
Abstract
The knee joint is a hinge joint. It is the largest synovial joint in the body. The main motion in the knee joint is flexion–extension. Mild internal rotation-external rotation and adduction-abduction can occur.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Anatomy of the knee joint
- The meniscus
- Stability of the knee joint
- Normal knee alignment
- Genu varum
- Genu valgum
- Blount disease
- Knee pain in children
- Osgood–schlatter disease
- Sinding–Larsen–Johansson disorder
- Jumper’s knee
- Osteochondritis dissecans
- Patellar instability (Recurrent patellar subluxation and dislocation)
- Popliteal cyst (Baker cyst)
- Patellofemoral pain syndrome
- Fibular hemimelia
- Congential pseudoarthrosis of the tibia
- Bowing of the leg
- Anterolateral bowing
- Posteromedial bowing of the tibia
- Anteromedial bowing of the tibia
Anatomy of the Knee Joint
-
The knee joint is a hinge joint (Fig. 7.1)
Fig. 7.1 
Anatomy of the knee joint
-
The knee joint is a hinge joint
-
■ It is the largest synovial joint in the body.
-
■ The main motion in the knee joint is flexion–extension. Mild internal rotation-external rotation and adduction-abduction can occur.
-
■ The range of motion of the knee is from full extension to about 150° flexion.
-
■ Three bones form of the knee joint (Fig. 7.1):
-
Lower femur.
-
Proximal tibia.
-
Patella:
-
□ The largest sesamoid bone in the body (bone impeded in a tendon)
-
-
-
■ The growth plates (physis) of the distal femur and proximal tibia are:
-
The most active growth plates in the lower extremity
-
□ The distal femur grows about 9 mm/year.
-
□ Proximal tibial grows about 6 mm/year.
-
□ Most of the neoplastic conditions in the lower extremity occur around the knee joint.
-
-
The growth plates are prone to growth disturbance when they are affected by Salter–Harris injuries.
-

The Meniscus
-
■ Two cartilaginous crescent-shaped structures that act like a cushion inside the knee (Fig. 7.2).
Fig. 7.2 
Medial and lateral meniscus
-
■ The meniscus lies on the surface of the tibial plateau, one medial and one lateral.
-
■ The medial meniscus is more prone to injury because it is more fixed to the joint capsule, more likely to be caught in between femur and tibia in case of injury.

Stability of the Knee Joint
-
■ The stability of the knee joint depends on strong ligaments connecting the femur with the tibia and the fibula (Fig. 7.3):
Fig. 7.3 
Ligaments of the knee
-
Anterior cruciate ligament (ACL):
-
□ Extends from the anterior part of the tibia to posterior femoral notch.
-
□ It prevents anterior displacement of the tibia on the femur.
-
□ ACL is prone to sport injuries especially in adolescent females playing sports with cutting movements (e.g., soccer).
-
-
Posterior cruciate ligament (PCL):
-
□ Extends from the posterior surface of the tibia to the anterior part of the femoral notch.
-
□ It prevents posterior displacement of the tibia on the femur.
-
□ PCL is less prone to sports injury than ACL.
-
-
Medial collateral ligament (MCL):
-
□ Extends from the medial femoral epicondyle to the medial aspect of the tibia.
-
□ It consists of two parts: superficial and deep.
-
□ Primary restrain of the knee joint against drifting into valgus (the tibia point laterally)
-
-
Lateral collateral ligament (LCL):
-
□ Extends from lateral femoral epicondyle to the upper end of the fibula.
-
□ Primary restrain of the knee joint against drifting into varus (the tibia points medially).
-
-

