. Ann Surg. 1995;221(1):29–42.
Helm CW, Bristow RE, Kusamura S, Baratti D, Deraco M. Hyperthermic intraperitoneal chemotherapy with and without cytoreductive surgery for epithelial ovarian cancer. J Surg Oncol. 2008;98(4):283–90.
Casado-Adam A, Alderman R, Stuart OA, Chang D, Sugarbaker PH. Gastrointestinal complications in 147 consecutive patients with peritoneal surface malignancy treated by cytoreductive surgery and perioperative intraperitoneal chemotherapy. Int J Surg Oncol. 2011;2011:468698. Epub 2011 Oct 16.
Koea JB, Lanouette N, Paty PB, Guillem JG, Cohen AM. Abdominal wall recurrence after colorectal resection for cancer. Dis Colon Rectum. 2000;43(5):628–32.
Valle M, Federici O, Garofalo A. Patient selection for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy, and role of laparoscopy in diagnosis, staging, and treatment. Surg Oncol Clin N Am. 2012;21(4):515–31.
Bell JC, Rylah BG, Chambers RW, Peet H, Mohamed F, Moran BJ. Perioperative management of patients undergoing cytoreductive surgery combined with heated intraperitoneal chemotherapy for peritoneal surface malignancy: a multi-institutional experience. Ann Surg Oncol. 2012;19:4244–51.
Raspe C, Piso P, Wiesenack C, Bucher M. Anesthetic management in patients undergoing hyperthermic chemotherapy. Curr Opin Anaesthesiol. 2012;25(3):348–55.
Pearse R, Dawson D, Fawcett J, Rhodes A, Grounds RM, Bennett ED. Early goal-directed therapy after major surgery reduces complications and duration of hospital stay. A randomised, controlled trial. Crit Care. 2005;9(6):687–93.
Raval NY, Squara P, Cleman M, Yalamanchili K, Winklmaier M, Burkhoff D. Multicenter evaluation of noninvasive cardiac output measurement by bioreactance technique. J Clin Monit Comput. 2008;22(2):113–9.
Montenij LJ, de Waal EE, Buhre WF. Arterial waveform analysis in anesthesia and critical care. Curr Opin Anaesthesiol. 2011;24(6):651–6.
Sugarbaker PH. Peritonectomy procedures. Ann Surg. 1995;221(1):29–42.
Wallemacq PE, Capron A, Vanbinst R, Boeckmans E, Gillard J, Favier B. Permeability of 13 different gloves to 13 cytotoxic agents under controlled dynamic conditions. Am J Health Syst Pharm. 2006;63(6):547–56.
Peters BG. Technical considerations in the preparation and dispensing of chemotherapy. Top Hosp Pharm Manage. 1995;14(4):78–88.
Stephens AD, Alderman R, Chang D, Edwards GD, Esquivel J, Sebbag G, Steves MA, Sugarbaker PH. Morbidity and mortality analysis of 200 treatments with cytoreductive surgery and hyperthermic intraoperative intraperitoneal chemotherapy using coliseum technique. Ann Surg Oncol. 1999;6:790–6.
Saxena A, Yan TD, Morris DL. A critical evaluation of risk factors for complications after cytoreductive surgery and perioperative intraperitoneal chemotherapy for colorectal peritoneal carcinomatosis. World J Surg. 2010;34:70–8.
Saxena A, Chua TC, Yan TD, Morris DL. Postoperative pancreatic fistula after cytoreductive surgery and perioperative intraperitoneal chemotherapy: incidence, risk, factors, management and clinical sequelae. Ann Surg Oncol. 2010;17(5):1302–10.
Kerscher AG, Mallalieu J, Pitroff A, Kerscher F, Esquivel J. Morbidity and mortality of 109 consecutive cytoreductive procedures with hyperthermic intraperitoneal chemotherapy (HIPEC) performed at a community hospital. World J Surg. 2010;34:62–9.
