
Abstract
-
Of patients with newly diagnosed colorectal cancer who will undergo surgery with curative intent as part of their treatment, approximately 5–12 % will have tumors that have spread beyond the anatomic landmarks of a standard resection and have invaded adjacent organs or structures. The goal of surgery in such cases is a wide en bloc resection of the tumor and any involved adjacent organ or structure.
-
Of patients who undergo resection with curative intent and receive adjuvant therapy, between 7 and 33 % develop isolated local or regional recurrences. In up to 20 % of these recurrences, resection (metastectomy) can be curative.
-
The most important factor that influences tumor recurrence is the stage of disease at presentation.
-
Other factors include obstruction or perforation at presentation, adjacent organ involvement, tumor aneuploidy, increased tumor grade, mucin production, or evidence of venous or perineural invasion.
-
The preoperative evaluation, operative approach, and often the perioperative oncologic therapy are similar for primary locally advanced and recurrent rectal cancer.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Rectal Cancer
- Multimodality Therapy
- Advanced Rectal Cancer
- Preoperative Chemoradiation
- Recurrent Rectal Cancer
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
-
Of patients with newly diagnosed colorectal cancer who will undergo surgery with curative intent as part of their treatment, approximately 5–12 % will have tumors that have spread beyond the anatomic landmarks of a standard resection and have invaded adjacent organs or structures. The goal of surgery in such cases is a wide en bloc resection of the tumor and any involved adjacent organ or structure.
-
Of patients who undergo resection with curative intent and receive adjuvant therapy, between 7 and 33 % develop isolated local or regional recurrences. In up to 20 % of these recurrences, resection (metastectomy) can be curative.
-
The most important factor that influences tumor recurrence is the stage of disease at presentation.
-
Other factors include obstruction or perforation at presentation, adjacent organ involvement, tumor aneuploidy, increased tumor grade, mucin production, or evidence of venous or perineural invasion.
-
The preoperative evaluation, operative approach, and often the perioperative oncologic therapy are similar for primary locally advanced and recurrent rectal cancer.
-
Locally advanced primary rectal cancers include tumors that are T4 N1-2 MX at the time of initial presentation. They are often associated with a higher rate of metastatic disease at the time of diagnosis and have a poorer overall prognosis than earlier stage disease.
-
T4 rectal tumors are found to be fixed by physical examination or to be invading adjacent organs or structures by diagnostic imaging studies.
-
In cases where an extended en bloc resection cannot be performed to achieve complete resection, patient survival is dismal: after no treatment or after palliative surgery, mean survival time is less than 1 year.
-
Multimodality therapy incorporating radiation, chemotherapy, and surgery should be used to achieve local tumor control and to prevent or control systemic tumor dissemination, thereby improving patient survival for patients with locally advanced primary or recurrent colorectal cancers.
-
To achieve these goals, appropriate surgery is combined with external-beam radiation (EBRT) and, under ideal circumstances, intraoperative radiation therapy (IORT) and adjuvant or neoadjuvant chemotherapy.
-
Survival with an isolated, untreated, locoregional, rectal cancer recurrence is quite poor. Most of these patients develop disabling complications, including severe pain from bony or nervous tissue involvement, urinary obstruction, fecal obstruction or incontinence, or persistent bleeding.
-
Nearly 90 % of rectal cancer recurrences after surgery alone occur in the central or posterior pelvis, and 19 % occur at the anastomosis.
-
Stage T4 primary tumors are significantly associated with relapse in the anterior pelvic region.
-
External-beam radiation alone or combined with systemic chemotherapy may result in temporary improvement of symptoms, but the 5-year survival rate is less than 5 %. For these patients, length of survival is perhaps less important than quality of life.
-
A patient who presents with a locally advanced primary or recurrent rectal cancer must be thoroughly evaluated for the presence of extrapelvic disease.
-
If extensive extrapelvic disease is found, the degree and scope of surgical resection should be changed from one of curative intent to palliation.
-
Whether a patient is a candidate for surgery is influenced by a number of factors, including the patient’s overall physical condition and comorbid diseases and the extent of spread and fixation of the tumor outside of the rectum.
Preoperative Evaluation and Patient Selection
-
Complete resection of a locally advanced primary or recurrent rectal cancer is a significant undertaking.
-
Complete resection may be technically possible in some patients, but if their overall physical condition does not make them an appropriate candidate, surgical palliation combined with chemoradiation is the more prudent course of action.