How to Examine the Knee Joint
(See the general orthopedic exam in the introduction chapter)
-
■ Inspection:
-
Alignment and deformity
-
Swelling and effusion (Fig. 7.4).
Fig. 7.4 
Effusion of the knee. Note the right knee swelling. The medial side of left knee shows the normal groove (arrow). The medial groove on the right knee had been obliterated due to knee effusion
-
Scars of previous surgery.
-
Color changes.
-
-
■ Palpation:
-
Bony landmark (patella, tibial tuberosity, medial and lateral femoral epicondyles)
-
Tenderness (joint line, patella, distal femur, proximal tibia, posterior knee)
-
-
■ Movement (Range Of Motion (ROM)):
-
Active and passive range of motion.
-
Restriction of movement may be due to contracture or pain.
-
Decreased ROM is a very sensitive indicator of joint inflammation.
-
-
■ Special test
-
Assessment of effusion.
-
□ Disappearance of the groove medial to the patella (Fig. 7.4): this is an early sign of knee effusion.
-
□ Ballottement test (Fig. 7.5)
Fig. 7.5 
Ballottement test. One hand squeezes the suprapatellar pouch to push the fluid underneath the patella. The index of other hand presses the patella downward. Feeling the patella “float” in the effusion is a positive sign
-
-
Assessment of meniscal pathology:
-
□ Apley Grinding test (Fig. 7.6).
Fig. 7.6 
Apley grinding test. The patient is positioned prone with the hip extended and knee flexed. The examiner holds the foot moving the leg internally (a) and externally (b) while pushing it down against the femur. If there is meniscal tear, the patient will feel pain
-
□ McMurray test: (Fig. 7.7).
Fig. 7.7 
McMurray test: (a) The knee is flexed with one hand holding the knee at the joint line and the other hand holding the foot. The knee is put in the position of valgus external rotation. (b) The knee is gradually extended with the leg kept in the position of valgus external rotation. Pain or a “click” constitutes a positive McMurray test for tear in the medial meniscus. (c and d) The same test is performed with leg in the position of internal rotation and varus. Click or pain is a positive test for lateral meniscus tear
-
-
Other tests for assessment of stability of the knee (see Chap. 10).
-




Normal Knee Alignment
-
■ The knee joint is in varus until 2 years of age (Fig. 7.8).
Fig. 7.8 
Normal alignment of the knee. The knee joint is in varus at 2 years of age then reaches maximum valgus around the age of 3 years and then normal adult alignment by the age 8 years
-
■ The alignment of the knee changes to valgus which reach maximum around the age of 3 years.
-
■ The normal adult alignment (7 degrees of valgus) is usually reached by the age 8 years.
-
■ Clinical Method of assessment of knee alignment:
-
The intercondylar distance (Fig. 7.9):
Fig. 7.9 
(a) Intermalleolar distance. This distance is increased in cases of genu varum (b) Intercondylar distance: this increases in cases of genu varum. (c) 3-year-old boy with genu varum and intercondylar distance of more than hand breadth
-
□ Intercondylar distance of more than hand breadth is an indication for genu varum.
-
-
The intermalleolar distance (Fig. 7.9):
-
□ The intermalleolar distance of more than hand breadth is an indication genu valgum.
-
-
The clinical thigh-leg angle (Fig. 7.10)
Fig. 7.10 
Physiological genu valgum. 30-month-old boy with physiological genu valgum. Notice the increased angle between the leg and the thigh dotted lines and the increased intermalleolar distance (double headed arrow)
-



