
Abstract
The role of the androgen receptor (AR) signaling axis in the progression of prostate cancer is a cornerstone to our understanding of the molecular mechanisms behind this important disease. Understanding the innate signaling axis of the AR and the aberrations of this axis in progression of prostate cancer has facilitated the development of emerging therapeutic interventions. Furthermore, the crosstalk of AR with other critical signaling pathways may explain the advancement of prostate cancer to metastatic castration-resistant prostate cancer (CRPC). Of particular interest to such crosstalk are the pathways associated with epithelial to mesenchymal transition (EMT). The reactivation of EMT is a hallmark of metastatic cancer spread, and recent evidence suggests the involvement of AR in the signaling pathways regulating EMT. Cadherin switching, EMT inducing transcription factors, Wnt, TGF-β, and Notch signaling can all be modulated by crosstalk with the AR. Overexpression and localization of the AR to the nucleus has been associated with reactivation of the androgenic signaling axis and progression to metastatic CRPC in patients. In this chapter we consider the current understanding of the functional exchanges between the androgen signaling championed by AR activity and key growth factor signaling pathways that impact EMT towards prostate cancer progression to metastatic CRPC and we discuss the clinical relevance of these insights in the effective targeting of advanced disease.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
15.1 Introduction
The pioneering work of Huggins and Hodges [1], first established the significance of male steroid hormones in prostate cancer cell proliferation and that their withdrawal diminished prostate tumor growth [1]. Seventy years later, this observation is still a cornerstone of the clinical treatment paradigm in the management of patients with metastatic prostate cancer. Androgen deprivation therapy (ADT) by a variety of surgical and/or pharmacological methods ultimately, fails to effectively cure patients with prostate cancer; they relapse and progress to the more aggressive disease state “castration-resistant prostate cancer” (CRPC) or “hormone-refractory prostate cancer.” Therapeutic failure ADT is assessed by biochemical recurrence, monitored in patients by sequential evaluation of serum prostate-specific antigen (PSA). It is indeed the alarmingly high number of 70,000 American men who develop disease recurrence each year that represents the treatment challenge for urologists, oncologists, and radiation oncologists, as well as basic scientists [2, 3]. Despite the shortcomings of PSA screening, it facilitates the identification of at risk patients experiencing biochemical recurrence to metastatic CRPC progression. The androgen signaling axis still remains the focal point of the first line clinically viable therapeutic approach to impeding prostate cancer progression [1, 3]. Progression to CRPC is characterized by increased androgen receptor (AR) expression, elevated intraprostatic androgens, and perpetually activated AR signaling despite physiologically castrate levels of androgens [4, 5]. Mechanisms via which androgenic/AR signaling is maintained in androgen-depleted environments and effects on target gene expression include the potential AR mutations, amplification, alternative splicing, overexpression, and altered sensitivity yielding altered AR expression and/or aberrantly activated function in diverse cellular processes involved in tumorigenesis [6]. Emerging evidence suggests that reactivation of epithelial–mesenchymal transition (EMT) processes may facilitate the development of prostate cancer [7], with increasing number of studies focusing on the direct involvement of androgen/AR signaling in EMT/MET transitions. The clinicopathological significance of EMT in human cancers continues to be a topic of debate. As the cellular landscape EMT is being interrogated by proteomic analysis toward defining its role in prostate cancer progression to metastasis. Investigating the regulatory mechanisms by which EMT programs are controlled by the androgen/AR signaling, is fundamentally important for understanding the functional contribution of EMT processes to various stages of prostate tumor progression to metastasis and emergence of CRPC disease.
15.1.1 The Androgen Receptor in Control of Prostate Growth
The AR is a member of the steroid–thyroid–retinoid nuclear receptor superfamily found on the X chromosome (Xq11-12) spanning approximately 180 kb of DNA with 8 exons [8]. In the normal AR signaling axis, testosterone synthesized in the testis or by the adrenal gland is sequestered by sex hormone-binding protein circulating in the blood sera. Dissociation from SHBP and diffusion across the plasma membrane brings testosterone into proximity with the cytochrome p450 enzyme 5 α- reductase (SRD5A1, SRD5A2) producing the cognate ligand of AR (dihydrotestosterone; DHT) [9–11]. Binding of DHT to the AR facilitates the rearrangement of AR domains and within the heat shock protein 90 super complex and subsequent transcriptional activation. AR bound to DHT homo-dimerizes and becomes activated via phosphorylation by the Protein Kinase A signaling pathway [12, 13]. The homo-dimer translocates into the nucleus and is able to bind androgen-responsive genes (ARG) at specific palindromic DNA sequences known as androgen- responsive elements (ARE) (Fig. 15.2a) [14]. This binding to ARE DNA allows the homo-dimeric AR to act as a scaffold and recruit coregulators and modulate transcription via actions as transcription factor [14–16]. The binding of the AR to the ARE forms a stable pre-initiation complex near the transcriptional start site facilitating the recruitment and initiation of RNA polymerase II (Fig. 15.2a) [17].
15.1.2 The Structure of AR
The AR is composed of an amino-terminal-activating domain (NTD), a carboxy-terminal ligand-binding domain (LBD), a DNA-binding domain in the mid-region that contains two zinc finger motifs to facilitate the interaction of the protein with the DNA double helix (DBD), and a hinge region to facilitate the change in protein folding upon binding to the ligand and dimerization (Fig. 15.1). These four domains comprise the 919 amino acid protein with a mass of 110 kDa. N-terminal Domain: The NTD (exon 1, amino acids 1–537) has been shown to possess multiple transcriptional activating units (TAU): TAU-1 and TAU-5 (Fig. 15.1) [17]. TAU-1 is associated with wild type AR transcriptional activation and is characterized by a high number of acidic amino acids, three glutamine repeats, and a phosphorylation site. Conversely, the TAU-5 sequence is characterized by stretches of proline, alanine, and glycine [17]. Having been attributed with 50 % of aberrant AR activity in CRPC, TAU-5 is responsible for the constitutive transcriptional activity of the NTD and is mediated by a core sequence of 435WHTLF439 in between the aforementioned alanine and glycine stretches (Fig. 15.1) [9, 18]. DNA-binding domain: The cysteine-rich DBD (exons 2 and 3, amino acid: 68) contains two important motifs [19]. The P-box motif found in the first of two zinc fingers facilitates the interaction of the AR with gene-specific nucleotide sequences inside the major groove of the DNA double helix (Fig. 15.1) [20]. The D-box motif mediates the DBD/LBD interaction that allows for inter-domain interaction and AR homo-dimerization after activation and facilitates the spacing of the AR over the half sites and binding on the ARE (Fig. 15.1) [9, 20–22]. The DBD contains one of the nuclear localization signals (NLS) as discussed below.

Androgen receptor structure: schematic diagram of protein domains and functions
Hinge Region: With only approximately 50 amino acids, the hinge region packs a big punch in a small space. The nonconserved and flexible hinge region separates the LBD and the DBD while containing part of the bipartite nuclear localization signal (Fig. 15.1) [23, 24]. The hinge region (as well as DBD and LBD) also contains a site for interaction with Filamin A, an actin interacting protein and signaling scaffold required for nuclear translocation of the AR [9, 25]. The hinge region plays a role in nuclear localization, DNA-binding inhibition, coactivator recruitment, and the N-terminal/C-terminal interaction of the AR [23]. Interestingly, a span of highly basic residues between 629 and 636 (629-RKLKKLGN-636) is conserved in all AR sequences known and decreases the affinity of AR for DNA binding as demonstrated by deletion constructs [23]. Ligand-Binding Domain: The LBD (exons 4–8, ∼250 amino acids) mediates the binding of the AR ligand (testosterone or DHT) to the AR protein and initiates the downstream cascade of the androgen signaling axis [9]. In addition to ligand binding, the LBD associates with the heat shock protein super-complex, interacts with numerous coregulators, and participates in receptor dimerization (Fig. 15.1 and 15.2a) [26–29]. The AR protein is composed of two activation domains (AF-1 and AF-2). The AF-1 domain is localized to the NTD and is composed of TAU-1 and TAU-5 domains contributing to the transcriptional activation program (Fig. 15.1). The AF-2 domain is localized to the LBD and interacts with LxxLL-containing coregulators such as the steroid receptor coactivators (SRC) and TAU domains in the NTD [9, 30].

Targeting AR translocation to the nucleus in prostate cancer. (a) After binding of cognate ligand, molecular handling by super-chaperone complexes, dimerization, phosphorylation, and association with dynein motor proteins onto microtubules (MT), AR translocates to the nucleus to mediate transcription of Androgen-responsive elements (ARE). (b) Taxane chemotherapeutics stabilize the interaction of β-tubulin subunits within the proto-filaments of the microtubule preventing the de-polymerization of the structure resulting in G2M arrest, apoptosis, and increased accumulation of AR in the cytoplasm. (c) With regard to Docetaxel (Taxane) resistant—CRPC, largely unknown mechanisms are employed which facilitate translocation of AR to the nucleus despite microtubule stabilization
15.1.3 The AR Localization: Translocation Matters
The AR is sequestered in the cytosol by the Hsp90 super-complex awaiting its cognate ligand DHT for initiation of the nuclear translocation protocol. The bipartite nuclear localization signal (NLS1) spans the DBD and hinge regions with exons 3 and 4 represented in [22]. This NLS is composed of the sequence, RKCYEAGMTLGARKLKK, and two basic motifs represent important sequence components which facilitate AR nuclear translocation (indicated in bold) [22]. The bipartite nature of the NLS ensures that there is cooperation between the different protein domains to allow nuclear shuttling. The AR NLS is regulated by the binding of the LBD to the cognate ligand, facilitating a conformation change in the protein that places the NLS in a functional orientation for translocation [22]. After AR has bound DHT, homo-dimerized, activated by phosphorylation, and translocated to the nucleus, the exposure of the NLS allows binding to the importin-α adaptor protein and importin-β carrier protein [31]. This allows movement through the nuclear pore complex and Ran-dependent release into the nucleus [32–37]. There is however a second NLS sequence (NLS2) in the LBD, that allows the AR to enter the nucleus in an importin-α-independent mechanism [27, 38, 39]. In addition to the importance of the bipartite NLS of the AR itself, the binding of AR to the Hsp90 super-complex aids to prevent aberrant signaling without cognate ligand activation. The hinge region of the AR is able to mediate an interaction with Filamin-A (FLNA) protein in the cytosol [25, 40]. The 280 kDa cytoskeletal protein, Filamin-A is a critical regulator of the solation–gelation equilibrium at the cell membrane by cross-linking F-actin fibers into orthogonal arrays and interacting with the AR and Hsp90 complex [25, 41]. Filamin-A is essential to mediating the translocation of the AR to the nucleus upon activation as well as the microtubule-associated motor protein, dynein [25, 40, 42]. Many of these important protein interactions have been mechanistically involved with the AR translocation to the nucleus; the molecular chain of events, however, responsible for this movement is not completely defined. The AR undergoes numerous interactions with coregulatory proteins that have been extensively reviewed [43]. The intramolecular interactions within the AR and intermolecular protein:protein interactions between AR subunits in a homo-dimeric complex are important to the activation and nuclear translocation [21]. Upon ligand binding, the D-box of the DBD interacts with the TAU-1 domain of the NTD, an N-terminal to C-terminal protein domain interaction that is initiated in the cytoplasm [21, 44]. This interaction between the D-box and the NTD of the AR is essential for the transition from intramolecular domain associations to intermolecular homo-dimerization, a process that occurs independent of DNA binding [44]. In fact, upon DNA binding the AR N/C interaction is lost, facilitating coregulator interaction with the AR and AR interaction with the major groove of DNA double helix [21, 45].
