
Abstract
OptiMedica was founded in Silicon Valley in 2004 to deliver innovative ophthalmic technologies and transform existing standards of care in retina, glaucoma and cataract. Our breakthrough technologies include the PASCAL® (Pattern SCAnning Laser) family of photocoagulators for the treatment of retinal disease and glaucoma and the Catalys™ Precision Laser System for the treatment of cataract [1–4].
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction By Mark Forchette: OptiMedica and Pattern Scanning Lasers
OptiMedica was founded in Silicon Valley in 2004 to deliver innovative ophthalmic technologies and transform existing standards of care in retina, glaucoma and cataract. Our breakthrough technologies include the PASCAL® (Pattern SCAnning Laser) family of photocoagulators for the treatment of retinal disease and glaucoma and the Catalys™ Precision Laser System for the treatment of cataract [1–4].
While we have been focused on both technologies from the very beginning, OptiMedica achieved its first commercial success with PASCAL. Launched worldwide in 2006, PASCAL was designed to dramatically improve the precision, efficiency and comfort of panretinal photocoagulation (PRP) procedures [1–4]. While a PRP treatment can require up to 2,000 laser spots, traditional single spot green laser photocoagulators required ophthalmologists to deliver them one at a time with a pulse duration of 100 ms. With the PASCAL pattern scanning technique, ophthalmologists could for the first time deliver up to 56 laser spots in half a second with a pulse duration of just 10 ms. This marked advancement brought significant benefits to ophthalmologists and patients, as treatments that previously required retrobulbar anesthetic blocks and multiple office visits could be completed in one visit with no block and with much less collateral tissue damage (see Fig. 17.1a–c).

(a) PASCAL photocoagulator. (b and c) Patterns from the PASCAL Streamline photocoagulator, the retinal photocoagulation product line developed by OptiMedica (image courtesy of OptiMedica Corporation, Sunnyvale, CA) https://optimedica.box.com/s/k7etsumdy08o2ms90do7
The benefits of our PASCAL technology led to rapid and broad adoption by ophthalmologists worldwide. By mid-2010, OptiMedica manufactured and shipped more than 600 PASCAL units in more than 40 markets around the world, with more than 750,000 patients treated and more than 30 million patterns delivered. This clinical and commercial success drew great interest from a number of other companies in the ophthalmic device industry, including Topcon Corp. Topcon added PASCAL to its product portfolio in 2008 and ultimately chose to acquire the technology in August 2010. The transaction, which represented the largest acquisition in the history of Topcon Corp.’s medical device business, delivered to Topcon Corp. a significant therapeutic product portfolio and a pipeline of retina innovation. At the same time, it was a strategic move for OptiMedica that gave us significant funding and the ability to apply undiluted focus to the development of our Catalys Precision Laser System.
Cataract procedures are in the midst of a revolutionary change, and we strongly believe that OptiMedica is poised to provide leadership in the technology that satisfies the high expectations of surgeons and their patients. As evidenced by our success with PASCAL, OptiMedica has a deep knowledge of laser–tissue interaction and the delivery of laser with high-speed scanning. Our research, development, and manufacturing teams excel in high quality optical design, integration of complex control systems, system ergonomics, and intuitive graphic user interface (GUI) design. We have a deep history of partnerships and personal relationships within the ophthalmic community, and our reputation for excellent customer service and support is second to none.
The Catalys™ Precision Laser System received CE Mark approval in Europe and FDA clearance in 2011 and 2012 for anterior capsulotomy, lens fragmentation, arcuate incisions and multiplanar primary and sideport cataract incisions. There are over 25 laser systems in operation in the USA and around the world at the time of this writing.
Motivating Concept: The Potential Impact of ReLACS on the Worldwide Market and Surgical Outcomes
From its founding in 2004, OptiMedica has been committed to delivering on the tremendous potential of ReLACS to ophthalmic surgeons and their patients. Together with Stanford University Chairman of Ophthalmology, Mark S. Blumenkranz, M.D., and Stanford research scientist, Daniel Palanker, Ph.D., the OptiMedica team began developing an OCT-guided FS laser with the idea that it could enhance cataract surgery by creating new levels of precision. Soon after the company’s inception, the initial patent for FS laser cataract surgery was filed.