-
Patients who are in poor health, or who will not be able to tolerate multimodality therapy combined with complete surgical resection, or have an ASA classifications of IV–V are not considered acceptable surgical candidates.
-
Nearly as important as their physical condition is consideration of the patient’s motivation and emotional preparedness for undergoing this extensive treatment.
-
If the patient is deemed an acceptable candidate for surgery, the next step is evaluation for the extent of local spread and the possibility of extrapelvic spread.
-
A thorough physical exam, with particular attention placed on the rectal and vaginal exam, needs to be performed, and any fixation of the tumor to rigid pelvic structures needs to be assessed.
-
Imaging should be repeated before surgery is considered and compared to similar previous studies to give some reassurance that there has been no progression or spread of the disease that might change or preclude any surgical intervention.
-
The abdomen and pelvis need to be evaluated with a double-contrast (intravenous and oral) computed tomography (CT) scan to exclude extrapelvic spread and to assess the extent of possible resection.
-
CT scans are generally reliable for identifying the extent of disease and adjacent organ involvement but are less discriminating for predicting local tumor resectability.
-
Any worrisome lesion that is technically accessible should be biopsied percutaneously.
-
Although the above tests are the standard evaluation for diagnosing recurrence and excluding extrapelvic spread of the tumor, other more tumor-specific tests have been proposed as adjuncts.
-
Numerous nonrandomized studies have shown that FDG-PET imaging for recurrent colorectal cancer has a significantly higher sensitivity and specificity than CT scanning. When CT scanning was compared with FDG-PET imaging in postoperative patients with colorectal locoregional recurrences, the sensitivity of FDG-PET was significantly higher than CT plus colonoscopy (90 vs. 71 %, respectively), although the specificities were similar (92 vs. 85 %, respectively).
-
FDG-PET imaging has been shown to maintain this high sensitivity and specificity, 84 and 88 %, respectively, even in the setting of the previously irradiated and postoperative pelvis.
-
Thus, FDG-PET might be a useful tool in the postoperative patient in whom there is a suspicion of recurrence but equivocal CT findings, and in whom extensive reoperative surgery might be of extremely high risk.
-
Even the combination of physical examination and radiographic studies may not be able to prove that there is a pelvic recurrence of a rectal cancer, especially if the patient has undergone a previous pelvic operation or pelvic irradiation. We generally accept three ways of differentiating postoperative changes from tumor. The first is to document a change in the lesion, such as increase in size over time; the second is invasion of the adjacent organs; the third is histological evidence obtained from endoscopic, CT-, or ultrasound-guided biopsies of the suspicious tissue.
-
Exploratory pelvic surgery should be strongly discouraged, as it poses an extreme risk to the patient and makes future evaluation of the pelvis even more difficult.
Determining Tumor Resectability
-
Locally advanced primary or locoregional recurrences of rectal cancers can extend to involve any of the pelvic organs or rigid bony structures of the pelvis. Resectability is based upon the anatomic location and what other structures are fixed to the lesion.
-
Although there are other schemes for assessing resectability, we use the following one to classify our patients who are being considered for possible resection. The tumor is classified as F0 when it is not fixed to any pelvic organ or structure, FR when the tumor is fixed but resectable, and FNR when the tumor is fixed and not resectable.
-
FR is further subdivided by noting the anatomical extent of the fixation (anterior, posterior, and lateral). The anatomic extent of the tumor determines the scope of the required resection.
-
For example, anterior fixed lesions may require a hysterectomy, vaginectomy, a partial or complete cystectomy, or prostatectomy, whereas lesions that are fixed posteriorly may require a sacrectomy (Figs. 45.1, 45.2, and 45.3).