15.1.4 Pathways Bypassing AR
During the last decade there has been a plethora of mechanisms pursued as potentially engaged by prostate tumors to bypass or perpetuate AR signaling toward CRPC [5, 6, 12]. These mechanisms, comprehensively considered, lend credence to the need for personalized medicine and continued research in the landscape of alternate pathways to CRPC [5, 6, 12]. Alterations to the regulation, structure, and posttranslational modifications of the AR itself can perpetuate continued androgen signaling. The mRNA and protein expression of the AR is commonly overexpressed in CRPC [4]. However, the structure of the AR can be altered as well. Point mutations increasing the affinity of the AR for ligand have been identified causing the pathway to become hypersensitive [46]. Promiscuous mutations cause binding flexibility in the LBD allowing the AR to become activated by adrenal androgens, androgenic metabolites, and even some anti-androgen therapeutics such as flutamide and bicalutamide have been described [5, 47–49]. Moreover, over twenty splicing variants of AR, some lacking LBD, and therefore constitutively active have been identified and associated with progression of CRPC and metastasis [17, 50–54]. AR can be activated independent of ligand interactions by aberrant signaling pathways causing the activation of the protein and homo-dimerization by growth factors, receptor tyrosine kinases, and the Akt pathway via loss of PTEN [5, 55–57]. Recent evidence has elucidated the potential for prostate cancer cells to synthesize their own androgens “hijacking” adrenal synthesis enzymes [6, 58–60]. The entire AR signaling axis can even be bypassed by overexpression of the apoptosis blocking protein Bcl2, frequently found overexpressed in prostatic intraepithelial neoplasia (PIN) [61, 62].
15.2 The Therapeutic Impact of Impairing Androgen Signaling in Prostate Cancer
Taxanes were first identified in the bark of yew trees, and their cytotoxic effects against cancer cells were pursued with zest [63]. The underlying mechanism of action behind such drugs as Taxotere (Docetaxel) and Paclitaxel has been historically considered the binding to microtubules, leading to stabilization or destabilization of microtubules and ultimately mitotic catastrophy [63]. Specifically, taxanes bind two subunits of β tubulin, stabilizing the interaction and preventing de-polymerization of the protofilament within microtubule complex [64]. This stabilizing interaction ultimately results in G2M arrest and apoptosis [63, 64]. Taxanes are able to counteract the effects to some extent of Bcl-2 protein overexpression. Bcl-2 is a pro-survival protein and important effector of apoptosis frequently overexpressed in prostate cancer [65, 66]. Taxane treatment counteracts the anti-apoptotic effect of Bcl-2, one of significant modes of overcoming androgen dependence and progression to CRPC [67, 68]. The clinical evidence delivered much therapeutic promise. In 2004 the findings of two landmark clinical trials, TAX327 and SWOG (Southwest Oncology Group) 9916, demonstrated a benefit of Docetaxel-based treatment regimen in patients experiencing CRPC [69]. Docetaxel treatment produced benefits in palliative relief and overall survival and these results have persisted with extended follow ups [70, 71]. Since the approval of Docetaxel from the US Food and Drug Administration, this clinical use as chemotherapeutic drug has generated an additional, but sometimes modest, survival benefit to patients progressed to CRPC. Work from our lab revealed that in addition to these aforementioned effects in stabilizing microtubules and inducing G2M arrest, taxanes are particularly poignant in prostate cancer, because they possess the ability to block translocation of the AR to the nucleus and inhibit AR-driven gene transcription (Fig. 15.2b) [72]. Using clinical specimens from patients treated with Docetaxel versus untreated, immunohistochemical analysis of tissue microarrays strikingly revealed significantly diminished AR nuclear localization in the Docetaxel-treated patients [72]. Significantly enough these translational studies revealed that while AR protein expression levels were not affected by the taxane treatment, the nuclear transport and localization of AR was markedly reduced in response to Docetaxel (38% decrease), evidence that provided a intriguing new insight into the mechanisms of action of microtubule-targeting agents, as well as resistance in CRPC. Further investigation into the domain of the AR responsible for mediating the interaction with the taxane target tubulin revealed that the NTD negotiated this association [72]. These important mechanistic insights serve as a roadmap to understanding why Taxane chemotherapeutic served as our only clinically relevant treatment for CRPC for nearly a decade and guide our pursuit of future therapeutics (Fig. 15.2a). Taxane treatment ultimately fails, however, as the majority of patients develop resistance. The mechanisms driving prostate cancer progression after Docetaxel treatment are far from completely understood and this has been the focus of pursuit by investigative efforts from our group and others (Fig. 15.2c). A potential mechanism of resistance can be attributed to the adenosine triphosphate-dependent drug efflux pump P-glycoprotein-1. More recent evidence supports that Docetaxel has a high affinity for this pump and that an increase in expression of the efflux pump itself is observed over the course of prostate cancer progression [73, 74]. Exacerbating the insult of progression to CRPC, biochemical recurrence is associated with other clinical manifestations. Bone, brain, and lymph node metastasis as well as increasing amounts of pain secondary to the metastatic lesions are common in CRPC patients [73]. Emergence of new therapeutic interventions such as Cabazitaxel, Abiraterone acetate, and MDV 3100 have demonstrated additional survival benefits to the Docetaxel-resistant metastatic CRPC patients (DR-CRPC) [75], with emerging strategic combinations of microtubule-targeting taxane-based drugs with the androgen signaling agents for effective therapeutic outcomes in DR-CRPC patients.
15.2.1 Cabazitaxel
Cabazitaxel is a novel, next-generation Taxane chemotherapeutic drug that has been shown to be effective in the DR-CRPC landscape [75, 76]. It has been shown to be highly cytotoxic and have a low affinity for the adenosine triphosphate-dependent drug efflux pump: P-glycoprotein 1, known to confer chemotherapeutic resistance [77]. Cabazitaxel was shown in a multicenter, randomized, phase 3 clinical trial (Treatment of Hormone-Refractory Metastatic Prostate Cancer (TROPIC)) to result in a significant increase in overall survival [76, 78]. Tumor response, biochemical recurrence, and tumor progression were all favored by Cabazitaxel treatment and consequently the drug was approved by the US Food and Drug Administration for use in DR-CRPC patients [75, 76, 78]. In addition to imparting overall survival benefits to chemotherapy naïve patients, the findings associated with Cabazitaxel are its ability to confer additional overall survival benefits in patients with biochemical recurrence on ADT, Docetaxel chemotherapy, or both [73, 75].
15.2.2 Abiraterone
Abiraterone Acetate (AA) is a novel anti-androgen therapy designed to target the adrenal androgen-mediated signaling axis by blocking the synthesis of adrenal products which serve as precursors for testosterone and DHT synthesis [75, 77, 79]. AA acts as a pregnenolone analog, inhibiting the rate limiting enzyme, cytochrome P450 (CYP17A1), further inhibiting androgen biosynthesis [75, 77]. AA inhibits both the 17α-hydroxylase and 17,20 functions of CYP17A1 [77]. The efficacy of AA was demonstrated in the COU-AA-301 trial, confirming that AA imparted additional survival benefit compared to DR-CRPC men treated with placebo and prednisone. In addition to overall survival increase, benefits were seen with regard to time to disease progression, biochemical recurrence, and tumor burden [75, 77, 80]. These results highlight the importance of targeting the AR signaling axis in conferring survival benefits in DR-CRPC patients.
15.2.3 MDV3100
The translational significance of AR targeting in DR-CRPC gains further support by the development of the direct AR antagonist, MDV3100 [77, 81]. This androgen-targeting agent is a diarylthiohydantoin member of the family of AR antagonists rationally designed from the crystal structure of the AR bound to its ligand [81]. MDV3100 is effective in the context of AR overexpression, in addition to inhibiting AR nuclear translocation, preventing binding of the AR to DNA, blocking recruitment of co-activators to AR target genes, and inducing apoptosis [81–83]. MDV3100 has been shown to be efficacious in improving survival in prostate cancer patients previously treated with ADT (CRPC), in Docetaxel-resistant patients, as well as in DR-CRPC patients [77, 84, 85]. Recent reports indicate that MDV3100 inhibits translocation of constitutively active AR splice variants lacking portions or all of the LBD, implicating MDV3100 in circumventing progression to CRPC [86].
15.3 AR Navigates Emergence of CRPC
With the outlook of the therapeutic horizon evolving and improving rapidly, prostate cancer is still treated as a single disease [87]. Other major human malignancies (breast, non-small cell lung cancer, colon cancer) are classified based on molecular features, for example, breast cancer is subclassified based on the presence of estrogen receptor, progesterone receptor, Her2/neu, and BRCA-1 [87, 88]. This provided effective therapeutic targets for successful drug development for specific molecular subtypes [87, 88]. Considering that the therapeutic repertoire in androgen-dependent prostate cancer is being hijacked by the extensive tumor heterogeneity of the disease and the stromal–epithelial interactions, it is of paramount importance to identify subpopulations in which the AR axis that can be actively targeted via optimized therapeutic strategies and carefully designed treatment sequencing. One must recognize the functional promiscuity of AR in targeting repressors and activators during prostate cancer progression. Until recently, investigation into the identity and functional contribution of AR-targeted genes was conducted in a hypothesis-driven, meticulous, and linear manner, building pillars to base future pursuits of drug and biomarker discovery in prostate cancer. In 2012, the challenge of wading through the tremendous output of data from bioinformatics lies towards development of molecular signatures and target identification in advanced disease patterns remains. Application of combination techniques of proteomic analyses coupled with microassay analysis of gene expression facilitated identification of proteins in prostate cancer signaling landscape, which are significantly upregulated on both the protein and gene level by AR signaling [89–91]. Such “topologically significant” nodes allow interpretation of the pathways which are affected most by androgen signaling in prostate cancer [91]. Functional validation of critical signaling pathways regulated by the androgen axis and AR activity provides valuable opportunities for exploitation at the mechanistic and translational level in the management of prostate cancer [91]. The main pathways that have been interrogated in recent years include AR nuclear signaling, AR crosstalk with growth factor signaling, androgenic regulation of epithelial to mesenchymal transition (EMT), extracellular matrix (ECM) adhesion and integrin priming, and regulation of angiogenesis by androgens. Our efforts focus on dissecting the role of AR signaling and its crosstalk with critical signaling effectors of apoptosis in controlling the process epithelial to mesenchymal transition (EMT) towards progression to metastatic CRPC.