In 2005, at the beginning of the ReLACS, development process, William Culbertson, I began working with OptiMedica after having spent 3 years using the Intralase FS laser in making flaps for LASIK at the Bascom Palmer Eye Institute. The fundamental precision of the Intralase instrument was immediately apparent, and we found that we could program the instrument to create LASIK flaps with diameters, shapes, thicknesses, and positions within 20 μm of what we intended to achieve. For the first time, we were able to customize the flap dimensions to the patient’s eye and to the intended type of correction. These results were far superior to what we could achieve using a microkeratome. Although the microkeratome usually made smooth interfaces, the inconsistencies of diameter, thickness, shape, and position made us largely abandon it for flap making.
I also found that the Intralase FS laser was a useful tool in performing other types of corneal surgery with dependability and accuracy that far exceeded what could be achieved with traditional manual techniques. Along with others, I created channels for INTACS rings, performed anterior lamellar keratoplasty with a perfect fit between donor and host [5], corneal incisions using preprogrammed dimensions and shapes, including arcuate incisions for correction of astigmatism [6], special shaped cataract incisions that seal better than manually created ones [7]. The software was even expanded to allow for custom shaped penetrating keratoplasty and deep anterior lamellar keratoplasty (“zig-zag,” “mushroom,” and “tophat” shapes).
In developing the Catalys Precision Laser System, our goal was to deliver the precision and safety benefits of FS laser technology to the practice of cataract surgery. Once we were able to demonstrate the feasibility of this concept in our initial bench laboratory work, we performed safety studies, and energy and scanning parameters were developed. A prototype FS laser with integral OCT imaging specifically designed for cataract surgery was constructed, initially employing a fixed curved single lens contact interface.
Following investigational review board (IRB) approval, human studies began in the Dominican Republic at the Clinica Centro Laser of Juan Batlle, M.D., in Santo Domingo in June 2009. Results from the very first cases confirmed our initial assumptions regarding the safety and accuracy of the laser, and we proceeded to develop a refined commercial instrument, which OptiMedica named “Catalys.”
The global market opportunity for FS lasers that perform cataract surgery is substantial. As the world’s population ages, surgical volumes are growing and cataract surgery patients are increasingly demanding the best visual outcomes made possible by new IOL technologies. Leading refractive cataract surgeons have recognized this trend and are dedicated to delivering the refractive outcomes that these patients expect. By creating consistent, reproducible cuts and pretreating the cornea and lens, Catalys has the potential to help cataract surgeons achieve the patient’s refractive goals.
Technical Aspects of the Commercial System
Laser System and Delivery
The Catalys FS laser engine is a diode-pumped solid state laser with a pulse duration <600 fs and near infrared wavelength of approximately 1,032 nm. A large focal depth of greater than 8 mm is required to fragment and soften cataractous tissue deep in the crystalline lens. The laser-focusing system needed to support this larger range of focal depth has special requirements, namely, a reduced numerical aperture and increased focal beam diameter. Therefore, as laser physics dictate, a higher threshold energy is needed for photodisruption of ocular tissues than with corneal FS laser surgery.
OptiMedica conducted preclinical and clinical studies to determine the operating parameter ranges for both safety and efficacy. The primary safety concerns of pulsed lasers at high repetition rates are heating of the retina (as described by the American National Standards Institute ocular laser safety standards) and of thermo-mechanical damage to retinal pigment epithelial cells. As a result of the safety studies, the repetition rate of the laser engine was modulated in application to maintain an average power based on pulse energy. To determine operating parameter ranges for efficacy, both preclinical and clinical studies were completed. With freshly enucleated porcine eyes and then 100 samples of enucleated human eyes, the team determined the threshold energy and pattern spot density (in both the lateral and axial dimensions) needed to make a continuous cut in the capsule and to segment the lens. Pulse energy ranged from 3 to 10 μJ with repetition rates between 12 and 80 kHz. Scanning parameters for pattern spot density were 5 μm in the lateral plane of the capsulotomy circle, 10 μm in its cylindrical depth and twice those values for lens fragmentation [8]. Operating parameters were further validated in the IRB-approved prospective clinical study in the Dominican Republic.