Genu Varum (Bow Leg)
Definition:
-
■ Deformity of the knee in which the lower leg is pointing medially (see Introduction chapter) (Figs. 7.8, and 7.9).
-
■ The child will have an increase in the intercondylar distance of more than one hand breadth.
-
■ Can be normal development until 2 years of age.
Common cause of genu varum:
Table 7.1: cause of genu varum.
Imaging:
Indication for plain radiographs in cases of genu varum:
-
■ Persistence of genu varum after 24 months.
-
■ Worsening genu varum after the age 1 year.
-
■ Unilateral genu varum.
-
■ Severe genu varum (clinical angle between thigh and leg of more than 20° or intercondylar distance of more than 6 cm).
-
■ Associated deformities of the other joints.
-
■ If suspecting general medical condition (e.g., rickets).
Genu Valgum (Knock Knee)
Definition:
-
■ Deformity of the knee in which the lower leg is pointing laterally (Fig. 7.8 and 7.10).
-
■ Genu valgum is a normal finding in children around 3 years of age (physiological genu valgum).
-
■ The condition usually improves gradually to reach the adult alignment by 8 years of age (7° valgus angle between the femur and the tibia).
Causes of genu valgum:
-
■ Physiologic genu valgum (Fig. 7.10).
-
■ Rickets and renal osteodystrophy.
-
■ Posttraumatic physeal arrest.
-
■ Proximal tibial fractures:
-
Proximal tibial fracture can result in genu valgum few months after the injury due to abnormal growth of the proximal tibial physis (Kozin fracture).
-
-
■ Tumor of the proximal tibia.
-
■ Infection of the proximal tibia.
-
■ Dysplasia (e.g., Multiple epiphyseal dysplasia)
Physiological genu valgum:
-
Part of the normal development of children (Fig. 7.10).
-
Reaches maximum around at the age of 3 years and then improve with time to reach normal alignment by the age of 8 years.
-
Clinical presentation:
-
□ Symmetrical deformity of the knee.
-
□ Increased the intermalleolar distance.
-
-
Treatment
-
□ Reassurance: physiologic valgus can improve up to the age of 8 years.
-
Blount Disease
Definition:
-
■ It is a developmental deformity resulting from abnormal endochondral ossification of the medial aspect of the proximal tibia physis leading to varus deformity and internal rotation of tibia.
-
■ It is also known as tibia vara.
Types:
-
■ Infantile type.
-
■ Adolescent type.
-
Infantile type of Blount’s disease is more progressive than the adolescent type due to greater growth potential.
-
Infantile type:
Incidence:
-
■ Occurs in infant and young children (2–4 years).
-
■ More common in black obese infants.
Pathology:
-
■ Affection of the proximal medial tibial physis
-
Decrease growth from the medial side with continued growth from the lateral side of the physis results in varus deformity.
-
Clinical presentation:
-
■ Severe progressive genu varum with internal rotation of the lower leg (Fig. 7.11).
Fig. 7.11 
Infantile tibia vara. 3-year-old girl weighing 44 kilograms presenting with bilateral genu varum with internal tibial torsion more on the right side
-
■ The condition is usually bilateral.
-
■ In unilateral cases, the condition can be associated with leg-length discrepancy.

Radiographs
-
■ Metaphyseal-diaphyseal angle (Fig. 7.12).
Fig. 7.12 
Metaphyseal diaphyseal angle. This is the angle between the line perpendicular to the lateral border of the tibia and the line across the widest area of the metaphysis. Angle >16° indicates Blount’s disease and angle <11° indicates physiologic genu varum
-
More than 16°: is specific for infantile Blount’s.
-
Less than 11°: is indicator of physiological genu varum.
-
Between 11–16°: can be either physiological genu varum or infantile Blount’s.
-
-
■ Growth plate changes in the medial aspect of the proximal tibial (Fig. 7.13).
Fig. 7.13 
Radiological changes in Blount’s disease. (a) Long radiographs (scanogram) of a 3-year-old girl showing the proximal tibial metaphyseal beaking (arrow). (b) A 4-year-old boy with depression of the medial tibial plateau and fusion of the growth plate on the medial side (arrow). Note the difference between the medial and lateral sides of the tibial growth plate
-
■ Medial metaphyseal peaking is often present (Fig. 7.13).


Treatment:
-
Knee Brace to correct varus before the age of 3 years.
-
If no improvement or if the patient is more than 3 years old: orthopedic referral for surgical treatment.
Adolescent type:
Incidence:
-
■ Less common than the infantile type.
-
■ The disease is common in adolescent obese boys.
Clinical picture:
-
■ Can be unilateral or bilateral.
-
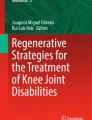
■ Radiograph will show varus deformity of distal femur and proximal tibia with less obvious affection of the growth plate (Fig. 7.14).
Fig. 7.14 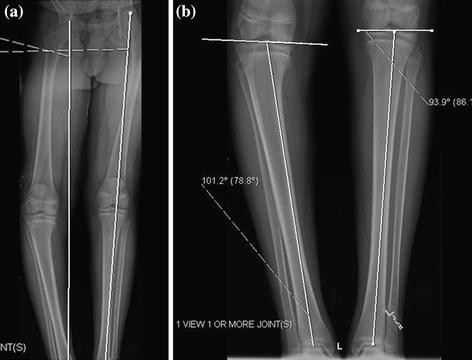
Radiographic changes of adolescent tibia vara. A 15-year-old black male presented with unilateral adolescent tibia vara on the right side. (a) Scanogram shows varus alignment on the right side with the mechanical axis medial to the joint. (b) Radiographs of the leg shows varus deformity of the proximal tibia