15.3.1 Epithelial to Mesenchymal Transition : “Moving and Shaping” the Metastatic Journey
The biological process of EMT was first described in the context of normal organ development [92]. Reactivation of EMT quickly became a hallmark of metastatic tumors. EMT is observed extensively in nonpathological conditions such as mechanisms of development including gastrulation and neural crest development in which epithelial cells must de-differentiate to a mesenchymal form, migrate, and redifferentiate into a new structure or organization [93]. EMT can be classified into three distinct subtypes based on the biological setting hosting its manifestation [94]. Type 1 EMTs are associated with embryonic implantation and gastrulation facilitating the stratification of the germinal layers [94]. Unlike Type 1, Type 2 EMTs are associated with wound healing, tissue regeneration, and organ fibrosis [94]. Type 2 EMTs are characteristically induced by inflammatory signaling, either as a response to injury-induced inflammation as seen in wound healing or ongoing inflammation of certain organs resulting in fibrosis [94]. Type 3 EMTs occur in neoplastic cells that undergo a manifold of genetic or epigenetic changes resulting in localized tumor cell proliferation [94]. The Type 3 EMT is responsible for changes that facilitate tumor cell invasion and metastasis [94].
The significance of EMT in cancer emerges as tumor cells must physically detach from their immediate primary tumor, invade into the surrounding microenvironment, intravasate into the vasculature, endure the turbulence of circulation in the blood stream or lymphatics, and extravasate from the circulatory system at a secondary site [93, 94]. Each step required for execution of EMT requires a vast number of molecular events [7, 93, 94]. Epithelial cells must begin their transition to a mesenchymal phenotype by disrupting their intercellular adhesive contacts [95], a phenomenon manifested by formation of apical constrictions and disorganization of the basal cytoskeleton resulting in detachment and loss of apical-basal organization [95–98]. The phenotype of detached cells becomes spindle-like and exhibits a front-rear polarity conferring enhanced motility and invasive shape [7, 99–101]. Further breakdown of the basal membrane and extracellular matrix (ECM) must occur for migration to ensue and this is accomplished via secretion of proteases and acquisition of migratory/invasive properties [95, 102]. Key mechanisms activating EMT include TGF-β and receptor tyrosine kinase (RTK)/Ras signaling in addition to the well-known canonical Wnt-/Β-catenin, Notch, Hedgehog, and NFκB-dependent pathways [103]. Cadherin switching is an important milestone and regulatory step in EMT development regulated by transcriptional regulators including Snail and Twist [103].
Recent investigations from this laboratory strongly implicate the androgen signaling axis as an active participant in the progression of the mechanistic sequelae of EMT [7, 104]. In what is seemingly becoming a controversial twist, androgens can induce EMT-associated changes in prostate cancer cells, regardless of their androgen sensitivity and AR status, conferring enhanced invasive and motile capacity therein as well as modulating known EMT transcriptional regulator, Snail [104]. Moreover, an inverse relationship between AR expression level and extent of androgen-induced EMT induction was established suggesting that very low level AR expression such as that seen immediately after beginning ADT may be contributing to metastatic spread of prostate cancer tumor cells [104]. Others have recently shown that prostate cancer cells expressing AR in androgen-deprived conditions undergo an EMT, indicated by decreased E-cadherin and increased N-cadherin and vimentin [105]. Confirmed previously, increased N-cadherin expression and metastasis was seen in LNCaP xenografts and human clinical specimens [106]. The β-catenin/Wnt-dependent signaling pathway is already a well-known accomplice in progression to EMT and metastasis, but the implication of this pathway under androgenic drive is essential to understanding prostate-specific EMT. Recent exciting insights into EMT regulation in prostate cancer implicates β-catenin in the androgen-modulated EMT effect [104].
15.3.2 Cadherin Switching and the Master Regulators of EMT
The physiological phenomenon known as “cadherin switching” has been accepted as a hallmark of EMT. E-cadherin or epithelial cadherin is an important cell adhesion protein mediating intercellular contacts and facilitating maintenance of tissue architecture. This is a protein essential to formation of adherens junctions which in combination with tight junctions mediate intercellular adhesion [93]. E-cadherin is structurally characterized as a single pass transmembrane glycoprotein which forms calcium-dependent homotypic interactions with E-cadherin on cell neighbors [93]. These essential interactions are anchored to the cytoskeleton by interactions with microfilaments composed of actin and mediated by β-catenin and α-catenin [93]. E-cadherin expression can be lost, nonpolar, or cytoplasmic expressed or alternatively transcriptional repression of E-cadherin can occur by diverse mechanisms engaging AR and its transcriptional coregulators [107]. Loss of E-cadherin expression results in loss of normal cell–cell interactions and facilitates progression of EMT and leads to metastasis [103, 108, 109]. Upon E-cadherin loss, N-cadherin expression is enhanced to promote the mesenchymal cell phenotype. N-cadherin or Neural-cadherin is a mesenchymal cell association protein that allows transient cell–cell contacts typically expressed in cell types including smooth muscle, myofibroblasts, endothelial cells, neurons, and neoplastic cells [7, 93, 110]. The cell types usually expressing N-cadherin are also typical components of the reactive stroma composing the microenvironment of the prostate cancer tumor cell [93]. The interactive mode employed by N-cadherin is not unlike that used by E-cadherin; this single span transmembrane protein engages in homotypic interactions with N-cadherin on neighboring cells [93]. Loss of E-cadherin has been associated with increasing Gleason grade in prostate cancer and the concept of cadherin switching is traditionally considered as predictive of metastatic development [111, 112].
E-cadherin expression is repressed by the zinc finger transcription factor Snail (SNAI1) [95]. Snail not only gained notoriety as a master regulator of EMT induction but also plays an essential role in embryonic development and cell survival [95]. Snail employs a mechanism of action whereby the transcription factor binds to the E-box of the E-cadherin promoter and silences gene expression promoting a mesenchymal phenotype (Fig. 15.3a) [7]. Interestingly enough, Snail is capable of modulating expression of proteins involved in tight junctions, including claudins, occludins, mucin-1, and cytokeratin 18 [113]. Further fulfilling its infamy of “master regulator,” Snail increases expression of mesenchymal phenotype-associated markers and proteins associated with invasive capacity: vimentin, fibronectin, metalloproteinase-2, -9, ZEB1, and LEF-1 [113]. To dissect the functional contribution of Snail to prostate EMT, one must focus on its crosstalk with the AR signaling axis. Indeed, AR may function in an analogous manner to Snail, thereby repressing the expression of E-cadherin and promoting EMT by itself (Fig. 15.3a) [114]. Work from this laboratory has demonstrated that in androgen responsive, TGF-β responsive, prostate cancer cell line, expression of Snail is significantly increased by exposure to DHT alone or in combination with TGF-β [104]. These observations support a functional involvement of the AR signaling navigated by Snail in acquisition of EMT characteristics of prostate tumor cells towards metastatic progression. Recent high throughput DNA analyses have furthered this investigation at the molecular level by identifying an ARE/ARG in the promoter region of Snail2 (slug), suggesting the direct modulation of Snail2 by AR [89].

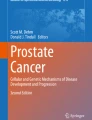
Role of AR in prostate cancer and EMT (a) Cadherin switching, Zeb1 feedback loop, and expression of Snail2 are modulated by the crosstalk with Androgen Receptor (AR). (b) TGFβ signaling can induce EMT-associated changes in Prostate cancer via Smad-dependent and -independent pathways and their crosstalk with the AR. (c) Wnt/β-catenin signaling engages in direct crosstalk with AR. AR and TCF-LEF1 transcription factors compete for β-catenin acting as a coactivator of transcription promoting EMT
A plethora of transcription factors impact expression and transcriptional activation of genes controlling the EMT phenomenon. Identification of those which specifically interact with the AR signaling axis provides a unique molecular platform begging exploration in prostate cancer (Fig. 15.3, panel A). Zeb1 (ZFHX1a gene) and Zeb2 (ZFHX1b) are closely related transcription factors whose activity has been strongly implicated in EMT [115]. These transcription factors are characterized by separated clusters of Zinc finger domain (7 total) which recognize the CAGGTA/G E-box promoter element [116]. ZEB1 modulates diverse-function genes, it significantly contributes to EMT by repression of E-cadherin expression, genes encoding basement membrane components, and regulators of cell polarity; other affects run the spectrum from tumor suppression to anti-adipose accumulation in vivo [7, 115–118]. Progression to metastasis is an event mediated by ZEB1, in addition to its important involvement in facilitating transendothelial migration [119, 120]. Clearly, ZEB1 plays an important role in orchestrating complex physiological processes such as, but certainly not limited to EMT. Recent work has revealed a bidirectional negative feedback loop between AR and Zeb1 that has implicated ADT in inducing EMT signatures in prostate cancer cells and human tissues [105]. Without androgenic stimulation, AR expression is diminished during early ADT, but in the absence of AR, Zeb1 expression cannot be inhibited and thereby becomes increased. With increased Zeb1 transcription factor expression, EMT promotion becomes transiently facilitated as a result of ADT leading to metastasis [105]. ZEB2 (SIP1) was originally described within the context of TGF-β signaling [116]. ZEB2 interacts with SMADs and promotes tumorigenic invasion and downregulates E-cadherin expression [121]. Expression of ZEB transcription factor has been correlated with progression to malignant carcinoma in various cancer types (including prostate), and that expression could be induced by both estrogen and progesterone [115, 122, 123]. Moreover, activated AR signaling induces ZEB1 in human prostate cancer cells and in triple negative breast cancer [115, 124]. Identification of AREs in the promoter of the ZEB1 gene confirms that expression of this dynamic regulator is controlled by AR signaling [115].
Identification of Enhancer of Zeste Homolog 2 (EZH2) from Chinnaiyan’s research group has been significant in understanding the role of epigenetic modifications in prostate cancer progression to EMT as well as in renal and breast cancer [125]. EZH2 expression is associated with cancer metastases and is markedly localized to tumors with poor prognosis in combination with depressed E-cadherin, both markers associated with poor disease-free survival [126, 127]. EZH2 functions as a histone lysine methyltransferase and its overexpression has been detected in mCRPC [126, 128]. Both EZH2 mRNA and protein levels are significantly elevated in prostate cancer compared to benign prostate hyperplasia (BPH) or human high grade PIN (HGPIN) [129]; however, in 2012 the precise role of EZH2 in prostate cancer progression is not fully understood. EZH2 targets NKX3.1 inducing repression of the homeobox gene, phenomenon observed in up to 85% of HGPIN lesions and prostatic adenocarcinomas [128]. Furthermore, EZH2 targets other genes undeniably linked to EMT, including E-cadherin and DAB2IP [130, 131]. The fusions of TMPRSS2, an androgen-regulated gene, and the oncogenic ETS transcription factor ERG place ERG under androgenic drive [132–137]. ERG activates EZH2 transcription allowing the methyltransferase to induce its repressive epigenetic agenda [138]. The neuronal chemorepellant and tumor supressor gene SLIT2 has also been linked to EZH2 [139]. EZH2 targets SLIT2 and inhibits its expression under the drive of AR-dependent TMPRSS2-ERG fusion [139]. SLIT2 is downregulated in a majority of prostate cancers and low levels of SLIT2 are associated with agressive disease [139]. ERG overexpression interferes with AR binding to ARE/ARGs, thus providing an additional layer of selection pressure to AR overexpression and mutation, driving progression to CRPC [138].