Fig. 45.1 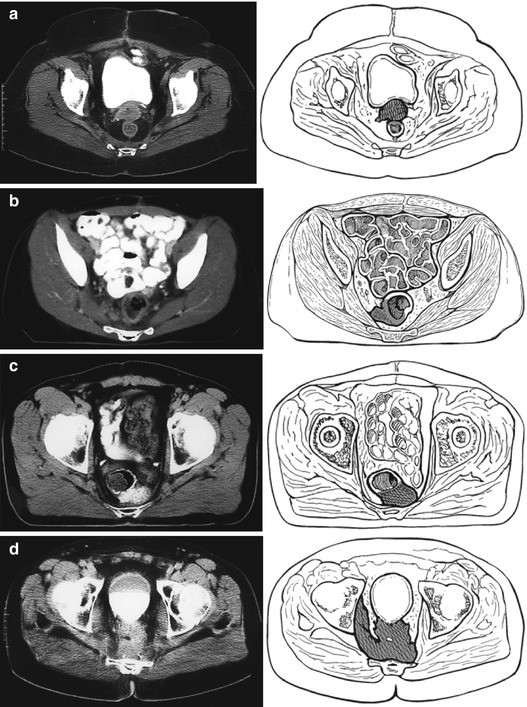
(a) A primary T3N0M0 rectal cancer treated with a lower anterior resection without adjuvant therapy. The anterior recurrent tumor fixed at the base of the bladder was treated with preoperative chemoradiation and then resected with IORT. (b) After a primary low anterior resection for T2N0M0 rectal cancer without adjuvant therapy, this patient developed a lateral pelvic recurrence. After preoperative chemoradiation, the patient underwent an abdominal resection with negative margins. (c) A recurrence after a T3N0M0 lesion treated with postoperative chemoradiation therapy was found to invade the sacrum. After additional EBRT and chemotherapy, IORT combined with an en bloc resection of the tumor and distal sacrum was performed with negative margins. (d) A massive recurrent cancer found in the pelvis after an abdominal perineal resection and postoperative chemoradiation. The tumor was fixed to vital pelvic structures and was deemed unresectable (With permission from Nicholls RJ, Dozois RR, editors. Surgery of the colon and rectum. New York: Churchill Livingston; 1997)
Fig. 45.2 
The IORT suite, showing the equipment, the position of the patient on the operating room table, and the linear accelerator
Fig. 45.3 

(a) The assortment of the Lucite tubes used to direct the electron beam to a fixed site in the operating field to deliver the IOT. (b) Place of a large Lucite tube to deliver the IORT into the pelvis. The tube is fixed in place by securing it to an external support apparatus attached to the operating table
-
Although we have found this classification scheme to be extremely useful, it does not reliably predict resectability before surgery because new findings may be discovered at operation.
-
However, in our experience, some factors are clearly associated with an unresectable tumor (Table 45.1).
Table 45.1 Symptoms or findings suggestive of an unresectable tumor for cure -
Any circumferential tumor that extends to the pelvic sidewall is considered unresectable.
-
Evidence of bilateral ureteral obstruction is a very worrisome finding. Unless there is focal infiltration of the bladder trigone causing bilateral ureteral obstruction, this finding usually indicates that a bulky tumor has invaded both lateral pelvic sidewalls.
-
Finally, S1 and S2 nerve root involvement or evidence of invasion of the sacral bone at the level of S1 and S2 indicates an unresectable tumor.
-
Pain from nerve root involvement with tumor occasionally needs to be differentiated from sciatic nerve compression. Nerve compression symptoms may completely resolve after pelvic irradiation and chemotherapy. On the other hand, persistent buttock and perineal pain usually resulting from tumor expansion and ingrowth is a more ominous symptom.




Multimodality Therapy for Advanced or Locally Recurrent Rectal Cancer
-
Surgery with curative intent is the mainstay of treatment for advanced or locally recurrent rectal cancer. However, surgery alone results in a high rate of local and distant failure.
-
To improve outcomes, surgery is combined with multimodality therapy, radiation, and chemotherapy. Radiotherapy is used to improve local control and systemic chemotherapy is used to treat possible disseminated disease.
-
In the setting of a locally advanced or recurrent rectal cancer, centers have combined multimodality therapy with intraoperative radiotherapy – either as electron-beam radiation therapy, high-dose rate brachytherapy, or traditional perioperative brachytherapy to further improve patient outcomes.
-
These forms of locally directed radiation reduce toxicity by limiting normal tissue exposure and deliver a high biologically equivalent dose to the localized area of the tumor.
-
In general, patients who never received prior pelvic radiation therapy, a full course of external-beam radiation (5,040 cGy) is administered with concurrent 5-fluorouracil chemotherapy.
-
Often, patients with recurrent rectal cancer have previously received a full course of pelvic external-beam radiation.
-
Such patients can be treated with an additional course of 2,000 cGy of external-beam radiation combined with additional 5-fluorouracil chemotherapy before repeating pelvic surgery.
-
A recent multicenter study has shown that hyperfractionated preoperative chemoradiation can be safely administered in recurrent rectal cancer patients who have previously received pelvic radiation. The overall tumor response rate was 44.1 %. Furthermore, there was no increase in postoperative complications as compared to patients who did not receive the hyperfractionated therapy.