Glehen O, Osinsky D, Cotte E, Kwiatkowski F, Freyer G, Isaac S, Trillet-Lenoir V, Sayag-Beaujard AC, Francois Y, Vignal J, Gilly FN. Intraperitoneal chemohyperthermia using a closed abdominal procedure and cytoreductive surgery for the treatment of peritoneal carcinomatosis: morbidity and mortality analysis of 216 consecutive procedures. Ann Surg Oncol. 2003;10(8):863–9.
Franko J, Gusani NJ, Holtzman MP, Ahrendt SA, Jones HL, Zeh 3rd HJ, Bartlett DL. Multivisceral resection does not affect morbidity and survival after cytoreductive surgery and chemoperfusion for carcinomatosis from colorectal cancer. Ann Surg Oncol. 2008;15(11):3065–72.
Kusamura S, Younan R, Baratti D, Costanzo P, Favaro M, Gavazzci C, Deraco M. Cytoreductive surgery followed by intraperitoneal hyperthermic perfusion: analysis of morbidity and mortality in 209 peritoneal surface malignancies treated with closed abdomen technique. Cancer. 2006;106(5):1144–53.
Glehen O, Gilly FN, Boutitie F, Bereder JM, Quenet F, Sideris L, Mansvelt B, Lorimier G, Msika S, Elias D, French Surgical Association. Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy: a multi-institutional study of 1,290 patients. Cancer. 2010;116(24):5608–18.
Glehen O, Kwiatkowski F, Sugarbaker PH, Elias D, Levine EA, De Simone M, Barone R, Yonemura Y, Cavaliere F, Quenet F, Gutman M, Tentes AA, Lorimier G, Bernard JL, Bereder JM, Porcheron J, Gomez-Portilla A, Shen P, Deraco M, Rat P. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol. 2004;22(16):3284–92.
Chua TC, Moran BJ, Sugarbaker PH, Levine EA, Glehen O, Gilly FN, Baratti D, Deraco M, Elias D, Sardi A, Liauw W, Yan TD, Barrios P, Gómez Portilla A, de Hingh IH, Ceelen WP, Pelz JO, Piso P, González-Moreno S, Van Der Speeten K, Morris DL. Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. J Clin Oncol. 2012;30(20):2449–56.
McConnell YJ, Mack LA, Francis WP, Ho T, Temple WJ. HIPEC + EPIC versus HIPEC-alone: differences in major complications following cytoreduction surgery for peritoneal malignancy. J Surg Oncol. 2013;107:591–6. doi:10.1002/jso.23276.
Preti V, Chang D, Sugarbaker PH. Pulmonary complications following cytoreductive surgery and perioperative chemotherapy in 147 consecutive patients. Gastroenterol Res Pract. 2012;2012:635314. Epub 2012 Aug 13.
Di Miceli D, Alfieri S, Caprino P, Menghi R, Quero G, Cina C, Pericoli Ridolfini M, Doglietto GB. Complications related to hyperthermia during hyperthermic intraoperative intraperitoneal chemotherapy (HIPEC) treatment. Do they exist? Eur Rev Med Pharmacol Sci. 2012;16(6):737–42.
Glockzin G, von Breitenbuch P, Schlitt HJ, Piso P. Treatment-related morbidity and toxicity of CRS and oxaliplatin-based HIPEC compared to a mitomycin and doxorubicin-based HIPEC protocol in patients with peritoneal carcinomatosis: a matched-pair analysis. J Surg Oncol. 2013;107:574–8. doi:10.1002/jso.23228.
Baratti D, Kusamura S, Mingrone E, Balestra MR, Laterza B, Deraco M. Identification of a subgroup of patients at highest risk for complications after surgical cytoreduction and hyperthermic intraperitoneal chemotherapy. Ann Surg. 2012;256(2):334–41.
Baratti D, Kusamura S, Laterza B, Balestra MR, Deraco M. Early and long-term postoperative management following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. World J Gastrointest Oncol. 2010;2(1):36–43.
Dovern E, de Hingh IH, Verwaal VJ, van Driel WJ, Nienhuijs SW. Hyperthermic intraperitoneal chemotherapy added to the treatment of ovarian cancer. A review of achieved results and complications. Eur J Gynaecol Oncol. 2010;31(3):256–61.