15.3.3 The Wnt Signaling and AR: Up, Close, and Intimate Interactions in Metastasis
The Wnt signaling pathway plays an important role in embryonic development and differentiation and is a highly conserved pathway among organisms. The deregulation of Wnt signaling is associated with tumorigenesis and EMT [140]. In prostate cancer cells, this pathway can engage in direct crosstalk with AR, with the central protagonist being β-catenin [140]. This molecule is located in distinct cellular locations: sequestered at the adherens junctions in concert with E-cadherin, in the cytoplasm, or in the nucleus [140]. Wnt ligand binds with the seven pass transmembrane receptors: FZD (Frizzled) at the plasma membrane interface with the extracellular environment (Fig. 15.3c). FZD receptors transduce a signal to Disheveled (Dvl) and Dvl subsequently dephosphorylates an associated protein Axin. Axin functions as a signaling scaffold protein coordinating the interactions of Adenomatous Polyposis Coli (APC), glycogen synthase kinase 3β (GSK3β), β-catenin, and Conductin (Fig. 15.3c). The coordination of these proteins by Axin facilitates the phosphorylation of β-catenin and APC by GSK3β. The dephosphorylation of Axin diminishes its capacity to coordinate β-catenin in complex with GSK3β causing decreased phosphorylation of β-catenin (Fig. 15.3c). The phosphorylation of β-catenin mediates subsequent ubiquitylation and degradation, but without phosphorylation by GSK3β, β-catenin accumulates in the cytoplasm. Accumulation of β-catenin results in nuclear translocation of the protein and interaction with lymphoid enhancer binding factor 1/T-cell factor (LEF1/TCF) transcription factors and transcription of β-catenin target genes, such as c-MYC, c-Jun and fra-1, in addition to EMT important urokinase type plasminogen activator receptor (uPAR), matrix metalloproteinases and cyclin D1 [140–144]. AR and β-catenin interact directly with one another (Fig. 15.3c), impacting the EMT outcome [145]. In vitro androgen-stimulated transcriptional responses are enhanced by functional involvement of Wnt signaling, consequently opposing the effects of antagonistic anti-androgenic treatment (bicalutamide) [146]. Together, these data reveal that β-catenin acts as a coactivator of AR gene target transcription and thereby associated with progression to CRPC under conditions of overexpression [140]. Furthermore, cognate ligand-induced AR signaling possesses the capacity to attenuate Wnt signaling and TCF/LEF1-dependent gene transcription.
The pioneering work of Arul Chinnaiyan’s discovery of TMPRSS2: ERG gene fusion has been paramount in advancing our molecular understanding of prostate cancer. These gene fusions result in androgen-driven expression of the transcription factor ERG. The consequences of these fusions on cell fate are diverse and intriguing, but an important observation that ERG fusion-positive tumors and Frizzled4 (Fzd4: 7 pass transmembrane receptor of Wnt signaling pathway) cooverexpression were consistently identified in clinical prostate cancer [147]. Moreover, overexpression of ERG induced the EMT phenomenon in androgen-responsive cell lines (VCaP), including repression of E-cadherin and induction of N-cadherin [147]. The effects of ERG overexpression could be abrogated by the modulation of FZD4, demonstrating that FZD4 was both necessary and sufficient to mediate the oncogenic effects of ERG overexpression and defining the impact of direct crosstalk of AR-driven ERG overexpression with the Wnt signaling on prostate cancer EMT [147].
15.3.4 The Star Power of AR Partner: Transforming Growth Factor-β
EMT induction is characteristically associated with Transforming Growth Factor-β (TGF-β) signaling and its cooperation with oncogenic Ras or receptor tyrosine kinases (RTKs) is commonly associated with growth factor receptor to induce EMTs and subsequent metastasis [103, 148]. TGF-β is a ubiquitously expressed growth inhibitory cytokine [149–152]. TGF-β contributes to tissue and organ homeostasis by inducing a system of proliferative versus apoptotic balances [149, 150]. TGF-β signaling is critical in diverse cell types by impacting important features of cellular behavior including migration, adhesion, alterations to the extracellular environment, apoptosis, and promoting formation of osteoblastic metastatic lesions [149, 151, 153]. The TGF-β pathway traditionally engages signaling involving the SMAD proteins (Fig. 15.3b) [149, 151, 153–155]. TGF-β signaling is mediated by the Serine/Threonine Kinase domains of the TGFβRI and TGFβRII receptors and the formation of hetero-tetrameric complexes (Fig. 15.3b) [155]. Binding to TGF-β causes TβRII receptor to phosphorylate the regulatory GS domain of TβRI, initiating a downstream signaling cascade mediated by SMAD proteins [153, 155]. TβRI selectively phosphorylates regulatory SMADs (R-SMADs) at the SSXS motif on the carboxyl terminus of the SMAD [149, 153]. The R-SMADs, SMAD2, and SMAD3, activated by the TβRI [149], are sequestered in the cytoplasm via their interactions with SMAD anchor for receptor activation (SARA) [149]. Once activated by TβRI, R-SMADs lose affinity for SARA and become free to interact with SMAD4 [149]. SMAD4 is essential for formation of SMAD-mediated transcriptional complexes, components of which are continuously shuttled between the cytoplasm and nucleus via nuclear pores [149, 150, 153]. The SMAD complex dictates transcriptional activation, via recruitment of coactivators such as p300, CBP, or SMIF. Conversely, for transcriptional repression, the SMAD complex recruits p107, SKI, SNON, TGIF, EVI1, and ZEB2 (SIP1) [149, 156]. Expression of these coregulators is dependent on cell type, developmental stage, and microenvironment-hosted crosstalk facilitating a broad cellular response repertoire [149]. Defective/lost TGF-β receptors and SMAD mutations are not directly responsible for the effects of EMT in cancer progression [151]; rather, loss of apoptotic response occurs in cancer cells despite production of TGF-β ligand [157].
Smad-independent signaling proceeds via MAPK pathways, involving activation of Erk, JNK, and p38 MAPK signaling pathways by TGF-β. Oncogenic Ras contributes to the activation of Erk/MAPK signaling, in a context-dependent manner. TGF-β activates TGF-β-activated Kinase 1 (TAK1), a MAPK kinase kinase family member (MAPKKK), leading to activation of JNK and p38 MAPK. TAK1 can also phosphorylate IκB, thereby activating NFκB signaling [153]. Direct mechanistic link of EMT to cancer progression is mediated by the effect TGF-β signaling on activation of Rho A (Fig. 15.3b). Rho A and p160ROCK (effector kinase) activation in conjunction with activation of Cdc24, p38, MAPK, and Smad signaling, correlate with stress fiber formation, membrane ruffling, lamellipodia formation and the physical mechanisms of EMT [153]. Rho A is upregulated in prostate cancer cells as compared to the benign prostate and this elevated expression is linked to aggressive disease and diminished disease-free survival in patients after radical prostatectomy [158]. In fact, Rho A activation by TGF-β is similarly activated by action of AR on Serum Response Factor target genes further corroborating the crosstalk between TGF-β and AR [158], in the context of EMT cellular “landscaping.” Elevated TGF-β correlates with increasing tumor grade in numerous human malignancies, including prostate cancer [159–162]. And furthermore, overexpression of TGF-β ligand is detected in advanced prostate cancer [150, 153, 154]. TGF-β ligand binds to and induces phosphorylation of TβRI by TβRII resulting in SMAD signaling in prostate cancer cells. SMADs 3 and 4 serve as transcriptional coregulators of AR target genes and conversely, ligand-bound AR transcriptionally modulates SMAD3 in prostate cancer [163, 164]. SMAD4 (alone or in conjunction with SMAD3) can coregulate AR transactivation via binding to the DBD and LBD domains of the steroid receptor thereby modulating its DHT-induced activity [151, 152]. SMAD3 can bind AR as well, but this interaction is mediated by the NTD [165]. In a mechanistic twist, AR overexpression enables prostate cancer cells to overcome the growth inhibitory effects of TGF-β under DHT deprived conditions [164]. Moreover, expression of SMAD3 enhances AR-mediated transactivation, whilst co-overexpression of SMAD3 and 4 repressed AR transactivation [166]. Our group has pursued the impact of dysfunctional TGF-β signaling in functional interaction with AR signaling in vitro and in vivo models of prostate cancer. The TGF-β/Smad signaling pathway elicits a downstream activation in Snail thereby repressing E-cadherin expression in a number of cancer cell types [167, 168]. In LNCaP TβRII human prostate cancer cells, DHT (alone or in combination with TGF-β) significantly induced Snail expression [152], pointing to a dynamic crosstalk between the AR and TGF-β pathways in control of EMT. Recent studies identified a role for Hexim-1 in mediating such a crosstalk between AR and TGF-β in prostate cancer progression. Hexim-1 is an inhibitor of cyclin-dependent kinase 9 (Cdk9) of transcription elongation factor (pTEFb) complex, which is upregulated and translocated to the cytoplasm during tumor progression [169]. Cdk9 interacts with AR and phosphorylates the AR at serine 81 [170] and transcriptionally programs Smads 1 and 3 via phosphorylation of linker region [171, 172]. Such refined mechanistic control of Hexim-1 expression supports its role as a converging modifier of activity for AR and TGF-β signaling crosstalk towards EMT [169].
15.3.5 Notch (Hi)-Jagged AR in Metastatic CRPC
Notch signaling is fundamentally significant in development and tissue homeostasis. Notch signaling facilitates an important mode of cell–cell communication. Notch proteins (1–4) are type I, single pass transmembrane receptors [173]. The extracellular domain of the Notch protein participates in ligand binding and is composed of a variable number of epidermal growth factor (EGF)-like domains (essential for ligand binding) and three cysteine-rich LIN12/Notch repeats (LNR) (ensure signaling only transduced in the presence of ligand) [173, 174]. The intracellular domains of the Notch receptor include RAM23 domain, six ankyrin/cdc10 repeats, two nuclear localization signals, transcriptional activation domain, and a PEST sequence [173]. The ligands recognized by the Notch receptor are Delta 1,3, and 4 as well as Jagged 1 and 2; these ligands are membrane bound and composed of an amino-terminal domain known as DSL and variable number of EGF-like repeats [175–179]. The Jagged ligands possess a cysteine-rich (CR) domain [173] and ligand receptor-initiated signaling cascade results in cleavage of the Notch receptor and ultimately translocation of the Notch intracellular domain (NICD) to the nucleus. There is growing evidence identifying Notch signaling as characteristic component of EMT. As discussed above, Snail1 is a transcription factor responsible for repressing E-cadherin transcription, with Notch1 activation upstream of Snail1 [173]. This observation has been further validated in the immortalized porcine aortic endothelial cell line, whereby overexpression of NICD induced an EMT via activation of Snail1 and subsequent repression of E-cadherin [180]. The correlation between expression of Notch ligand, Jagged1, and high grade and metastatic prostate cancer compared to localized prostate cancer [181] is of major translational value as Jagged1 may serve as an independent prognostic indicator of prostate cancer recurrence and progression [181], potentially driven by a link with androgenic signaling [181, 182]. Notch1 signaling is associated with osteoblast differentiation and Notch1 expression is markedly elevated in osteoblast skeletal-derived prostate cancer cells [182], validating the role of this EMT promoting pathway in prostate cancer metastasis to the bone.