Docking System and Coupling to the Eye
The Catalys system includes an advanced Liquid Optics™ Interface, a disposable multi-piece patient–laser interface that serves as the final critical optic for the video and OCT imaging and laser delivery. Liquid Optics was the product of considerable innovative thinking and development. While the initial clinical study with Catalys used a curved applanating patient interface (PI), the surgical team and engineers saw an opportunity to improve the design to eliminate corneal folds, improve incision quality, reduce intraocular pressure (IOP) rise during docking, and reduce the unsightly subconjunctival hemorrhages that persisted for 2–3 weeks post-surgery. The team knew that surgeons and patients would be expecting a comfortable experience for the patient and a predictable refractive outcome that the initial curved lens PI configuration would not deliver to a satisfactory degree. Rather than speeding to market with a suboptimal design, the team committed to an alternative design that addressed all opportunities for improvement. The reengineered interface resulted in a novel, fluid-filled interface which does not distort the cornea and provides a clear optical path for precise OCT, video imaging and laser delivery. Moreover, when compared to the earlier interface, the Liquid Optics Interface has delivered a five-time reduction in IOP rise and has resulted in significantly less eye redness post-surgery [9] (see Fig. 17.2). Please see Chap. 6 for more information on details concerning the fluid-filled PI.

Liquid Optics Interface. Liquid Optics Interface docking system demonstrating the progression of placing the suction ring on the eye and raising the suction ring to engage with the disposable lens (image courtesy of OptiMedica Corporation, Sunnyvale, CA)
Imaging System
The Catalys system uses a proprietary long-range spectral domain OCT to accurately locate the ocular surfaces in three dimensions. The OCT is integrated with the FS laser optics and applied through the same focusing objective and Liquid Optics Interface as the FS laser. The axial resolution, which is based on the coherence length of the light source, is <15 μm. The lateral resolution, which is based on the optical design, is <40 μm. The image is acquired after the globe is secured to and stabilized by the PI. The accompanying live video system operates at a wavelength nearly coincident with the FS laser, with a field of view that is 17 mm in diameter. Signal processing algorithms use the raw OCT and video data to automatically identify the surfaces of the anterior cornea, posterior cornea, iris, anterior capsule, and posterior capsule.
While anterior segment OCT is broadly used in clinical practices today, as a diagnostic tool, not all OCT systems are designed with equal quality and technical specifications. For ReLACS, signal processing of 3D OCT images is needed to turn the diagnostic data into a controlled guidance system. OptiMedica’s Catalys addresses this requirement with Integral Guidance™, a proprietary image-guidance system that identifies ocular surfaces, creates and maintains exclusion (i.e., safety) zones where the laser cannot fire, helps the surgeon accurately and repeatedly adjust patterns, and ensures that the FS laser pulses are delivered precisely to the intended location.
Integral Guidance removes inverted OCT images (such as seeing a double iris) and other imaging artifacts, so the posterior capsule can be accurately identified. Ocular structures and laser exclusion zones can be created even when the eye is tilted relative to the laser path from docking, or in the case of a tilted crystalline lens with zonular dehiscence. Additionally, ocular surfaces such as the anterior and posterior capsule are identified, so the fragmentation depth can be maximized to safely deliver laser energy deep into the lens in order to make lens disassembly as easy as possible (see Fig. 17.3).

Catalys OCT. A cross-sectional view of the three-dimensional high-resolution spectral domain optical coherence tomography (OCT) from the Catalys graphical user interface (image courtesy of OptiMedica Corporation, Sunnyvale, CA)
Early Technical Obstacles and How They Were Overcome
OptiMedica believes the success of ReLACS will be measured on the scale of tens of microns. The company designed and developed the Catalys system to leave nothing to chance and to deliver the most precise results possible. Of the four systems currently in development and equipped to perform ReLACS, Catalys has demonstrated the highest levels of precision for the capsulotomy (according to published data available at the time of printing).
Getting to this level of precision did not happen overnight, and it did not happen alone. The multiple years-long development process for Catalys was highly collaborative, bringing together OptiMedica’s executive, engineering and development teams and a group of esteemed cataract surgeons from around the world. These surgeons participated closely at every point in the development process, weighing in on everything from clinical considerations and technical requirements to practice integration issues. They also treated hundreds of preclinical eyes, and many participated in IRB-approved clinical studies. In addition, OptiMedica worked closely with a Medical Staff Advisory Board comprised of technicians, nurses and practice administrators, each of whom lent unique perspective to the technology’s integration into clinical practice. Together, this extended team was able to develop unique and innovative solutions to address various obstacles during the Catalys system’s development.