Surgery
-
Before surgery, the magnitude of the operation and the possible complications are discussed in depth with the patient and family members.
-
In cases of large locally advanced primary rectal cancers, the sphincter mechanism is preserved. In recurrent cancers, there is little role for an attempt at sphincter preservation, as the risk of complications or poor functional outcomes is quite high.
-
In addition, the resection of adjacent structures or organs and the functional implications and reconstruction alternatives, such as an ileal conduit, need to be discussed. All patients visit with and are marked for multiple ostomies by an enterostomal therapist.
-
In the OR, the patient is placed in the lithotomy position with both arms tucked and the legs supported in Allen stirrups. Special care is taken to ensure that the arms are well padded and in a neutral position to avoid any nerve injury. The calves are positioned and padded to avoid any pressure from directly resting on the stirrups, since the lengthy operation may result in compartment syndrome and/or venous thrombosis.
-
Bilateral ureteral stents are inserted cystoscopically preoperatively in all patients.
-
A midline incision is usually made. Transverse abdominal incisions should be avoided, as they compromise the placement of any stomas and may injure the inferior epigastric vessels, the primary blood supply of the rectus muscle.
-
Preservation of the rectus muscle is important in case a transpelvic rectus abdominis flap is required to reconstruct the pelvic floor.
-
If the patient has had prior abdominal surgery, all adhesions need to be lysed.
-
Once all adhesions have been lysed, the entire abdomen needs to be thoroughly explored for evidence of extrapelvic tumor deposits.
-
The liver, omentum, retroperitoneum, peritoneal lining, and the area of any prior surgical incision should be carefully examined for metastatic disease.
-
Any suspicious finding should be biopsied and analyzed by frozen section. The presence of extrapelvic disease would be a contraindication to radical resection.
-
For rectal cancer recurrences that are not fixed to any pelvic structure (F0), a completion abdominoperineal resection (APR) is required. The scope of the resection is similar to a standard APR, but the pelvic fibrosis induced by any prior surgery would have distorted or eliminated the ideal, relatively bloodless plane between the mesorectum and sacral fascia.
-
The distinction between fibrosis and tumor infiltration into adjacent tissue can be very difficult to discern at the time of the operation. If there is any question a frozen section should be analyzed. If tumor cells are seen, a complete resection with negative margins is not feasible. It is in this setting that the use of IORT improves clinical outcomes.
-
When the tumor is fixed, either anteriorly or posteriorly, the scope of the operation is much larger than for the nonfixed lesion (F0).
-
If the fixed tumor is considered resectable, we classify it as a FR (fixed, resectable) lesion. For anteriorly fixed tumors, there are different operations that need to be considered, whereas for a primary or recurrent posteriorly fixed tumor, our operation of choice is an en bloc distal sacrectomy.
-
Postoperatively, these patients are managed quite conservatively as prolonged ileus and urinary retention is quite common. Given the high risk of venous thromboembolism, these patients are given unfractionated heparin three times a day, and use of mechanical compression devices and mandatory early ambulation are enforced.
Use of Intraoperative Radiation Therapy
-
In cases of close margins, known microscopically positive margins, or minimal gross unresectable disease in the pelvis or after the sacrectomy, an option is to use intraoperative electron-beam radiation therapy (IORT).
-
To give IORT, a Lucite cylinder is positioned in the pelvis to target the at-risk area. The patient is then positioned under the linear accelerator. One thousand to 2,000 cGy is delivered, depending on the extent of margin involvement.
-
A dose of 1,000 cGy is recommended for minimal residual disease; 1,500 cGy is given for gross residual disease less than 2 cm, and 2,000 cGy is reserved for unresectable or gross residual disease more than 2 cm. The IORT dose that can be given should take into account the total of any prior external-beam radiation that has been administered.
-
Other options exist of delivering intraoperative or prolonged local radiation therapy. One combined-modality treatment protocol uses high-dose intraoperative brachytherapy (HDR-IORT). The radiation is delivered via an array of catheters that are imbedded in a flexible rubber pad or vinyl mesh. This is then sutured to the area of concern and other normal tissues are packed away and protected. The catheters are connected to a high-dose rate Ir source, either intraoperatively or postoperatively.
-
These techniques do not require a dedicated OR with a linear accelerator to administer radiation regionally and may therefore expand where this type of surgery can be performed.