15.4 Conclusions
The AR acts as a cornerstone of the aberrant signaling mechanisms associated with prostate cancer. Intense pursuit of the anomalous pathways via which androgen signaling is perpetuated in CRPC has identified “diverting” mechanisms that still impact tumor progression and therapeutic response in patients. The androgenic signaling axis can become altered in a number of ways: point mutations, truncations, variant expression of the AR itself, posttranslational modifications deviating from the normal signaling by RTKs and downstream of growth factor signaling pathways, and the ability of prostate cancer cells to commandeer androgen synthesis in the face of ADT. In close exchanges directed by AR, EMT can be reactivated in prostate cancer epithelial cells by the key signaling controllers of prostate growth and their functional interactions (TGF-β and androgen axis/AR), towards metastatic behavior. Thus unfolding the key players in EMT-activating signaling pathways engaged in crosstalk with AR signaling is paramount to recognizing potential therapeutic targets for CRPC. The landscape becomes progressively defined: Loss of E-cadherin expression and induction of N-cadherin are regulated by key transcription factors, Snail and Slug, which transcriptionally repress E-cadherin via the androgenic signaling axis. In a more prominent role, Zeb1 directly recruited by the AR signaling, engages in a bidirectional negative feedback loop, highlighted in ADT. In the absence/repression of AR (as in early ADT), Zeb1 is overexpressed facilitating the mechanistic events leading to EMT. Also impacted by the androgenic status, β-catenin, accumulates in the cytoplasm and translocates to the nucleus, to induce transcription of LEF1/TCF genes and others which mediate EMT processes. Interestingly, β- catenin can also interact with AR directly and act as a transcriptional coactivator of AR driving not only EMT but also progression to CRPC.
In a less direct crosstalk event, AR drives overexpression of TMPRSS2: ERG genes fusion products resulting in highly overexpressed transcription factor ERG (ETS family of transcription factors). At the clinical setting this overexpression of ERG and FZD is associated with prostate tumor progression. At the cellular level, elevated ERG induces EMT, an effect that can be abrogated with silencing of FZD, thus implicating the Wnt signaling pathway in driving the effects of ERG gene fusions. In view of the documented significant association between elevated TGF-β ligand and increasing prostate tumor grade, a dynamic crosstalk of TGF-β signaling with AR, in controlling EMT during progression to metastasis, becomes central to the cellular landscape of CRPC development. Moreover, Smads3 and 4 interact directly with AR to reciprocally modulate both target gene transcriptional activation and expression. Androgen treatment of human prostate cancer cells significantly upregulates Snail and promotes the TGF-β and AR interaction in controlling EMT. Notch signaling is essential to intercellular communication, and expression of Jagged1 (main effector) emerges as a potential independent prognostic indicator of prostate cancer recurrence and progression, since expression of Jagged1 correlates with high grade and metastatic prostate cancer compared to benign disease or localized tumors. Moreover Jagged1 bypasses AR in prostate cancer metastasis, and Notch1 signaling is functionally involved with osteoblast differentiation in skeletal-derived prostate cancer cells. As our understanding of the role of AR signaling in navigating EMT towards prostate cancer metastasis and CRPC expands, so do the opportunities to exploit the interactions of AR with lead partners, in pursuit of novel therapeutic targets and prognostic indicators of disease progression.
Abbreviations
- CRPC:
-
Castration-resistant prostate cancer
- ADT:
-
Androgen deprivation therapy
- EMT:
-
Epithelial–mesenchymal transition
- TGF-β:
-
Transforming growth factor-β
- DHT:
-
Dihydrotestosterone
- ARE:
-
Androgen-responsive elements
- PSA:
-
Prostate-specific antigen
References
Huggins C, Hodges CV (1941) Studies on prostatic cancer. I. The effect of castration, of estrogen and of androgen injection on serum phosphatase in metastatic carcinoma of the prostate. Cancer Res 1:293–297
Freedland SJ, Moul JW (2007) Prostate specific antigen recurrence after definitive therapy. J Urol 177(6):1985–1991
Hu R, Denmeade SR, Luo J (2010) Molecular processes leading to aberrant androgen receptor signaling and castration resistance in prostate cancer. Expert Rev Endocrinol Metab 5(5):753–764
Chen CD, Welsbie DS, Tran C, Baek SH, Chen R, Vessella R, Rosenfeld MG, Sawyers CL (2004) Molecular determinants of resistance to antiandrogen therapy. Nat Med 10(1):33–39
Feldman BJ, Feldman D (2001) The development of androgen-independent prostate cancer. Nat Rev 1:34–45
Knudsen KE, Penning T (2010) Partners in crime: deregulation of AR activity and androgen synthesis in prostate cancer. Trends Endocrinol Metab 21(5):315–324
Matuszak EA, Kyprianou N (2011) Androgen regulation of epithelial-mesenchymal transition in prostate tumorigenesis. Expert Rev Endocrinol Metab 6(3):469–482
Gelmann EP (2002) Molecular biology of the androgen receptor. J Clin Oncol 13:3001–3015
Lonergan PE, Tindall DJ (2011) Androgen receptor signaling in prostate cancer development and progression. J Carcinog 10(20):1–12
Schmidt LJ, Tindall DJ (2011) Steroid 5 alpha reductase inhibitors targeting BPH and prostate cancer. J Steroid Biochem Mol Biol 125:32–38
Wilson JD (2001) The role of 5 alpha-reduction in steroid hormone physiology. Reprod Fertil Dev 13:673–678
Brinkmann AO, Blok LJ, de Ruiter PE, Doesburg P, Steketee K, Berrevoets CA, Trapman J (1999) Mechanisms of androgen receptor activation and function. J Steroid Biochem Mol Biol 69(1):307–313
Nazareth LV, Weigel NL (1996) Activation of the human androgen receptor through a protein kinase A signaling pathway. J Biol Chem 271:19900–19907
Feng J, Zheng SL, Wennuan L, Isaacs WB, Xu J (2011) Androgen receptor signaling in prostate cancer: new twists for an old pathway. Steroids Horm Sci S2:1–7
Heinlein CA, Chang C (2002) Androgen receptor (AR) coregulators: an overview. Endocr Rev 23:175–200
Roy AK, Lavrosky Y, Song CS (1999) Regulations of androgen action. Vitam Horm 55:309–352
Jenster G, van der Korput HAGM, Trapman J, Brinkmann AO (1995) Identification of two transcription activation units in the N-terminal domain of the human androgen receptor. J Biol Chem 270(13):7341–7346
Dehm SM, Regan KM, Schmidt LJ, Tindall DJ (1989) Selective role for an NH2-terminal WxxLF motfi for aberrant androgen receptor activation in androgen depletion independent prostate cancer cells. Cancer Res 67:10067–10077
Simental JA, Sar M, Lane MV, French FS, Wilson EM (1991) Transcriptional activation and nuclear targeting signals of the human androgen receptor. J Biol Chem 266(1):510–518
Umesono K, Evans RM (1989) Determinants of target gene specificity for steroid/thyroid hormone receptors. Cell 57:1139–1146
van Royen ME, van Cappellen WA, de Vos C, Houtsmuller AB, Trapman J (2012) Stepwise androgen receptor dimerization. J Cell Sci 125:1970–9
Zhou ZX, Sar M, Simental JA, Lane MV, Wilson EM (1994) A ligand dependent bipartite nuclear targeting signal in the human androgen receptor. Requirement for the DNA-binding domain and modulation by the NH2 terminal and carboxyl-terminal sequences. J Biol Chem 269(18):13115–13123
Haelens A, Tanner T, Denayer S, Callewaert L, Claessens F (2007) The hinge region regulates DNA binding, nuclear translocation, and transactivation of the androgen receptor. Cancer Res 67(9):4514–4523
Robinson-Rechavi M, Escriva GH, Laudet V (2003) The nuclear receptor superfamily. J Cell Sci 116:585–586
Ozanne DM, Brady ME, Cook S, Gaughan L, Neal DE, Robson CN (2000) Androgen receptor nuclear translocation is facilitated by the f-actin cross linking protein filamin. Mol Endocrinol 14:1618–1626
McKenna NJ, Lanz RB, O’Malley BW (1999) Nuclear receptor coregulators: cellular and molecular biology. Endocr Rev 20:321–344
Poukka H, Karvonen U, Yoshikawa N, Tanaka H, Palvimo JJ, Janne OA (2000) The RING finger protein SNURF modulates nuclear trafficking of the androgen receptor. J Cell Sci 113:2991–3001
Pratt WB, Toft DO (1997) Steroid receptor interactions with heat shock protein and immunophilin chaperones. Endocr Rev 18:306–360
Xu L, Glass CK, Rosenfeld MG (1999) Coactivator and corepressor complexes in nuclear receptor function. Curr Opin Genet Dev 9:140–147
Heery DM, Kalkhoven E, Hoare S, Parker MG (1997) A signature motif in transcriptional co-activators mediates binding to nuclear receptors. Nature 387:733–736
Chan SC, Li Y, Dehm SM (2012) Androgen receptor splice variants activate AR target genes and support aberrant prostate cancer cell growth independent of the canonical AR nuclear localization signal. J Biol Chem 287:19736–49
Black BE, Paschal BM (2004) Intranuclear organization and function of the androgen receptor. Trends Endocrinol Metab 15:411–417
Brodsky AS, Silver PA (1999) Nuclear transport HEATs up. Nat Cell Biol 1:E66–E67
Corbett AH, Silver PA (1997) Nucleocytoplasmic transport of macromolecules. Microbiol Mol Biol Rev 61:193–211
Cutress ML, Whitaker HC, Mills IG, Stewart M, Neal DE (2008) Structural basis for the nuclear import of the human androgen receptor. J Cell Sci 121:957–968
Gorlich D (1997) Nuclear protein import. Curr Opin Cell Biol 9:412–419
