
Abstract
Venous air embolism (VAE) occurs in a patient undergoing a neurosurgical procedure. Mechanism, pathophysiology, signs, and treatment of VAE are discussed as well as preventative measures to decrease the likelihood of such an event from occurring.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Central Venous Pressure
- Pulmonary Blood Flow
- Neurosurgical Procedure
- Hypoxic Pulmonary Vasoconstriction
- Right Atrial Pressure
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
The patient is a 36‐year‐old male who was scheduled to undergo a right occipital-parietal craniotomy for the excision of a small occipital AVM (L-2). He had previously suffered an intraventricular hemorrhage 1 week prior to the scheduled surgery. The patient was otherwise healthy and had nothing remarkable in his past medical history.
An upper extremity 18‐G peripheral IV and 20‐G left radial arterial line were placed prior to taking the patient back to the OR. Following an uneventful, hemodynamically stable induction with fentanyl, vecuronium, and Pentothal, a 9-French left subclavian central venous catheter and a 14‐G lower extremity peripheral IV were placed for additional access. A precordial Doppler (L-5) was also used for monitoring. After the surgeons placed the patient in a reclining, head flexed forward position (L-2), surgery commenced.
Approximately 1.5 h after the surgeons made their initial incision, the rhythmic sound of the precordial Doppler changed slightly (L-4, L-5). Very soon after, the capnograph monitor displayed a sudden drop of etCO2 from 35 to 24 mmHg (L-3, L-4, L-5). The surgical team was immediately notified (L-6, L-7) of the possibility of venous air embolism (L-1). The surgeons immediately packed the area with saline-soaked gauze (L-6, L-7), while the anesthesia team used the central line to draw back bright red frothy blood (L-7). The anesthesia team continued to draw back from the central line until normal venous-appearing blood drew back consistently and easily.
During this time, the patient was also placed in a Trendelenburg position and nitrous oxide was discontinued, and the patient was ventilated with 100 % oxygen (L-8). The patient’s MAP remained relatively stable throughout the episode. Within 5–10 min, the etCO2 returned to baseline. The remainder of the surgery proceeded uneventfully, and the patient was extubated and later discharged without sequelae.
Lessons Learned
L-1: What is a venous air embolism (VAE)? What is the mechanism through which a VAE can occur?
-
A.
VAE is the entrainment of air (either atmospheric or pressurized) from a surgical site into the venous system causing potential hemodynamic and systemic disturbances via the obstruction of pulmonary blood flow.
-
B.
The risk of VAE is present anytime there exists a pressure gradient between the pressure immediately outside an open venous site and the central venous pressure (CVP) or right atrial pressures (RAP). The pressure gradient between the outside and the inside of the vein can occur via one of two ways (Fig. 27.1a, b):
Fig. 27.1 
Venous air embolism can occur in (a) the sitting position due to gravity’s effects on the venous pressure at the open venous site. (b) The supine position where the external pressurized air source provides the pressure gradient for air entry into an open venous site. P i pressure inside vein, P o pressure outside vein
-
1.
Gravitational effects – When the site of the open vein is higher than the right atrium, there exists a relative negative pressure with respect to the RAP, and the intravascular venous pressure becomes subatmospheric. This negative pressure will cause atmospheric air to be entrained into the open vein.
-
2.
Pressurized air – In laparoscopic or endoscopic procedures, insufflated air or carbon dioxide can enter the venous circulation at open venous sites due to supra‐atmospheric pressures regardless of height differences.
-
3.
As little as 5 cm H2O pressure difference between RAP and the outside of an open vessel can cause a hemodynamically significant VAE.
-
1.

L-2: What neurosurgical procedures and patient positions are associated with an increased risk of VAE?
-
A.
Historically, neurosurgical procedures, and specifically surgeries of the posterior fossa in any position and those performed in the sitting position, have been known to have the highest incidence of intraoperative VAE. The large dural sinuses within the cranial vault are incompressible and are thus common sites that air can enter the venous system.
-
B.
Other procedures with reported VAE include spine surgeries, neck surgeries, total hip arthroplasty, cesarean delivery, and liver surgeries.
-
C.
Nonsurgical procedures such as placement of central venous catheters have the potential for VAE to occur.
L-3: What is the pathophysiology of a VAE?
-
A.
The factors that determine the severity of morbidity and mortality have to do with the volume and rate of air accumulation as well as the location of the entrainment:
-
1.
Reported lethal volumes of air have been reported from 200 to 500 cc, or 3–5 cc/kg, and it has been postulated that smaller volumes of air are more lethal when entrained in venous openings that are closer to the heart.
-
2.
For reference, a 5-cm H2O pressure difference across a 14-G catheter can transmit 100-cc air/s.
-
1.
-
B.
Hemodynamics – As stated above, the obstruction of pulmonary blood flow from a VAE can have significant hemodynamic effects:
-
1.