For example, the Liquid Optics Interface was just one of many subsystems the OptiMedica team refined over time in order to get maximal precision, patient comfort and streamlined workflow. The template-based planning software and automatic surface detection are features that streamline workflow. Planning occurs prior to patient docking and can be completed by someone other than the treating physician. The automatic and highly accurate surface detection algorithms, which are the cornerstone of the Catalys system’s Integral Guidance™ process, eliminate the need for the surgeon to manually identify ocular surfaces while the patient is under dock. While it took OptiMedica several years to refine planning and surface detection, the resulting subsystems enhance the accuracy of the procedure and minimize the amount of time that a patient is under dock. This last point is especially critical, as elderly patients may have ocular comorbidities like glaucoma and vascular diseases, so time under dock and intraocular pressure rise should be minimized. Currently we have reduced docked time to approximately 3 min with the expectation that this will decrease with engineering refinements. Since the IOP is only nominally increased during dockage with the Liquid Optics Interface (see Chap. 6), it is unlikely that this period of suction attachment will have any clinical significance.
The supreme measure of the quality of a system is the performance it delivers. Throughout the development process, OptiMedica and its team of advisors prioritized precision, accuracy, safety, and ergonomics as the most important elements to deliver patient benefit with the Catalys system.
Clinical Capabilities and Parameters for Cataract Surgery
The Catalys Precision Laser System is designed to perform the anterior capsulotomy, laser phacofragmentation, corneal arcuate incisions and transcorneal cataract incisions with paracenteses. The capsulotomy is performed first, followed by lens fragmentation and corneal incisions. For each cut, the laser pulses are applied posterior to anterior in order to avoid cavitation and gas bubbles that may be created by treatment posterior to the laser.
Laser Anterior Capsulotomy
Laser Ablation Pattern and Energies/Spacing
OptiMedica conducted extensive preclinical trials with freshly enucleated porcine eyes to determine the laser parameters that enable precise and complete capsulotomies with minimal collateral damage. The experimental design involved extracting the lens, placing it in balanced salt solution (BSS), and vertically directing the laser energy to the anterior capsule through a cover slip. The pattern spot density needed to create a continuous cut with a pulse duration of <600 fs and wavelength of 1,032 nm, was a focal spot size <10 μm, lateral spot spacing of 5 μm and axial spacing of 10 μm [8]. The threshold pulse energy to induce cavitation was approximately 3 μJ. Similar operating parameters were used in clinical trials; the exact values were proprietary at the time of this textbook’s publishing.
Vertical Extent of Laser Treatment
Using Integral Guidance, Catalys registers the 3D curvature of the anterior capsule and automatically adjusts the incisional depth so that the depth is consistent along the entire circumference of the capsulotomy. If the lens is tilted relative to the laser pathway, Catalys tilts the laser treatment plane to correspond to the lens tilt. This results in a consistent cut that is simultaneously applied over the 360° of the capsulotomy. For this reason, the system is able to optimize the capsulotomy parameters to ensure a complete cut while minimizing energy applied to the eye.
Strength of Cuts
Capsulotomy strength was tested by distending empty porcine capsules and registering the force at rupture. The break force for 3 μJ laser capsulotomy was 152 ± 21 mN compared with 65 ± 21 mN for manual CCC (p < 0.05) [10].
Accuracy of Cuts
In a randomized, prospective IRB-approved study, 29 eyes received the Catalys laser procedure and 30 eyes received manual cataract surgery. For all eyes, the anterior capsular disks were removed prior to phacoemulsification so that shape and circularity of the CCC or capsulotomy could be measured.
Size: Size accuracy was calculated as the deviation between intended diameter and observed diameter. The mean deviation for manual capsulorhexis was −0.282 ± 0.305 mm, whereas the mean deviation for laser capsulotomy was just 0.027 ± 0.025 mm (p < 0.001). This represented a more than tenfold decrease in deviation from intended diameter. Moreover, the size variability from case to case was much reduced (see Fig. 17.2), demonstrating a much more predictable and repeatable capsulotomy construction with the laser (see Fig. 17.4).

Capsule size and shape. Laser capsulotomy from the Catalys Precision Laser System stained with trypan blue demonstrating an order of magnitude more precision in size and shape (image courtesy of OptiMedica Corporation, Sunnyvale, CA) https://optimedica.box.com/s/ikmbky7b8p2xvry9gwek
Shape: Circularity was measured as a function of disk size and area. A perfect circle has a circularity value of 1.00. The manual capsulorhexis had a mean circularity of 0.77 ± 0.15 (n = 22), while the laser capsulotomy had a mean circularity of 0.95 ± 0.04 (n = 29) (p < 0.001) [8, 10] (see Fig. 17.4).