Nigg EA (1997) Nucleocytoplasmic transport: signals, mechanisms, and regulation. Nature 386:779–787
Picard D, Yamamoto KR (1987) Two signals mediate hormone-dependent nuclear localization of the glucocorticoid receptor. EMBO J 6:3333–3340
Savory JGA, Hsu B, Laquian IR, Giffin W, Reich T, Hache RJG, Lefebvre YA (1999) Discrimination between NL1- and NL2- mediated nuclear localization of the glucocorticoid receptor. Mol Cell Biol 19:1025–1037
Loy CJ, Sim KS, Yong EL (2003) Filamin-A fragment localizes to the nucleus to regulate androgen recepto and coactivator functions. Proc Natl Acad Sci USA 100(8):4562–4567
Koteliansky VE, Shirinsky V, Gneushev GN, Smirnov VN (1981) Filamin, a relative high molecular mass actin-binding protein from smooth muscles, promotes actin polymerization. FEBS Lett 136:98–100
Darshan MS, Loftus MS, Thadani-Mulero M, Levy BP, Escuin DE, Zhou XK, Gjurezi A, Chanel-Vos C, Shen R, Tagawa ST, Bander NH, Nanus DM, Giannakakou P (2011) Taxane-induced blockade to nuclear accumulation of the androgen receptor predicts clinical responses in metastatic prostate cancer. Cancer Res 15:6019–6029
Heemers HV, Tindall DJ (2007) Androgen receptor (AR) coregulators: a diversity of functions converging on and regulating the AR transcriptional complex. Endocr Rev 28(7):778–808
Schaufele F, Carbonell X, Guerbadot M, Borngraeber S, Chapman MS, Ma AAK, Miner JN, Diamond MI (2005) The structural basis of androgen receptor activation: intramolecular and intermolecular amino-carboxy interactions. Proc Natl Acad Sci USA 102:9802–9807
Van Royen ME, Cunha SM, Brink MC, Mattern KA, Nigg AL, Dubbink HJ, Verschure PJ, Trapman J, Houtsmuller AB (2007) Compartmentalization of androgen receptor protein–protein interactions in living cells. J Cell Biol 177:63–72
Gregory CW, Raymond TJ, Mohler JL, French FS, Wilson EM (2001) Androgen receptor stabilization in recurrent prostate cancer is associated with hypersenstivity to low androgen. Cancer Res 61:2892–2898
Marcelli M, Ittmann M, Mariani S, Sutherland R, Nigam R, Murthy L, Zhao Y, DiConcini D, Puxeddu E, Esen A, Eastham J, Weigel NL, Lamb DJ (2000) Androgen receptor mutations in prostate cancer. Cancer Res 60:944–951
Taplin ME, Bubley GJ, Ko Y-J, Small EJ, Upton MP, Rajeshkumar BR, Balk SP (2001) Selection for androgen receptor mutations in prostate cancers treated with androgen antagonist. Cancer Res 59:2511–2515
Tilley WD, Buchanan G, Hickey TE, Bentel JM (1996) Mutations in the androgen receptor gene are associated with progression of human prostate cancer to androgen independence. Clin Cancer Res 2:277–285
Dehm SM, Schmidt LJ, Heemers HV, Vessella RL, Tindall DJ (2008) Splicing of a novel androgen receptor exon generates a constitutively active androgen receptor that mediates prostate cancer therapy resistance. Cancer Res 68:5469–5477
Guo Z, Yang X, Sun F, Jiang R, Linn DE, Chen H, Chen H, Kong X, Melamed J, Tepper CG, Kung H-J, Brodie AMH, Edwards J, Qiu Y (2009) A novel androgen receptor splice variant is upregulated during prostate cancer progression and promotes androgen-depletion-resistant growth. Cancer Res 69(6):2305–2313
Hu R, Dunn TA, Wei S, Isharwal S, Veltri RW, Humphreys E, Han M, Partin AW, Vessella RL, Isaacs WB, Bova GS, Luo J (2009) Ligand independent androgen receptor variants derived from splicing of cryptic exons signify hormone refractory prostate cancer. Cancer Res 69(1):16–22
Hu R, Isaacs WB, Luo J (2010) A snapshot of the expression signature of androgen receptor splicing variants and their distinctive transcriptional activities. Prostate 71(15):1656–1667
Sun S, Sprenger CCT, Vessella RL, Haugk K, Soriano K, Mostaghel EA, Page ST, Coleman IM, Nguyen HM, Sun H, Nelson PS, Plymate SR (2010) Castration resistance in human prostate cancer is conferred by a frequently occurring androgen receptor splice variant. J Clin Invest 120(8):2715–2730
Craft N, Shostak Y, Carey M, Sawyers CL (1999) A mechanism for hormone-independent prostate cancer through modulation of androgen receptor signaling by the Her-2/neu tyrosine kinase. Nat Med 5:280–285
Culig Z, Hobisch A, Cronauer MV, Radmayr C, Trapman J, Hattmair A, Bartsch G, Klocker H (1994) Androgen receptor activation in prostatic tumor cell lines by insulin-like growth factor-I, kertinocyte growth factor, and epidermal growth factor. Cancer Res 54:5474–5478
Li J, Yen C, Liaw D, Podsypanina K, Bose S, Wang SI, Puc J, Miliaresis C, Rodgers L, McCombie R, Bigner SH, Giovanella BC, Ittmann M, Tycko B, Hibshoosh H, Wigler MH, Parsons R (1997) PTEN, a putative protein tyrosine phosphatase gene mutated in human brain, breast and prostate cancer. Science 275:1943–1947
Locke J, Guns ES, Lubik AA, Adomat HH, Hendy SC, Wood CA, Ettinger SI, Gleave ME, Nelson CC (2008) Androgen levels increase by intratumoral de novo steroidogenesis during the progression of castration-resistant prostate cancer. Cancer Res 68:6407–6414
Montgomery RBMEA, Vessella R, Hess DL, Kalhorn TF, Higano CS, True LD, Nelson PS (2008) Maintenance of intratumoral androgens in metastatic prostate cancer: a mechanism for castration resistant tumor growth. Cancer Res 68:4447–4454
Stanbrough M, Bubley GJ, Ross K, Golub TR, Rubin MA, Penning TM, Febbo PG, Balk SP (2006) Increased expression of genes converting adrenal androgens to testosterone in androgen-independent prostate cancer. Cancer Res 66:2815–2825
Colombel M, Symmans F, Gil S, O’Toole KM, Chopin D, Benson M, Olsson CA, Korsmeyer S, Buttyan R (1993) Detection of the apoptosis-suppressing oncoprotein bcl-2 in hormone-refractory human prostate cancer. Am J Pathol 143(8):390–400
Liu AY, Corey E, Bladou F, Lange PH, Vessella RL (1996) Prostatic cell lineage markers: emergence of Bcl2+ cells of human prostate cancer xenograft LuCaP23 following castration. Int J Cancer 65:85–89
Huizing MT, Misser VHS, Pieters RC, ten Bokkel Huinink WW, Veenhof CHN, Vermorken JB, Pinedo HM, Beijnen JH (1995) Taxanes: a new class of antitumor agents. Cancer Invest 13(4):381–404
Kraus LA, Samuel SK, Schmid SM, Dykes DJ, Waud WR, Bissery MC (2003) The mechanism of action of docetaxel (Taxotere) in xenograft models is not limited to bcl-2 phosphorylation. Invest New Drugs 21:259–268
Bruckheimer EM, Kyprianou N (2001) Dihydrotestosterone enhances transforming growth factor beta induced apoptosis in hormone sensitive prostate cancer cells. Endocrinology 142:2419–2426
Bruckheimer EM, Kyprianou N (2002) BCL-2 antagonizes the combined apoptotic effect of transforming growth factor-beta and dihydrotestosterone in prostate cancer cells. Prostate 53:133–142
Debes JD, Tindall DJ (2004) Mechanisms of androgen refractory prostate cancer. N Engl J Med 351:1488–1490
Oliver CL, Miranda MB, Shangary S, Land S, Wang S, Johnson DE (2005) (−−)—Gossypol acts directly on the mitochondria to overcome Bcl-2 and Bcl-X(L) mediated apoptosis resistance. Mol Cancer Ther 4:23–31
Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, Oudard S, Theodore C, James ND, Turesson I, Rosenthal MA, Eisenberger MA (2004) Docetaxel plus prednisone or mitoxantrone and prednisone for advanced prostate cancer. N Engl J Med 351:1502–1512
Berthold DR, Pond GR, Soban F, de Wit R, Eisenberger M, Tannock IF (2008) Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: updated survival in the TAX 327 study. J Clin Oncol 26:242–245
Petrylak DP, Tangen CM, Hussain MH, Lara PN, Jones JA, Taplin ME, Burch PA, Berry D, Moinpour C, Kohli M, Benson MC, Small EJ, Raghavan D, Crawford ED (2004) Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med 351:1513–1520
Zhu M-L, Horbinski CM, Garzotto M, Qian DZ, Beer TM, Kyprianou N (2010) Tubulin-targeting chemotherapy impairs androgen recepto activity in prostate cancer. Cancer Res 70(20):7992–8002
Abdulla A, Kapoor A (2011) Emerging novel therapies in the treatment of castrate-resistant prostate cancer. CUAJ 5(2):120–133
Attard G, Greystroke A, Kaye S, De Bono J (2006) Update on tubulin targeting agents. Pathol Biol (Paris) 54:72–84
Sartor AO (2011) Progression of metastatic castrate-resistant prostate cancer: impact of therapeutic inervention in the post-docetaxel space. J Hematol Oncol 4(18):1–7
Galsky MD, Dritselis A, Kirkpatrick P, Oh WK (2010) Cabazitaxel. Nat Rev Drug Discov 9:677–678
Di Lorenzo G, Buonerba C, De Placido S, Sternberg CN (2010) Castration-resistant prostate cancer: current and emerging treatment strategies. Drugs 70(8):983–1000
De Bono JS, Oudard S, Ozguroglu M, Hansen S, Machiels JP, Kocak I, Gravis G, Bodrogi I, Mackenzie MJ, Shen L, Roessner M, Gupta S, Sartor AO (2010) Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet 376:1147–1154
Walcak JR, Carducci MA (2007) Prostate cancer: a practical approach to current management of recurrent disease. Mayo Clin Proc 82:243–249
De Bono JS, Logothetis CJ, Fizazi K, North S, Chu L, Chi KN, Kheoh T, Haqq C, Molina A, Scher HI (2010) Abiraterone acetate (AA) plus low dose prednisone (P) improves overall survival in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC) who have progressed after docetaxel-based chemotherapy (chemo): Results of COU-AA-301 [abstract]. In: Presidential symposium at ESMO, Milan, Italy
Shen HC, Balk SP (2009) Development of androgen recepto antagonists with promising activing in castration-resistant prostate cancer. Cancer Cell 15(6):461–463
Scher HI, Beer TM, Higano CS, Anand A, Taplin ME, Efstanthiou E, Ratjkopf D, Shelkey J, Yu EY, Alumkal J, Hung D, Hirmand M, Seely L, Morris MJ, Danila DC, Humm J, Larson S, Fleisher M, Sawyers CL (2010) Antitumor activity of MDV3100 in castration resistant prostate cancer: a phase 1–2 study. Lancet 375:1437–1446