With smaller volumes, entrained air can deposit in the pulmonary circulation, causing obstruction in the pulmonary arterial bed. Neutrophil accumulation and release of vasoactive substances occur, resulting in pulmonary vasoconstriction which can affect right ventricular function and lead to hypotension.
-
2.
Larger volumes of air can produce an “air lock,” which can cause immediate hemodynamic collapse secondary to the inability of the right heart to compress against the large air bubble trapped in the right heart. This can present as pulseless electrical activity as a result of total obstruction of right ventricular ejection in the face of preserved electrical cardiac activity.
-
1.
-
C.
Pulmonary – Hypoxia/hypoxemia is a hallmark of VAE and occurs through a variety of mechanisms (Fig. 27.2):
Fig. 27.2 
Mechanisms of hypoxemia during embolism. CAP PERM capillary permeability, AV arteriovenous, HPV hypoxic pulmonary vasoconstriction, PA pulmonary artery, FRC functional residual capacity, CC closing capacity (Adapted from Benumof JL. Anesthesia for thoracic surgery. 2nd ed. Philadelphia: Saunders; 1995)
-
1.
Decreased cardiac output – Occurs as a result of obstruction to pulmonary flow.
-
2.
Hypoventilation – Air bubbles trapped in the alveolar‐capillary interface serve as a barrier preventing gas exchange. The physiologic dead space increases and leads to a relative hypoventilation and an increase in PaCO2.
-
3.
Decreased hypoxic pulmonary vasoconstriction (HPV) – A VAE that has travelled into the pulmonary circulation will cause an increase in PA pressures and will lead to decreased HPV and increase intrapulmonary shunting.
-
4.
Decreased functional residual capacity:
-
(a)
Bronchoconstriction is also known to occur as a result of platelet activation and the release of vasoactive mediators in the setting of VAE.
-
(b)
Increased pulmonary interstitial edema leads to decreased FRC and will occur via two ways: (1) Serotonin released from activated platelets trapped behind the obstructing air in the pulmonary circulation can increase pulmonary capillary permeability. Increased pulmonary capillary permeability will lead to increased pulmonary interstitial edema. (2) Pulmonary hypertension induced by the obstructing air will also cause increased pulmonary interstitial edema.
-
(c)
The decreases in lung volume will predispose the patient to hypoxemia as a result of atelectatic lung units.
-
(a)
-
1.
-
D.
Neurological – Whereas it has been established that up to 35 % of the population has a patent foramen ovale (PFO), paradoxical air emboli are a major concern in the setting of VAE. As stated above, VAE will cause an obstruction to right ventricular outflow, thereby increasing right heart pressures. This relative increase in right-sided pressures will create a right-to-left shunting across the PFO, and air emboli can bypass the pulmonary circulation and enter the systemic circulation. Focal neurological defects and myocardial ischemia can result from even small amounts of air.

L-4: What are the presenting signs of a VAE?
-
A.
Cardiovascular – Increased right heart strain may lead to EKG changes. Tachyarrhythmias are also common. Pulmonary artery pressures are increased and cardiac output is decreased. Depending on the amount and rate of air entrained, hypotension can range from mild to complete hemodynamic collapse.
-
B.
Pulmonary – Awake patients may complain of coughing, breathlessness, chest pain, and a sense of “impending doom.” Pulmonary rales and wheezing may also be present. With respiratory monitoring, decreases in oxygen saturation and PaO2 are common.
An acute drop in etCO2 is a sensitive sign of VAE. PaCO2 may increase subacutely as a result of relative hypoventilation. The decrease in PaO2 and PETCO2 and increase in PaCO2 is the result of blockage of the pulmonary circulation and concomitant increase in dead space ventilation seen with VAE.
L-5: What are the most sensitive methods to detect a VAE? What are the limitations in each of these methods?
See Table 27.1 for further information.
L-6: What precautionary measures should be taken in procedures where VAE is a significant risk?
-
A.
The anesthesiologist must make an assessment of VAE risk as a function of the specific procedure and positioning for the procedure.
-
B.
Monitoring should be adjusted accordingly. While all anesthetic procedures necessitate the use of pulse oximetry and capnograph monitoring, the anesthesiologist must determine if the placement of a central line for aspiration of air (see below), precordial Doppler, or TEE is appropriate based on VAE risk.
-
C.
Patients should be well hydrated so as to increase CVP to its maximal safest value. An increased CVP will reduce the VAE risk by creating less of a pressure gradient between the pressure outside and inside any open bleeding site (Fig. 27.1).
-
D.
Positioning – While the head-up position carries a higher risk for VAE, it may be prudent to adjust the patient in a flexed leg-up position so as to increase central venous pressure.
-
E.