Treatment:
-
■ Orthopedic referral of surgical intervention (osteotomy).
Knee Pain in Children
Cause:
-
■ Patellofemoral pain:
-
□ Patellar overload.
-
□ Chondromalacia patellae.
-
□ Patellar subluxation.
-
-
■ Extensor mechanism inflammation:
-
□ Osgood–Schlatter.
-
□ Jumper’s knee.
-
□ Sinding–Larsen–Johansson Disorder.
-
-
■ Tumor:
-
Osteosarcoma.
-
Ewing sarcoma.
-
Osteoid osteoma.
-
Unicameral bone cyst.
-
-
Vascular:
-
Osteochondritis dissecans.
-
-
■ Traumatic:
-
Meniscal tear.
-
Ligament injury.
-
Knee plica.
-
Stress fractures:
-
□ Proximal tibial stress fractures.
-
-
-
■ Infections.
-
Septic arthritis.
-
Osteomyelitis of the proximal tibia or distal femur.
-
Septic bursitis (Fig. 7.15)
Fig. 7.15 
Knee bursitis. A 14-year-old boy with 4 days history of anterior knee pain, swelling, and redness. Examination shows inflammation of the prepatellar bursa (pre patellar buritis). The patient was treated with antibiotic with complete resolution of his symptoms
-
□ Prepatellar bursitis.
-
□ Infrapatellar bursitis.
-
-
-
■ Rheumatologic condition:
-
Juvenile rheumatoid arthritis.
-
-
■ Referred pain:
-
Hip pathology, e.g., SCFE.
-
-
■ Miscellaneous:
-
Growing pain.
-
Bipartite patella.
-

Approach to child with knee pain
-
■ History:
-
Pain:
-
□ Onset, duration, progression, and exact location.
-
-
Precipitating factor:
-
□ The exact mechanism of injury.
-
-
General manifestation of infection (fever, chills)
-
Ability to bear weight
-
Ability of the child to continue his/her usual activities.
-
□ Children with simple growing pain can continue all their regular activities.
-
-
-
Physical exam:
-
Examination of the ipsilateral hip.
-
Examination of the contralateral knee (for comparison).
-
Examination of the affected knee.
-
□ Range of motion, active and passive, is the most sensitive indicator of arthritis.
-
-
-
Imaging:
-
Radiographs of the affected knee.
-
Radiographs of the ipsilateral hip.
-
If there is persistence of pain with negative plain radiographs, consider obtaining MRI.
-
Osgood–Schlatter Disease
Definition:
-
■ Inflammation of the insertion of the patellar tendon in the tibial tubercle (tibial tubercle apophysitis).
Incidence:
-
■ More common in
-
Boys.
-
In children active in sports that require repeated of knee movement like soccer.
-
Clinical presentation:
-
Patient will complain of anterior knee pain and swelling.
-
□ The pain is related to physical activity.
-
-
On examination; tender swelling at the tibial tubercle (Fig. 7.16).
Fig. 7.16 
Osgood Schlatter. (A and B) A 14-year-old boy soccer player with right knee pain. Examination shows anterior knee swelling over the tibial tubercle (arrow)

Radiographs of the knee (Fig. 7.17)