Centration: Following laser delivery, centration of the laser capsulotomy was analyzed using still frames from the Catalys video system. Centration accuracy was measured relative to the intended capsulotomy center. The average root mean squared distance from the center of capsulotomy to the intended center was just 0.077 ± 0.047 mm [10]. The manual capsulorhexis was centered by the surgeon’s view and could not be measured with micron level accuracy for comparison purposes (see Fig. 17.5a, b).

Centration image. (a) Laser capsulotomy centration. Still frame from Catalys video system during capsulotomy centration. (b) Overlay of X/Y scatter plot with average root mean square distance of capsulotomy center and dilated pupil center (image courtesy of OptiMedica Corporation, Sunnyvale, CA)
Postoperative Consistency of Effect
The size and shape of capsule aperture changes over time [11, 12]. Size and shape changes in OptiMedica laser capsulotomy eyes and manual CCC eyes were analyzed at time of surgery and 1 week and 4 weeks postoperatively. The diameter of the laser apertures deviated just 0.1 mm, on average, whereas the manual CCC apertures decreased in size by over half a millimeter. The laser aperture shape was also more consistent over time [10].
Unique Benefits
The accuracy and precision of capsulotomy size, shape, and centration achieved with Catalys is unmatched by any system, according to published data available at the time of print. Moreover, the surgeon can select the method for centering the capsulotomy preoperatively, such as on the center of the dilated pupil or scanned capsule center as determined by OCT. After the patient is docked to the system, Integral Guidance can automatically adjust the planned capsulotomy according to the chosen target for the patient.
Limitations Overcome
In ReLACS, the cornea is part of the optical system. To enable precise imaging and laser delivery it is critical that both the anterior and posterior surfaces of the cornea are undistorted. In OptiMedica’s first approach, the curved lens interface applanated the cornea and induced folds in nearly 75% of cases. These folds reduced the ability of the laser to focus to a point below a fold. The clinical impact was striking, as skips or tags in the capsulotomy were visualized directly posterior to corneal folds [9].
Lens Fragmentation
Geometric Patterns
OptiMedica studied a wide range of patterns in years of preclinical studies and only went to clinical trials with those patterns expected to be successful. The commercial system is equipped with a variety of nuclear fragmentation patterns for segmenting and softening the crystalline lens. Segmentation patterns include a cross design, a sextant pattern and an octant pattern. Softening patterns deliver laser energy to the regions in between the incision lines created by the segmentation patterns (see Fig. 17.6).

Lens fragmentation pattern exploration. Lens fragmentation patterns, including both segmentation and softening, from the Catalys Precision Laser System (image courtesy of OptiMedica Corporation, Sunnyvale, CA)
Fragmentation Dimensions
In a Catalys procedure, the fragmentation dimensions (width and depth) are matched precisely to the 3D ocular anatomy of each patient. Once the patient is under dock, Integral Guidance detects the iris boundaries and posterior capsule and sets exclusion zones to delineate areas where the laser cannot fire. The volume of the lens fragmentation zone is safely maximized in two ways:
-
1.
The fragmentation width is bounded by an iris margin instead of the capsulotomy diameter Catalys is able to fragment more peripherally while still safely avoiding the iris.
-
2.
The fragmentation depth follows the curvature of the posterior capsule instead of being guided by one (or several) manually selected marker(s). This approach allows the lens to be fragmented at a consistent, safe and minimal distance from the posterior capsule. In the IRB-approved study (n = 30 laser; n = 29 manual), the fragmentation depth varied from 2.7 to 4.9 mm, as dictated by the thickness of the crystalline lens [13] (see Fig. 17.7a, b).