Vishnu P, Tan WW (2010) Update on option for treatment of metastatic castration-resistant prostate cancer. Onco Targets Ther 3:39–51
Attard G, Cooper CS, de Bono JS (2009) Steroid hormone receptors in prostate cancer: a hard habit to break? Cancer Cell 16:458–462
Tran C, Ouk S, Clegg NJ, Chen Y, Watson PA, Arora V, Wongvipat J, Smith-Jones PM, Yoo D, Kwon A, Wasielewska T, Welsbie D, Chen CD, Higano CS, Beer TM, Hung DT, Scher HI, Jung ME, Sawyers CL (2009) Development of a second-generation antiandrogen for treatment of advanced prostate cancer. Science 324:787–790
Watson PA, Chen YF, Balbas MD, Wongvipat J, Socci ND, Viale A, Kim K, Sawyers CL (2010) Constitutively active androgen receptor splice variants expressed in castration-resistant prostate cancer require full length androgen receptor. Proc Natl Acad Sci USA 107:16759–16765
Massard C, Fizazi K (2011) Targeting continued androgen receptor signaling in prostate cancer. Clin Cancer Res 17(12):3876–3883
Ferte C, Andre F, Soria JC (2010) Molecular circuits of solid tumors: prognostic and predictive tools for bedside use. Nat Rev Clin Oncol 7:367–380
Bolton EC, So AY, Chaivorapol C, Haqq CM, Li H, Yamamoto KR (2007) Cell- and gene- specific regulation of primary target genes by the androgn receptor. Genes Dev 21:2005–2017
Holzbeierlein J, Lal P, LaTulippe E, Smith A, Satagopan J, Zhang L, Ryan C, Smith S, Scher H, Scardino P, Reuter V, Gerald WL (2004) Gene expression analysis of human prostate carcinoma during hormonal therapy identifies androgen responsive-genes and mechansims of therapy resistance. Am J Pathol 164(1):217–227
Vellaichamy A, Dezso Z, JeBailey L, Chinnaiyan AM, Sreekumar A, Nesvizhskii AI, Omenn GS, Bugrim A (2010) “Topological significance” analysis of gene expression and proteomic profiles from prostate camcer cells reveal key mechanisms of androgen response. PLoS One 5(6):1–10
Greenburg G, Hay ED (1982) Epithelia suspended in collagen gels can lose polarity and express characteristics of migrating mesenchymal cells. J Cell Biol 95(1):333–339
Yilmaz M, Christofori G (2009) EMT, the cytoskeleton, and cancer cell invasion. Cancer Metastasis Rev 28:15–33
Kalluri R, Weinberg RA (2009) The basics of epithelial-mesenchymal transition. J Clin Invest 119(6):1420–1428
Acloque H, Adams MS, Fishwick K, Bronner-Fraser M, Nieto MA (2009) Epithelial-mesenchymal transitions: the importance of changing cell state in development and disease. J Clin Invest 119(6):1438–1449
Barrallo-Gimeno A, Nieto MA (2005) The Snail genes act as inducers of cell movement and survival: implications in development and cancer. Development 132:3151–3161
Moreno-Bueno G, Portillo F, Cano A (2008) Transcriptional regulation of cell polarity in EMT and cancer. Oncogene 27:6958–6969
Peindao H, Olmeda D, Cano A (2007) Snail, Zeb, bHLH factors in tumor progression: an alliance against the epithelial phenotype? Nat Rev Cancer 7:415–428
Kalluri R (2009) EMT: when epithelial cells decide to become mesenchymal-like cells. J Clin Invest 119(6):1417–1419
Thiery JP, Acloque H, Huang RY, Nieto MA (2009) Epithelial-mesenchymal transitions in development and disease. Cell 139(5):871–890
Yang J, Weinberg R (2008) Epithelial-mesenchymal transition: at the crossroads of development and tumor metastasis. Dev Cell 14(6):818–829
Haraguchi M, Okubo T, Miyashita Y, Miyamoto Y, Hayashi M, Crotti TN, McHugh KP, Ozawa M (2008) Snail regulates cell-matrix adhesion by regulation of the expression of integrins and basement membrane proteins. J Biol Chem 283:23514–23523
Huber MA, Kraut N, Beug H (2005) Molecular requirements for epithelial-mesenchymal transition during tumor progression. Curr Opin Cell Biol 17:548–558
Zhu M-L, Kyprianou N (2010) Role of androgens and the androgen receptor in epithelial-mesenchymal transition and invasion of prostate cancer cells. FASEB J 24:769–777
Sun Y, Wang B-E, Leong KG, Yue P, Li L, Jhunjhunwala S, Chen D, Seo K, Modrusan Z, Gao W-Q, Settleman J, Johnson L (2011) Androgen deprivation causes epithelial-mesenchymal transtition in the prostate: Implications for androgen-deprivation therapy. Cancer Res 72(2):527–536
Tanaka H, Kono E, Tran CP, Miyazaki H, Yamashiro J, Shimomura T (2010) Monoclonal antibody targeting of N-Cadherin inhibits prostate cancer growth, metastasis, and castration resistance. Nat Med 16:1414–1420
Nelson WJ, Nusse R (2004) Convergence of Wnt, beta-catenin, and cadherin pathways. Science 303(5663):1483–1487. doi:10.1126/science.1094291
Thiery JP (2002) Epithelial-mesenchymal transition in tumour progression. Nat Rev Cancer 2:442–454
Thiery JP (2003) Epithelial -mesenchymal transitions in development and pathologies. Curr Opin Cell Biol 15:740–746
Harris TJ, Tepass U (2010) Adherens junctions: from molecules to morphogenesis. Rev Mol Cell Bio 11(7):502–514
Gravdal K, Halvorsen OJ, Haukaas SA, Akslen LA (2007) A switch from E-cadherin to N-cadherin expression indicates epithelial to mesenchymal transition and is of strong and independent importance for the progress of prostate cancer. Clin Cancer Res 13(23):7003–7011
Jeanes A, Gottardi CJ, Yap AS (2008) Cadherins and cancer: how does cadherin dysfunction promote tumour progression? Oncogene 27(55):6920–6929
Baritaki S, Chapman A, Yeung K, Spandidos DA, Palladino M, Bonavida B (2009) Inhibition of epithelial to mesenchymal transition in metastatic prostate cancer cells by the novel proteasome inhibitor, NPI-0052: pivotal roles of Snail repression and RKIP induction. Oncogene 28:3573–3585
Liu YN, Liu Y, Lee HJ, Hsu YH, Chen JH (2008) Activated androgen receptor downregulates E-cadherin gene expression and promotes tumor metastasis. Mol Cell Biol 28(23):7096–7108
Anose BM, Sanders MM (2011) Androgen receptor regulates transcription of the ZEB1 transcription factor. Int J Endocrinol 2011:1–10
Brabletz S, Brabletz T (2010) The ZEB/miR-200 feedback loop-a motor of cellular plasticity in development and cancer? EMBO Rep 11(9):670–677
Hidaka T, Nakahata S, Hatakeyama K (2008) Down regulation of TCF8 is involved in leukemogenesis of adult T-cell leukemia lymphoma. Blood 112(2):383–393
Saykally JN, Dogan MP, Cleary MP, Sanders MM (2009) The ZEB1 transcription factor is a novel repressor of adiposity in female mice. PLoS One 4(12):1–12
Drake JM, Strohbehn G, Bair TB, Moreland JG, Henry MD (2009) ZEB1 enhances transendothelial migration and represses the epithelial phenotype of prostate cancer cells. Mol Biol Cell 20:2207–2217
Spaderna S, Schmalhofer O, Wahlbuhl M, Dimmler A, Bauer K, Sultan A, Hlubek F, Jung A, Strand D, Eger A, Kirchner T, Behrens J, Brabletz T (2008) The transcriptional repressor ZEB1 promoters metastasis and loss of cell polarity in cancer. Cancer Res 68:537–544
Comijn J, Berx G, Vermassen P, Verschueren K, van Grunsven L, Bruyneel E, Mareel M, Huylebroeck D, van Roy F (2001) The two handed E box binding zinc finger protein SIP1 downregulates E-cadherin and induces invasion. Mol Cell 7:1267–1278
Chamberlain EM, Sanders MM (1999) Identification of the novel player delta EF1 in estrogen transcriptional cascades. Mol Cell Biol 19(5):3600–3606
Richer JK, Jacobsen BM, Manning NG, Abel MG, Wolf DM, Horwitz KB (2002) Differential gene regulation by the two progesterone receptor isoforms in human breast cancer cells. J Biol Chem 277(7):5209–5218
Graham TR, Yacoub R, Taliafero-Smith L (2010) Reciprocal regulation of EB1 and AR in triple negative breast cancer cells. Breast Cancer Res Treat 123(1):139–147
Varambally S, Dhanasekaran SM, Zhou M, Barrette TR, Kumar-Sinha C, Sanda MG, Ghosh D, Pienta KJ, Sewalt RGAB, Otte AP, Rubin MA, Chinnaiyan AM (2002) The polycomb group protein EZH2 is involved in progression of prostate cancer. Nature 419:624–629
Bachmann IM, Halvorsen OJ, Collett K, Stefansson IM, Straume O, Haukaas SA, Salvesen HB, Otte AP, Akslen LA (2006) EZH2 expression is associated with high proliferation rate and aggressive tumor subgroups in cutaneous melanoma and cancers of the endometrium, prostate, and breast. Oncol 24:268–273
Laitinen S, Martikainen PM, Tolonen T, Isola J, Tammela TLJ, Visakorpi T (2008) EZH2, Ki-67, and Mcm7 are prognostic markers in prostatectomy treated patients. Int J Cancer 122:595–602
Shen MM, Abate-Shen C (2010) Molecular genetics of prostate cancer: new prospects for old challenges. Genes Dev 24:1967–2000
Li J, Fan QH, Fan XS (2010) EZH2 expression in human prostate cacner and its clinicopathologic significance. Natl J Androl 16:123–128
Cao Q, Yu J, Dhanasekaran SM, Kim HJ, Mani RS, Tomlins SA, Mehra R, Laxman B, Cao X, Kleer CG (2008) Repression of E-cadherin by the polycomb group protein EZH2 in cancer. Oncogene 27:7274–7284
Chen H, Tu SW, Hsieh JT (2005) Down-regulation of human DAB2IP gene expression mediated by polycomb Ezh2 complex and histone deacetylase in prostate cancer. J Biol Chem 280:22437–22444
Hermans KG, van Marion R, van Dekken H, Jenster G, van Weerden WM, Trapman J (2006) TMPRSS2:ERG fusion by translocation or interstitial deletion is highly relevant in androgen-dependent prostate cancer, but is bypassed in late-stage andgrogen receptor-negative prostate cancer. Cancer Res 66:10658–10663
Nam RK, Sugar L, Wang Z, Kitching R, Klotz LH, Venkateswaran V, Narod SA, Seth A (2007) Expression of TMPRSS2:ERG gene fusions in prostate cancer cells is an important prognostic factor for cancer progression. Cancer Biol Ther 6:e1–e6