Radiological signs of Osgood Schlatter. Radiographs of a patient with Osgood–Schlatter disease. Wide arrow points to the enlarged tibial tubercle. Small arrow points to the small fragment of calcification and fragmentation within the patellar ligament
-
■ Enlargement of the tibial tubercle (tibial apophysis).
-
■ Possible fragmentation of the tibial apophysis.
Treatment:
-
First line:
-
□ Decrease activity (the child may have to stop practicing sports for few months).
-
□ NSAIDs.
-
-
If no improvement:
-
□ Physical therapy.
-
○ Stretching of the hamstring.
-
○ Quadriceps strengthening.
-
-
□ Brace (knee immobilizer).
-
-
Orthopedic referral is rarely needed.
Sinding–Larsen–Johansson Disorder
-
■ Inflammation of the distal pole of the patella (traction apophysitis).
-
■ Affected population and clinical presentation is similar to Osgood–Schlatter disease except that pain in related to the lower end of the patella.
-
■ Treatment: as Osgood–Schlatter disease.
Jumper’s knee:
-
■ Inflammation of the patellar tendon.
-
■ Affected population and clinical presentation is similar to Osgood–Schlatter disease except that pain in related to the patellar tendon.
-
■ Treatment: as Osgood–Schlatter disease.
Osteochondritis Dissecans
Definition:
-
■ Osteochondritis dissecans occurs when an area of the bone close to the articular cartilage becomes avascular and ultimately separates from the underlying bone.
Causes:
-
■ The exact cause is unknown. Theories include:
-
Trauma.
-
Repeated stresses.
-
Familial predisposition.
-
Location:
-
■ Most lesions located on the lateral portion of the medial femoral condyle (Fig. 7.18).
Fig. 7.18 
Osteochondritis dissecans. Radiographs of left knee (a: anteroposterior; b: Notch view) showing osteochondral defect on the medial femoral condyle

Clinical presentation:
-
■ Vague knee pain.
-
■ Recurrent effusion.
-
■ If the fragment become loose or separated, there can be crepitation, popping, and occasionally locking of the knee.
-
Physical finding:
-
Parapatellar tenderness.
-
Quadriceps atrophy.
-
Pain with range of motion.
-
Knee effusion.
-
Diagnosis:
-
■ Radiograph will show:
-
Subchondral fragment with a lucent line separating it from the condyle (Fig 7.18).
-
-
■ MRI is more sensitive and can detect early cases.
-
■ Arthroscopy is the most reliable method in evaluating the status of the lesion.
Treatment
-
■ Most stable lesions will heal spontaneously.
-
■ Orthopedic referral.
-
MRI will guide the treatment plan:
-
If the lesion is stable (non detached) from underlying bone:
-
□ Activity modification.
-
□ Physical therapy for strengthening.
-
-
If the lesion is detached from the underlying bone or no improvement with non operative management:
-
□ Operative treatment (arthroscopy) for either fixation of the fragment or excising it.
-
-
Patellar Instability (Recurrent Patellar Subluxation and Dislocation)
Anatomical considerations:
-
■ The patella lies in the trochlear groove of the distal femur.
-
■ The patella almost always dislocate laterally.
-
■ The line of pull of the quadriceps tendon is not in line with patellar tendon. The angle between them is called Q angle (Fig. 7.19).
Fig. 7.19 
Q angle is the angle between the axis of the femur (from the ASIS to the patella) and the axis of the patellar ligament (from patella to tibial tubercle)
-
Factors that increase the Q angle will cause more susceptibility to dislocation and subluxation.
-
-
■ The main restrain against lateral patellar dislocation is the medial patello-femoral ligament which extends from the medial femoral condyle to the medial patella.

Predisposing factors for recurrent dislocation and subluxation:
-
■ Dysplastic trochlear groove.
-
■ Patella alta (high riding patella).
-
The patella will not be seating in the trochlear groove as it will lie above it.
-
-
■ Increase Q angle:
-
Genu valgum.
-
Increased femoral anteversion.
-
External tibial torsion.
-
Laterally positioned tibial tuberosity.
-
-
■ VMO (vastus medialis obliqus) insufficiency:
-
The muscle fibers of the quadriceps responsible for pulling the patella medically.
-
-
■ Syndromes associated increased laxity.
-
Down syndrome.
-
Ehlers–Danlos syndrome.
-
Marfan’s syndrome.
-
Turner’s syndrome.
-
Clinical Presentation
Classification of patellar dislocation by history
-
■ Recurrent patellar dislocation.
-
History of repeated dislocation.
-
With the dislocation event the patella will lie on the lateral side of the knee and has to be reduced back by the patient himself or someone else.
-
-
■ Recurrent patellar subluxation.
-
History of repeated subluxation. The patient feels that the patella is unstable, but no full dislocation.
-
Usually associated with knee pain.
-
-
■ Habitual dislocation of the patella.
-
Dislocation of the patella each time the patient bends his knee.
-
-
■ Chronically dislocated patella.
-
The patella had been always in a dislocated position (Fig. 7.20).
Fig. 7.20 
Chronically dislocated patella. A 17-year-old patient with right chronically dislocated patella since early childhood. (a) The patella lies on the outer aspect of the knee (dotted circle). Axial CT (b) and coronal reformat (c) shows the abnormal shape of the patella which is lying outside the groove
-
-
■ Examination of the lower extremity for the predisposing factors.
-
■ General examination for signs of increased laxity (e.g., elbow hyperextension).
-
■ The condition may be bilateral.
-
■ Parapatellar tenderness.
-
■ Mild effusion.
-
■ Specific test for patellar stability:
-
Tracking of the patella (J sign)
-
□ Assess patellar tracking by flexing and extending the knee.
-
□ Positive J sign with patella deviating laterally at the end of extension.
-
-
Apprehension sign
-
□ Positive result (quadriceps contraction or apprehension look on the face) indicates instability (Fig. 7.21):
Fig. 7.21 
Apprehension sign. The patient lies supine on the table with the knee in 20–30° of flexion and the quadriceps relaxed. The examiner carefully glides the patella laterally observing for the apprehension sign. A positive test is the presence of this reaction by the patient
.
-
-