Roviello F, Pinto E, Corso G, Pedrazzani C, Caruso S, Filippeschi M, Petrioli R, Marsili S, Mazzei MA, Marrelli D. Safety and potential benefit of hyperthermic intraperitoneal chemotherapy (HIPEC) in peritoneal carcinomatosis from primary or recurrent ovarian cancer. J Surg Oncol. 2010;102(6):663–70.
Kerscher AG, Mallalieu J, Pitroff A, Kerscher F, Esquivel J. Morbidity and mortality of 109 consecutive cytoreductive procedures with hyperthermic intraperitoneal chemotherapy (HIPEC) performed at a community hospital. World J Surg. 2010;34(1):62–9.
Jaehne J. Cytoreductive procedures-strategies to reduce postoperative morbidity and management of surgical complications with special emphasis on anastomotic leaks. J Surg Oncol. 2009;100(4):302–5.
Glockzin G, Schlitt HJ, Piso P. Peritoneal carcinomatosis: patients selection, perioperative complications and quality of life related to cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. World J Surg Oncol. 2009;7:5.
Younan R, Kusamura S, Baratti D, Cloutier AS, Deraco M. Morbidity, toxicity, and mortality classification systems in the local regional treatment of peritoneal surface malignancy. J Surg Oncol. 2008;98(4):253–7.
Mohamed F, Moran BJ. Morbidity and mortality with cytoreductive surgery and intraperitoneal chemotherapy: the importance of a learning curve. Cancer J. 2009;15(3):196–9.
Chua TC, Yan TD, Smigielski ME, Zhu KJ, Ng KM, Zhao J, Morris DL. Long-term survival in patients with pseudomyxoma peritonei treated with cytoreductive surgery and perioperative intraperitoneal chemotherapy: 10 years of experience from a single institution. Ann Surg Oncol. 2009;16(7):1903–11.
Kusamura S, Baratti D, Hutanu I, Rossi P, Deraco M. The importance of the learning curve and surveillance of surgical performance in peritoneal surface malignancy programs. Surg Oncol Clin N Am. 2012;21(4):559–76.
Kusamura S, Baratti D, Virzì S, Bonomi S, Iusco DR, Grassi A, Hutanu I, Deraco M. Learning curve for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in peritoneal surface malignancies: analysis of two centres. J Surg Oncol. 2013;107:312–9. doi:10.1002/jso.23231.
Kusamura S, Baratti D, Deraco M. Multidimensional analysis of the learning curve for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in peritoneal surface malignancies. Ann Surg. 2012;255(2):348–56.
Burke S, Abu-Wasel B, Eid A, Nissan A, Hanani M. Differential effect of hyperthermia on nerves and smooth muscle of the mouse ileum. J Surg Oncol. 2011;103(1):92–100.
Boutros C, Somasundar P, Espat NJ. Early results on the use of biomaterials as adjuvant to abdominal wall closure following cytoreduction and hyperthermic intraperitoneal chemotherapy. World J Surg Oncol. 2010;8:72.
Acknowledgement
The authors are grateful to Tiffany Felix for her editorial assistance with this collaborative effort.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Additional information
Funding
This work is supported by the Henry M. Jackson Foundation for the Advancement of Military Medicine, INCORE, International Consortium of Research Excellence of the Theodor-Billroth-Academy [TBA®], Germany-Israel-USA and the US Military Cancer Institute.
Disclaimer
The views expressed in this manuscript are those of the authors and do not reflect the official policy of the Department of the Army, the Department of Defense, or the US Government.
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Brücher, B.L.D.M., Itzhak, A., Bilchik, A., Nissan, A., Stojadinovic, A. (2014). Carcinomatosis: Cytoreduction and Heated Intraperitoneal Chemotherapy (HIPEC) Versus Palliation. In: Steele, S.R., Maykel, J.A., Champagne, B.J., Orangio, G.R. (eds) Complexities in Colorectal Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-9022-7_5
Download citation
DOI: https://doi.org/10.1007/978-1-4614-9022-7_5
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-9021-0
Online ISBN: 978-1-4614-9022-7
eBook Packages: MedicineMedicine (R0)