Narod SA, Seth A, Nam R (2008) Fusion in the ETS gene family and prostate cancer. Br J Cancer 99:847–851
Perner S, Demichelis F, Beroukhim R, Schmidt FH, Mosquera JM, Setlur S, Tchinda J, Tomlins SA, Hofer MD, Pienta KG, Kuefer R, Vessella R, Sun XY, Meyerson M, Lee C, Sellers WR, Chinnaiyan AM, Rubin MA (2006) TMPRSS2:ERG fusion associated deletions provide insight into the heterogeneity of prostate cancer. Cancer Res 66:8337–8341
Rajput AB, Miller MA, De Luca A, Boyd N, Leung S, Hurtado-Coll A, Fazli L, Jones EC, Palmer JB, Gleave ME, Cox ME, Huntsman DG (2007) Frequency of the TMPRSS2:ERG gene fusion is increased in moderate to poorly differentiated prostate cancers. J Clin Pathol 60:1238–1243
Soller MJ, Isaksson M, Elfving P, Soller W, Lundgren R, Panagopoulos I (2006) Confirmation of the high frequency of the TMPRSS2:ERG fusion gene in prostate cancer. Genes Chromosomes Cancer 45:717–719
Yu J, Yu J, Mani RS (2010) An integrated network of androgen receptor, polycomb, and TMPRSS2-ERG gene fusions in prostate cancer progression. Cancer Cell 17:443–454
Yu J, Cao Q, Yu J, Wu L, Dallol A, Li J, Chen G, Grasso C, Cao X, Lonigro RJ, Varambally S, Mehra R, Palanisamy N, Wu JY, Latif F, Chinnaiyan AM (2010) The neuronal repellant SLIT2 is a target for repression by EZH2 in prostate cancer. Oncogene 29(39):5370–5380
Yardy GW, Brewster SF (2005) Wnt signalling and prostate cancer. Prostate Cancer Prostatic Dis 8:119–126
Crawford HC, Fingleton BM, Rudolph-Owen LA, Goss KJ, Rubinfeld B, Polakis P, Matrisian LM (1999) The metalloproteinase matrilysin is a target of beta-catenin transactivation in intestinal tumors. Oncogene 18(18):2883–2891
He T-C, Sparks AB, Rago C, Hermeking H, Zawel L, da Costa LT, Morin PJ, Vogelstein B, Zinzler KW (1998) Identification of c-MYC as a target of the APC pathway. Science 281(5382):1509–1512
Marchenko ND, Marchenko GN, Weinreb RN, Lindsey JD, Kyshtoobayeva A, Crawford HC, Strongin AY (2004) Beta-catenin regulates the gene MMP-26, a novel matrix metalloproteinase expressed both in carcinomas and normal epithelial cells. Int J Biochem Cell Biol 36(5):942–956
Tetsu O, McCormick F (1999) Beta-catenin regulates expression of cyclin D1 in colon carcinoma cells. Nature 398:422–426
Robinson DR, Zylstra CR, Williams BO (2008) Wnt signaling and prostate cancer. Curr Drug Targets 9(7):571–780
Truica CI, Byers S, Gelmann EP (2000) Beta-catenin affects androgen receptor transcriptional activity and ligand specificity. Cancer Res 60:4709–4713
Gupta S, Iljin K, Sara H, Mpindi JP, Mirtti T, Vainio P, Rantala J, Alanen K, Nees M, Kallioniemi O (2010) FZD4 as a mediator of ERG oncogene-induced WNT singaling and epithelial- to- mesenchymal transition in human prostate cancer cells. Mol and Cell Pathobiol 70(17):6735–6745
Grunert S, Jechlinger M, Meug H (2003) Diverse cellular and molecular mechanisms contribute to epithelial plasticity and metastasis. Nat Rev Mol Cell Biol 4:657–665
Siegel PM, Massague J (2003) Cytostatic and apoptotic actions of TGF-Beta in homeostasis and cancer. Nat Rev Cancer 3:807–820
Zhu B, Kyprianou N (2005) Transforming growth factor beta and prostate cancer. Cancer Treat Res 126:157–173
Zhu M-L, Kyprianou N (2008) Androgen receptor and growth factor signaling cross talk in prostate cancer cells. Endocr Relat Cancer 15:841–849
Zhu M-L, Partin JV, Bruckheimer EM, Strup SE, Kyprianou N (2008) TGF-Beta signaling and androgen receptor status determine apoptotic cross-talk in human prostate cancer cells. Prostate 68(3):287–295
Derynck R, Zhang YE (2003) Smad-dependent and Smad-independent pathways in TGF-Beta family signaling. Nature 425:577–584
Coffey RJ Jr, Shipley GD, Moses HL (1986) Production of transforming growth factors by human colon cancer lines. Cancer Res 46:1164–1169
Pu H, Collazo J, Jones E, Gayheart D, Sakamoto S, Vogt A, Mitchell B, Kyprianou N (2009) Dysfunctional transforming growth factor beta receptor II accelerates prostate tumorigenesis in the TRAMP mouse model. Cancer Res 69(18):7366–7374
Ten Dijke P, Goumans MJ, Itoh F, Itoh S (2002) Regulation of cell proliferation by Smad proteins. J Cell Physiol 191:1–16
Akhurst RJ, Derynck R (2001) TGF-beta signaling in cancer- a double edged sword. Trends Cell Biol 11:S44–S51
Schmidt LJ, Duncan K, Yadav N, Regan KM, Verone AR, Lohse CM, Pop EA, Attwood K, Wilding G, Mohler JL, Sebo TJ, Tindall DJ, Heemers HV (2012) RhoA as a mediator of clinincally relevant androgen action in prostate cancer cells. Mol Endocrinol 26(5):716–735
Bierie B, Moses HL (2006) TGF-beta and cancer. Cytokine Growth Factor Rev 17(1–2):29–40
Ivanovic V, Melman A, Davis-Joseph B, Valcic M, Gelieber J (1995) Elevated plasma levels of TGF-beta in patients with invasive cancer. Nat Med 1(4):282–284
Levy L, Hill CS (2006) Alterations in components of the TGF-beta superfamily signaling pathways in human cancer. Cytokine Growth Factor Rev 17(1–2):41–58
Wojtowicz-Praga S (2003) Reversal of tumor-induced immunosuppression by TGF-beta inhibitors. Invest New Drugs 21(1):21–32
Song K, Wang H, Krebs TL, Wang B, Kelley TJ, Danielpour D (2010) DHT selectively reverses Smad3-mediated/TGF-Beta-induced responses through transcriptional down-regulation of Smad3 in prostate epithelial cells. Mol Endocrinol 24:2019–2029
van der Poel HG (2005) Androgen receptor and TGFbeta1/Smad signaling are mutually inhibitory in prostate cancer. Eur Urology 48(6):1051–1058
Hayes SA, Zarnegar M, Sharma M, Yang F, Peehl DM, Ven Dijke P, Sun Z (2001) SMAD3 represses androgen receptor-mediate transcription. Cancer Res 61:2112–2118
Kang HY, Huang KE, Chang SY, Ma WL, Lin WJ, Chang C (2002) Differential modulation of androgen receptor-mediated transactivation by Smad3 and tumor suppressor Smad4. J Biol Chem 277:43749–43756
Boccon-Gibod L, Hammerer P, Madersbacher S, Mottet N, Prayer-Galetti T, Tunn U (2007) The role of intermittent androgen deprivation in prostate cancer. BJU Int 100:738–743
Thuault S, Tan EJ, Peinado H, Cano A, Heldin CH, Moustakas A (2008) HMGA2 and Smads co-regulate SNAIL1 expression during induction of epithelial-to-mesenchymal transition. J Biol Chem 283:33437–33446
Mascareno EJ, Belashov I, Siddiqui MAQ, Liu F, Dhar-Mascareno M (2012) Hexim-1 modulates androgen receptor and the TGF-Beta signaling during the progression of prostate cancer. Prostate 72:1035–1044
Lee DK, Chang C (2003) Molecular communication between androgen receptor general transcription machinery. J Steroid Biochem Mol Biol 84(1):41–49
Alarcon C, Zaromytidou AI, Xi Q, Gao S, Yu J, Fujisawa S, Barlas A, Miller AN, Manova-Todorova K, Macias MJ, Sapkota G, Pan D, Massague J (2009) Nuclear CDKs drive Smad transcriptional activation and turnover in BMP and TGF-beta pathways. Cell 139(4):757–769
Matsuura I, Chiang KN, Lai CY, He D, Wang G, Ramkumar R, Uchida T, Ryo A, Lu K, Liu F (2010) Pin1 promotes transforming growth factor beta induced migration and invasion. J Biol Chem 285(3):1754–1764
Bolos V, Grego-Bessa J, de la Pompa JL (2007) Notch signaling in development and cancer. Endocr Rev 28(3):339–363
Rebay I, Fleming RJ, Fehon RG, Cherbas L, Cherbas P, Artavanis-Tsakonas S (1991) Specific EGF repeats of Notch mediate interactions with delta and serrate: implications for notch as a multifunctional receptor. Cell 67:687–699
Bettenhausen B, Hrabe de Angelis M, Simon D, Guenet JL, Gosler A (1995) Transient and restricted expression during mouse embryogenesis of DII1, a murine gene closely related to Drosophila Delta. Development 121:2407–2418
Dunwoodie SL, Henrique D, Harrison SM, Beddington RS (1997) Mouse D113: a novel divergent Delta gene which may complement the function of other Delta homologues during early pattern formation in the mouse embryo. Development 124:3065–3076
Lindsell CE, Shawber CJ, Boulter J, Weinmaster G (1995) Jagged: a mammalian ligand that activates Notch1. Cell 80:909–917
Shawber C, Boulter J, Lindsell CE, Weinmaster G (1996) Jagged2: a serrate-like gene expressed during rat embryogenesis. Dev Biol 180:370–376
Shutter JR, Scully S, Fan W, Richards WG, Kitajewski J, Deblandre GA, Kintner CR, Stark KL (2000) DII4, a novel Notch ligand expressed in arterial endothelium. Genes Dev 14:1313–1318
Timmerman LA, Grego-Bessa J, Raya A, Bertran E, Perez-Pomares JM, Diez J, Aranda S, Palomo S, McCormick F, Izpisua-Belmonte JC, de la Pompa JL (2004) Notch promotes epithelial-mesenchymal transition during cardiac development and oncogenic transformation. Genes Dev 18:99–115
Santagata S, Demichelis F, Riva A, Varambally S, Hofer MD, Kutok JL, Kim R, Tang J, Montie JE, Chinnaiyan AM, Rubin MA, Aster JC (2004) JAGGED1 expression is associated with prostate cancer metastasis and recurrence. Cancer Res 64:6854–6857
Bailey JM, Singh PK, Hollingsworth MA (2007) Cancer metastasis facilitated by developmental pathways: sonic hedgehog, notch, and bone morphogenic proteins. J Cell Biochem 102:829–839
Acknowledgments
Support: NIH/NIDDK R01 Grant 00491815; James F. Hardymon Research Endowment
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Martin, S.K., Fiandalo, M.V., Kyprianou, N. (2013). Androgen Receptor Signaling Interactions Control Epithelial–Mesenchymal Transition (EMT) in Prostate Cancer Progression. In: Wang, Z. (eds) Androgen-Responsive Genes in Prostate Cancer. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-6182-1_15
Download citation
DOI: https://doi.org/10.1007/978-1-4614-6182-1_15
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-6181-4
Online ISBN: 978-1-4614-6182-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)