Imaging:
-
■ Radiographs:
-
Sunrise view (Fig. 7.22) will show the lateral tilt of the patella.
Fig. 7.22 
Sunrise view. This view shows the position of the patella in the trochlear groove
-
-
■ CT and MRI
-
Can better delineate the tilt of the patella.
-
May show trochlear hypoplasia.
-

Treatment
-
■ After first dislocation:
-
Knee immobilizer for 1–2 weeks followed by physical therapy.
-
-
■ Recurrent dislocation:
-
Therapy: isometric quadriceps-strengthening exercise
-
Orthopedic referral: Surgery is indicated if conservative treatment fails.
-
□ Correction of underlying deformity (e.g., genu valgum)
-
□ Reconstruction of the medial patellofemoral ligament.
-
-
Popliteal Cyst (Baker Cyst)
Definition:
-
■ Baker cyst is common in children.
-
■ It is a cystic mass filled with gelatinous material that develops in the popliteal fossa.
Clinical presentation:
-
■ It is more common in boys.
-
■ Usually found on the medial side of the popliteal fossa (Fig. 7.23).
Fig. 7.23 
Popliteal Cyst (Baker Cyst). A 6-year-old boy brought with his family because of non painful swelling on the back of the right the knee. The arrow shows the baker’s cyst on medial side of the back of the knee
-
■ Painless.
-
■ It can disappear spontaneously within 6–24 months.

Treatment
-
■ A prolonged period of observation is recommended before considering surgical excision.
-
■ Indication of further diagnostic evaluation (Atypical finding):
-
□ Tenderness.
-
□ Firmness (solid mass).
-
□ History of rapid enlargement.
-
□ Pain.
-
-
■ If swelling persists for more than 12 months or atypical findings, orthopedic referral for excision.
Patellofemoral Pain Syndrome
Other names
-
■ Chondromalacia patella (misnomer as the patellar cartilage is intact).
-
■ Patellar overload syndrome.
Definition:
-
Knee pain due to increased loads of the patellofemoral joint.
Clinical presentation:
-
■ A common cause of knee pain in adolescent girls.
-
■ Anterior knee pain that increases with activity.
Predisposing factor:
-
■ Certain mechanical factors lead to increased stress on the patellar cartilage by causing uneven distribution of stresses through the articulation between patella and trochlea.
-
Miserable malalignment syndrome:
-
□ Common rotational malalignment in adolescent females.
-
□ It consists of the following three elements (Fig. 7.24):
Fig. 7.24 
Miserable malalignment syndrome. A 15-year-old girl with 2 years history of knee pain. Patient had excess femoral anteversion as manifested by her patellas pointing inward. Despite the inward position of the patella, her foot is still pointing forward due to her external tibial torsion
-
○ Increased femoral anteversion.
-
○ External tibial torsion.
-
○ Pes planus (flat foot).
-
-
-
Increased Q angle.
-