-
One possible disadvantage with the use of more standard postoperative brachytherapy catheters is that it is difficult to protect normal tissue, particularly the small intestine, once the operation is complete. However, these alternative methods for delivering local radiation therapy, when combined with extended surgery and chemotherapy, seem to result in morbidity and survival outcomes that are comparable to the experience with intraoperative electron-beam radiation therapy.
Results of Multimodality Treatment for Advanced Primary or Locally Recurrent Rectal Cancer
-
For patients with advanced primary rectal cancer, studies have shown the benefit of combined preoperative chemoradiation followed by radical surgery.
-
In a retrospective review of 60 patients with primary locally advanced rectal cancers, 81 % were able to undergo curative resection. Their overall 2-year survival was 91 %, and their local regional recurrence rate was 7.5 %.
-
In another study, preoperative chemoradiation with extensive surgery improved overall survival and control of pelvic disease compared to preoperative radiation therapy alone. In that study, the use of IORT improved local control in patients with microscopic residual disease or clinically fixed tumors. None of the patients treated with IORT developed local failure in the pelvis.
-
In summary, a number of reports of patients with locally advanced primary rectal cancer who were treated with intraoperative radiation and surgery have shown an overall improvement in local control compared to historical controls.
-
Surgery alone has been used to treat recurrent rectal cancers. Garcia-Aguilar and colleagues reported a series of 87 patients with recurrent rectal cancer:
-
Sixty-four patients underwent surgical exploration, and only 42 were able to undergo resection with curative intent. The estimated 5-year survival rate for patients who had curative-intent surgery was significantly better than that for patients who had only palliative or no surgery (35 vs. 7 %). In most series, recurrence and survival rates for patients with recurrent rectal cancer treated with surgery alone are less than those for patients with primary advanced rectal cancer but are still better than historical data for patients treated with palliative therapies. In general, patients treated with multimodality therapy including preoperative or intraoperative radiation therapy experience 3-year local control rates ranging from 25 to 78 %, and long-term survival has been reported to be between 25 and 40 %. The most consistent findings from all of these reports are that the most predictive factor associated with a better outcome, decreased local recurrence, cancer-specific, and overall survival is an R0 resection. The presence of microscopic positive or grossly positive margins markedly reduces survival.
-
-
The institution with the largest reported experience using multimodality therapy including IORT for recurrent rectal cancer is the Mayo Clinic. Between 1981 and 1996, 394 patients were treated, 90 of whom had unresectable local or extrapelvic disease at the time of surgical exploration. Although 304 patients underwent resection of the recurrent tumor, only 138 (45 %) underwent a histologically confirmed curative resection:
-
The 166 remaining patients had a palliative operation because of either gross (n = 139) or microscopic (n = 27) residual cancer in the pelvis.
-
The 1-year, 3-year, and 5-year survival rates for the 304 patients were 84, 43, and 25 %. The median survival time was 31 months.
-
The 5-year survival rate was greater after curative surgery (i.e., negative histologic margins) than after palliative surgery (37 vs. 16 %, P < 0.001). The presence of gross residual disease in patients who underwent nonpalliative resections resulted in decreased survival compared to those patients with microscopic residual disease.
-
However, survival for patients who had extended resections was not significantly different than that for patients who had a limited resection (28 vs. 21 %, P = 0.11, respectively). Logistic regression analysis found several independent factors that contributed to the ability to perform a curative resection. On multivariate analysis, increasing number of tumor fixation sites was associated with a palliative resection. These factors also affected overall survival; patients with pain and more than one site of fixation had significantly lower survival rates.
-
The best 5-year survival rates were in patients who had nonfixed tumors (41 %) or asymptomatic recurrences (41 %).
-
-
Other institutions that have used a multimodality approach that included some form of intraoperative radiation have reported similar improvements in local recurrence and survival.
-
Perioperatively related mortality was very low in patients who undergo this multimodality treatment (0.3 %). Unfortunately, the treatment-related morbidity is relatively high.
-
In one series of 304 patients who underwent surgery with curative intent, 96 (32 %) required prolonged hospitalizations, 78 (26 %) of whom required readmissions and/or additional surgical procedures.
-
The most frequent complications included pelvic abscesses (6.6 %), bowel obstructions (5.3 %), enteric fistulas (4.3 %), and perineal wound complications (4.6 %).