Fig. 17.7 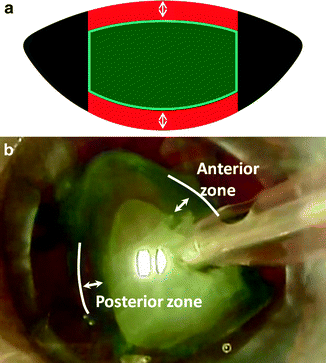
Laser exclusion zones. (a) Schematic of anterior and posterior lens safety margins (highlighted with white arrows) and lens fragmentation zone ( in the middle) created with Integral Guidance. Safety margins are defined regions where the laser cannot fire. (b) Video frame of phaco tip grabbing a lens quadrant following laser lens fragmentation. Anterior and posterior lens safety zones created with Integral Guidance are maintained through laser lens fragmentation and visible during lens removal (image courtesy of OptiMedica Corporation, Sunnyvale, CA)

Effectiveness of Laser Lens Pre-softening
Study Design
Cataracts were graded preoperatively on the LOCSIII scale for density. Most of the patients had advanced cataracts, with almost three-quarters of enrolled patients registering a LOCS grade 3 or 4 cataract. For each patient, one eye was randomized to manual cataract surgery while the other eye received the Catalys laser procedure followed by ultrasound phaco-assisted lens extraction and IOL implantation. After each phacoemulsification procedure, the cumulative dissipated energy (CDE) registered on the Alcon Infiniti system was recorded.
Study Result
Overall, there was approximately a 40% reduction in CDE for the laser pretreated lenses as compared to the non-pretreated lenses (p = 0.028) [13]. According to anecdotal evidence, laser pretreatment of the lens makes a grade 4 lens feel like a grade 2 during ultrasound phacoemulsification. The CDE data supports this claim, with grade 4 pretreated lenses registering a CDE of 19.5 and grade 2 non-pretreated lenses registering a CDE of 18.2 (see Fig. 17.8). With refinements in patterns and phaco equipment, Professor HB Dick, Chairman of the University Eye Hospital, Bochum Germany, has found a 96% reduction across all grades.

CDE chart by LOCS grade. Comparison of cumulative dissipated energy (CDE) used per case with and without lens segmentation and softening performed with Catalys. Results are grouped by preoperative nuclear color and opalescence based on the Lens Opacities Classification System III (image courtesy of OptiMedica Corporation, Sunnyvale, CA)
In a follow-up study, surgical video was reviewed and the number of active phaco manipulations (movement of phaco tip in conjunction with use of phaco power) was recorded. The laser pretreated lenses required 45% fewer active surgical phaco manipulations to segment into four quadrants than did non-pretreated lenses [14].
Limitations Overcome
Results of OptiMedica’s clinical studies demonstrated a progressive decline in phaco energy usage as the surgeons became accustomed to working with laser-segmented and softened lenses.
Unique Benefits
Catalys lens fragmentation is optimized for accuracy, effectiveness, safety and speed. The accuracy is enabled by the system’s clear imaging pathway and precise surface detection algorithms. Fragmentation is highly effective, with a near [96] CDE reduction across all cataract grades. Automated exclusion zone registration makes lens treatment safe by ensuring that lasers are delivered a consistent distance from posterior capsule and iris. Lastly, speed is optimized because surface detection does not require manual delineation of ocular surfaces by the surgeon.
Corneal Incisions
Clear Corneal Incisions
The architecture and dimensions of Catalys corneal incisions are customizable for self-sealing architectures. Given the wide inner diameter of the suction ring (14.5 mm), these incisions can be created with high precision at the limbal edge, if desired, without decentering the suction ring. The incision can be configured as fully penetrating or not, as dictated by sterility requirements. Since the system in OptiMedica’s Dominican Republic study was located outside of the operating room, the corneal incisions were non-penetrating (see Fig. 17.9a–d).

Catalys corneal incisions. (a and b) Architecture of clear cornea incision initiated with Catalys Precision Laser System. The laser incision (yellow) and diamond knife incision (red) are highlighted on the post-op OCT image. Laser incision was not fully penetrating so as to maintain sterility of the procedure (image courtesy of OptiMedica Corporation, Sunnyvale, CA). (c and d) Still frame from video from Catalys Precision Laser video system during creation of arcuate incision (image courtesy of OptiMedica Corporation, Sunnyvale, CA) https://optimedica.box.com/s/nd4bc98nwfpzl6hh1au3
Corneal Arcuate Incisions
Compared to manual incisions, the laser has the ability to create more consistent, predictable incisions in arc length, depth, angulation, and shape. While the patient is under dock, Integral Guidance registers the corneal thickness at the location of planned arcuate incision. The depth of the incision can be programmed during treatment planning as a set micron value (e.g., 600 μm) or as a percentage of corneal thickness at the treatment location.
Improved consistency in the incision should lead to a more consistent outcome. Given the difference in tissue reaction to laser photocavitation as compared to a blade, large-scale studies will need to be conducted to determine an appropriate nomogram for laser corneal arcuate incisions.