Treatment
-
■ Ice, rest, NSAID.
-
■ Physical therapy:
-
Quadriceps strengthening and hamstring stretching.
-
-
■ Patellar stabilizing braces may be needed.
-
■ If no improvement: orthopedic referral (surgery is rarely indicated, results are not always very promising).
Congenital Condition Affecting the Leg
Fibular hemimelia:
Definition:
-
■ Congenital condition with abnormal development of the fibula.
-
■ Considered type of longitudinal deficiency of the limb.
Incidence:
-
■ One in every 100,000 live birth.
Clinical presentation:
-
■ Limb length discrepancy (LLD). The affected side will be shorter than the other side (Fig. 7.25).
Fig. 7.25 
Fibular hemimelia. A 4-year-old girl with left side fibular hemimelia. (a) The patient has 5 cm limb length discrepancy (white line indicating the knee level bilaterally), with pelvic obliquity (black line). (b) The left foot shows the absence of the most lateral ray
-
Positive Galeazzi sign.
-
Limping.
-
-
■ Foot:
-
Deficiency of the lateral rays of the foot (Fig. 7.25).
-
Abnormal development of the carpal bone.
-
Valgus deformity of the foot.
-
-
■ Knee:
-
Deficiency of the anterior cruciate ligament.
-
Valgus deformity of the knee due to abnormal shape of the lateral femoral condyle.
-

Radiographs:
-
■ Scanogram (radiographs of the whole lower extremity (Fig. 7.26):
Fig. 7.26 
Long radiographs of both lower extremity (scanogram) of the patient in Fig. 7.25. (a) The radiograph shows the 5 cm difference between both sides. (b) External fixator was applied and distraction osteogenesis was done to lengthen the affected bone. (c) 5 cm of new bone regenerate was formed (arrow)
-
LLD.
-
Valgus deformity to the extremity.
-

Management:
-
■ Orthopedic referral (see Chap. 2).
Congential Pseudoarthrosis of the Tibia
Definition:
-
■ Developmental condition of persistent non union of distal part of tibia.
-
■ Pseudoarthrosis: means non union with excess motion between the two ends of the bone (false joint).
Clinical presentation:
-
■ The child will have anterolateral bowing of his tibia (Fig. 7.27).
Fig. 7.27 
Congenital pseudoarthrosis of the tibia. A 3-year-old boy with spontaneous fracture of the left leg. (a) Radiograph shows fracture with non union (pseudoarthrosis) of the tibia and fibula. (b) Clinical picture of the leg shows the anterior bowing of the leg
-
■ The condition usually occurs spontaneously in the second or third years of life.
-
Spontaneous fracture of the leg will occur (with minimal or no history of trauma).
-
-
■ About 50 % of these children will have neurofibromatosis.
-
■ Persistence of non union (or recurrence of fracture) despite multiple surgical interventions.
-
■ Pain is minimal.