-
The complication rate was significantly higher in patients who underwent extended surgical resections and in patients who had recurrences fixed in more than two sites in the pelvis. These findings underscore the need for thorough preoperative patient selection to ensure that the patient is fit enough to tolerate the surgery and the potential complications and that there is no evidence of disease outside of the region of resection.
Palliative Care for Advanced or Recurrent Rectal Cancer
-
Patients who present with locally advanced or recurrent rectal cancer must first be evaluated with the intent to cure.
-
An equally important consideration is palliation of symptoms if a cure does not seem to be achievable. The local effect within the pelvis of an advanced or recurrent rectal cancer drives the need to address control of symptoms.
-
These symptoms often include rectal bleeding, rectal obstruction, urinary obstruction due to local invasion, and severe pain related to invasion of the pelvic sidewall or direct invasion of pelvic nerves.
-
Over the past decade, the choice of palliative options has expanded, and the choice of treatment requires careful consideration of the presenting symptoms, possible future symptoms, extent of local and distant spread of the disease, and the overall physical condition of the patient.
-
Palliative interventions may be broadly classified as noninvasive, minimally invasive, and surgical.
-
The primary noninvasive palliative option is radiotherapy. In patients who have never received pelvic radiation, a full course of external-beam irradiation may be a very effective treatment for bleeding, pelvic pain, and near obstruction. The use of external-beam radiotherapy may result in palliation of severe pelvic pain in 50–90 % of patients.
-
However, virtually all patients will experience progression of the tumor and recurrent symptoms before they die.
-
Minimally invasive approaches to palliation usually involve mechanical means to reduce symptoms related to pelvic tumors. These include ureteral stents to alleviate urinary obstruction and expandable metal colonic wall stents or the use of lasers to relieve rectal obstruction. Self-expanding metal stents (SEMS) are useful for the nonsurgical management of rectal obstructions, bleeding, and malignant fistulas. In a review of the literature, palliation with SEMS was achieved in 90 % of patients.
-
In the largest series to report on SEMS for malignant rectal obstructions, stents could be deployed successfully in 36/37 patients with rectal obstructions, and 28 had good long-term results with no need for subsequent intervention.
-
Endoscopic lasers are an alternative to SEMS. The neodymium yttrium argon garnet (Nd:YAG) laser is the most commonly used. Endoscopic laser treatments remove the tissue from the lumen by coagulative necrosis or immediate tissue vaporization, depending on the amount of energy applied.
-
Palliation of symptoms and marked improvement in quality of life is achieved after repeated laser sessions (usually 2–5) in 80–90 % of patients.
-
Unfortunately, laser therapy does not appear to be a durable treatment. Effective palliation declines as patients survive longer; successful palliation at 1 year was only 42 %.
-
There is no data on the use of palliative resections in patients with locally advanced or recurrent rectal cancer. However, a report from Memorial Sloan-Kettering has evaluated the role of palliative resection in 80 patients with stage IV rectal cancer. Twenty-four percent had clinical evidence of obstruction and 94 % had either T3 or T4 lesions. None had received prior surgery or radiation therapy. They underwent radical resection of the primary lesion and surgical treatment of solitary hepatic metastasis, if present.
-
There was one death, a 15 % postoperative morbidity, and a 20 % colostomy rate. The overall local recurrence rate was 6 %, the actuarial local control at 2 years was 94 %, and the median survival was 25 months.
-
This study shows that in appropriately selected patients with stage IV disease and complicated or advanced rectal cancer, surgical resection of the primary tumors can achieve very reasonable oncologic results and provide good palliation of symptoms related to the tumor.
Summary
-
For patients with advanced primary or recurrent rectal cancers, the only hope of cure requires a coordinated multidisciplinary approach to treatment. In general, EBRT, chemotherapy, extensive surgery, and the use of directed IORT appear to improve local control and survival.
-
Surgery in these patients carries a higher morbidity rate than surgery for primary rectal cancer but one that is acceptable in appropriately selected patients. Before proceeding with multimodality therapy, patients should be thoroughly evaluated for the presence of disseminated extrapelvic or metastatic disease, which would, in most instances, preclude a curative operation.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Cima, R.R. (2014). Rectal Cancer: Locally Advanced and Recurrent. In: Beck, D., et al. The ASCRS Manual of Colon and Rectal Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8450-9_45
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8450-9_45
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8449-3
Online ISBN: 978-1-4614-8450-9
eBook Packages: MedicineMedicine (R0)