Regarding the use of PEEP, previously it was thought that using PEEP may help in preventing the incidence of VAE, but studies show that in the seated position, central venous pressure is not augmented enough by PEEP to offset the negative pressure gradient. Additionally, excessive PEEP may compromise hemodynamics (see Fig. 54.3) and the increase in right heart pressures may increase the risk of paradoxical emboli across a PFO. Currently, the data for the use of PEEP in procedures where there is a risk of VAE is mixed.
L-7: What is the treatment of VAE?
-
A.
The first step in treatment is recognizing that VAE has occurred. Depending on monitors being utilized, TEE, precordial Doppler, and capnograph values can all be used to aid in diagnosis of VAE.
-
B.
Once VAE is diagnosed, goals of management include:
-
1.
Prevention of further air entrainment – Surgeons should be notified when there is suspicion of VAE and immediately cover the surgical site with saline and saline-soaked gauze to prevent further air entrainment. If possible, the positioning of the table should be altered so that the bleeding site is below the level of the heart, thereby eliminating the negative pressure gradient. Placing the patient in the left lateral decubitus position, also known as the Durant maneuver, may reduce the effects of an air lock and relieve right ventricular obstruction and allow hemodynamic flow. In cranial procedures, bilateral external jugular compression can reduce the negative pressure gradient by increasing the venous pressure at the entrainment site and also help the surgeon to identify the site of bleeding from open dural sinuses:
-
(a)
Caution should be taken when performing external jugular compression as the prevention of venous drainage may lead to increase intracranial pressure – which may be even more detrimental in certain clinical settings.
-
(b)
Additionally, accidental compression of carotid arteries may lead to ischemia from lack of cerebral perfusion.
-
(a)
-
2.
Aspiration of air – In cases where there is high risk for VAE, placement of a multi‐orifice central venous catheter may be warranted, not only for hemodynamic purposes but also to aspirate air from the right atrium in the setting of VAE. Appropriate placement of a multi‐orifice catheter may be technically difficult and is commonly done through the use of X‐ray, or TEE, or an ECG lead that is attached to the catheter tip. The ideal position is 2 cm distal to the superior vena cava‐right atrial junction, where one would find a biphasic P wave on ECG (Fig. 27.3). Although the data are mixed, aspiration of 15–20 cc of air has been shown to improve outcomes in VAE.
Fig. 27.3 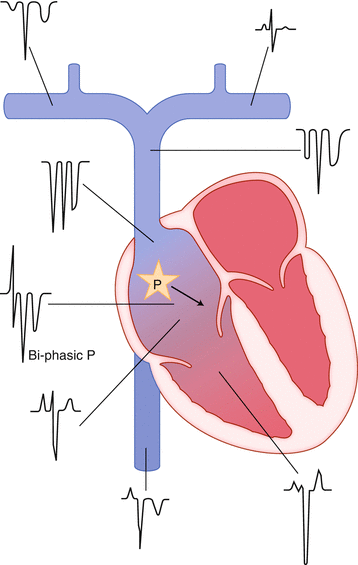
ECG configurations observed at various locations when a central venous catheter is used as an intravascular ECG electrode. The configurations are observed when lead II is monitored and the positive electrode is connected to the catheter. “P” indicates the sinoatrial (SA) node. The heavy black arrow indicates the P wave vector. Note the biphasic P wave when the catheter tip is in the mid-atrial position (Adapted from Miller RD, Eriksson LI, Fleisher L, Wiener-Kronish JP, editors. Miller’s anesthesia: expert consult. 7th ed. Philadelphia: Churchill Livingstone; 2009)
-
3.
Hemodynamic support – Because of the hemodynamic disturbances that can occur in VAE, it is important that the anesthesiologist is prepared to support the patient hemodynamically. Inotropic support for the right ventricle should be readily available and resuscitation measures should be taken if hemodynamic collapse occurs. Even in a non‐code setting, hemodynamic support can improve outcomes. Closed chest massage can help air locks migrate distally into smaller pulmonary vessels, allowing forward pulmonary blood flow in the larger vessels. 100 % oxygen should be instituted to improve oxygen delivery. There are also studies showing that hyperbaric oxygen may improve outcomes.
-
1.

L-8: Why is nitrous oxide detrimental in the setting of VAE?
-
A.
Although nitrous oxide does not increase the incidence of VAE, it increases the size of the airspace and should be discontinued once VAE is recognized, and the patient should be placed on 100 % oxygen.
-
B.
Nitrous oxide is 34 times more soluble in blood than nitrogen and therefore nitrogen will leave the airspace to go into the blood relatively slowly. Thus, the efflux of nitrogen gas out of an air space is much slower than the influx of nitrous oxide into an airspace. Therefore, the airspace will increase in size.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Rangwala, Z. (2014). Venous Air Embolism During Arteriovenous Malformation Repair. In: Benumof, J. (eds) Clinical Anesthesiology. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8696-1_27
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8696-1_27
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8695-4
Online ISBN: 978-1-4614-8696-1
eBook Packages: MedicineMedicine (R0)