Radiograph:
-
■ Anterolateral Bowing of the tibia (Fig. 7.27).
-
■ Atrophic non union of the distal tibia and fibula (atrophy and sclerosis of the bone ends).
Management:
-
■ Orthopedic referral.
-
The non union is very resistant to healing (one of the most tough conditions to treat in pediatric orthopedic).
-
Sometimes amputation of the extremity is the only possible method of treatment especially after multiple failures to achieve union or multiple re-fractures.
-
Bowing of the leg:
-
□ There are different types of bowing of the leg.
-
□ The direction of the bow is the direction of the apex of the bow.
Anterolateral bowing:
-
■ Usually associated with congenital pseudoarthrosis of the tibia (Fig. 7.27).
-
■ Most dangerous type of tibial bowing.
-
■ Treatment:
-
Orthopedic referral for bracing.
-
Posteromedial bowing of the tibia
-
■ Usually resolve spontaneously with growth.
-
■ Takes about 7–10 years to remodel.
-
■ Associated with:
-
Calcaneovalgus deformity of the foot.
-
LLD (the affected leg is usually shorted by about 3–5 cm at the end of growth).
-
-
■ Treatment:
-
Orthopedic referral for management of LLD.
-
No need for bracing (no increased risk of fractures).
-
Anteromedial bowing of the tibia:
-
■ Associated with fibular hemimelia.
High Yield Facts
-
■ Genu varum is normal finding until the age of 2 years old, and then the knee alignment changes to valgus that reaches maximum by the age of 3 years old.
-
■ At about the age of 8 years, most children will reach adult alignment of 7 degrees of valgus.
-
■ Presence of bowlegged after 24 months, unilateral, and > 20 degree clinically should be evaluated.
-
■ Children with infantile Blount’s disease who are older than 3 years or failed brace treatment should be referred to orthopedics for surgical correction.
-
■ Patellofemoral pain is common in adolescent girls. Treatment is mainly non operative.
-
■ Genu valgum, patella alta, and hypoplastic trochlear groove are among the predisposing factors for patellar instability.
-
■ Patellar instability can present with recurrent attacks of patellar dislocation or patellar subluxation and pain.
-
■ Popliteal cyst is a common condition in children. Observation for up to 12 months is the appropriate first treatment.
-
■ Rest, NSAIDs, quadriceps stretching and strengthening, and cross training is the most appropriate initial management of Osgood–Schlatter disease.
-
■ Anterolateral bowing of the tibia is associated with congenital pseudoarthrosis of the tibia (a condition which is very resistant to treatment).
-
■ Posteromedial bowing of the tibia is associated with limb length discrepancy.
Clinical Scenarios
The presenting patient | The most probable diagnosis and plan of action |
|---|---|
13-year-old girl soccer player complaining that she had three dislocation of her “knee cap” in the last year during her practice. On exam, the patient has obvious bilateral genu valgum | Patellar instability with genu valgum |
■ Orthopedic referral for correction of the deformity | |
15-year-old boy basketball player complaining of right knee pain and swelling during and after practice, he said his knee is locking. Physical examination showed atrophy and weakness of the quadriceps muscle, tenderness on the media condyle of the femur, and mild joint effusion, radiograph on the right knee revealed lucency in the medial femoral condyle. What is the most likely diagnosis? | Osteochondritis dissecans |
Orthopedic referral | |
■ MRI | |
■ If the lesion is stable (not separated from the underlying bone), conservative treatment for 3 months | |
12-year-old football player complained of leg pain for the last 1 month which is more after the games, physical examination showed swelling, tenderness to palpation of tibial tuberosity. | Osgood-Schlatter disease |
Treatment | |
■ NSAID | |
■ Avoid excessive sport activities for few weeks | |
18-month-old boy brought to the clinic by his mother for deformity of the left leg. On exam, patient has multiple cafe au lait patches on the trunk and back. The left leg is bowed with abnormal movement in the lower third. Radiographs show a fracture of the tibia and fibula with sclerotic edges | Neurofibromatosis with congenital pseudoarthrosis of the tibia |
■ Orthopedic referral | |
■ Warn the family that the condition will need multiple surgeries and may end in amputation |
References
Staheli LT. Knee and tibia. In: Staheli LT, editor. Practice of pediatric orthopedics. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2006. p. 143–58.
Sponseller PD. Bone, joint, and muscle problems. In McMillanJA, Feigin RD, DeAngelis C, Jones MD, editors. Oski’s Pediatrics: Principles and practice. 4th ed. Philadelphia: Lippincott Williams and Wilkins; 2006. p. 2470–2504.
Kocher MS, Tucker R, Ganley TJ, Flynn JM. Management of osteochondritis dissecans of the knee: Current concepts review. American Journal of Sports Medicine. 2006;34(7):1181–91.
Davids JR. Pediatric knee. Clinical assessment and common disorders. Pediatric Clinics of North America. 1996;43(5):1067–90.
Lehman WB, Abdelgawad AA, Sala DA. Congenital tibial dysplasia (congenital pseudoarthrosis of the tibia): an atypical variation. Journal of Pediatric Orthopaedics B. 2009;18(5):211–3.
Herzenberg JE, Paley D. Leg lengthening in children. Current Opinion in Pediatrics. 1998;10(1):95–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Abdelgawad, A., Naga, O. (2014). The Knee/Leg. In: Abdelgawad, A., Naga, O. (eds) Pediatric Orthopedics. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-7126-4_7
Download citation
DOI: https://doi.org/10.1007/978-1-4614-7126-4_7
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-7125-7
Online ISBN: 978-1-4614-7126-4
eBook Packages: MedicineMedicine (R0)