Ergonomic Simplicity of Operation
Catalys was designed with superior ergonomics to ensure surgeon ease-of-use and a comfortable patient experience.
Graphical User Interface
The Catalys system’s intuitive and elegant touchscreen graphical user interface was designed to simplify the planning process and minimize the time that the patient is under dock. The system is equipped with a high definition 24-in. monitor that can be positioned for comfortable use and visibility from a standing or seated position (see Fig. 17.10).

Catalys graphical user interface. Sample Catalys Precision Laser System treatment page as seen on graphical user interface (image courtesy of OptiMedica Corporation, Sunnyvale, CA)
Mobility of Device
Precision in ReLACS involves more than just controlling the directionality of a laser. It is also critical to control the target. When designing Catalys, safety and precision were OptiMedica’s top design objectives. Since success in the procedure is measured in tens of microns, OptiMedica equipped Catalys with an integrated Dexta bed with custom headrest that was explicitly designed to maximize the head stability of elderly cataract patients.
Footprint
Catalys is designed for comfortable use in a 10 × 10 square foot area; this area includes the system footprint, an integrated patient chair, surgeon chair and service access. For installation, Catalys can fit through a 34-in. doorway.
Procedural Workflow
Treatment planning: Planning a treatment on the Catalys system is quick, intuitive and template-based. Templates for each incision can be configured for commonly used treatment parameters. The surgeon or a member of the technical staff can enter the treatment plan for a particular patient in advance of the procedure. The process takes less than one minute.
Patient docking: The Liquid Optics suction ring is placed on the sclera and the connection is stabilized by system-controlled vacuum. The surgeon then fills the ring with balanced saline solution (BSS) and swings the patient bed under the system. Using the joystick on the patient chair, the surgeon maneuvers the chair to mate the suction ring to the disposable lens attached to the system. This connection is stabilized by another vacuum and a mechanical lock.
Treatment customization: Once the patient is under dock, Integral Guidance quickly and accurately customizes the treatment plan to fit the ocular anatomy of the patient. The surgeon simply needs to confirm the customized plan (adjusted if necessary) and then initiate treatment. The system workflow was designed to minimize patient time under dock. Minimizing dock time is relevant to procedure precision because patient stability is critical to accurate laser delivery. In addition, minimizing the amount and duration of IOP rise is a safety standard for elderly patients.
Treatment delivery: The capsulotomy takes 2 s; and the full set of laser incisions takes approximately 40–60 s to complete, depending on the cuts included and the parameters.
Ten Compelling Reasons Why a Customer Should Buy the Catalys Precision Laser System
-
1.
Catalys delivers unsurpassed clinical outcomes, stemming from its superior technology.
-
2.
Catalys offers surgeons the unique benefits of an advanced, proprietary Liquid Optics Interface™. Designed to be a crucial element in the optical path, the Liquid Optics Interface eliminates corneal folds and results in lower IOP rise and less petechiae after the procedure.
-
3.
Catalys delivers unparalleled precision and safety with Integral Guidance™, which combines proprietary 3D Spectral Domain OCT and signal processing to automatically detect and map the ocular surfaces and automatically create exclusion zones. Integral Guidance customizes the surgeon’s treatment plan to the anatomy and the orientation of the patient’s eye relative to the laser.
-
4.
Catalys features an easy-to-use and elegant graphical user interface designed to simplify the planning process and minimize the time that the patient is under dock.
-
5.
As evidenced by the features and benefits above, Catalys is the product of a development process based on the deep involvement of physicians and staff, resulting in a detailed understanding of the requirements and workflow.
-
6.
OptiMedica is dedicated to developing superior technology and demonstrating clinical results through rigorous scientific studies.
-
7.
OptiMedica has a history of technology innovation in ophthalmology, including the development of the family of PASCAL photocoagulators. Through that effort, the company developed and brought to market revolutionary technology and sold more than 600 systems worldwide before the business was acquired by Topcon Corp.
-
8.
OptiMedica has an unwavering dedication to supporting ophthalmologists and their staffs in the application of the technology and to creating true partnerships to ensure the successful integration of ReLACS into the practice.
-
9.
OptiMedica has strong financial backing from top investors, including Kleiner Perkins, Caufield & Byers, Alloy Ventures, DAG Ventures, BlackRock, and Bio*One Capital.
-
10.
OptiMedica’s management team is a group of industry veterans that brings collective knowledge from ophthalmology and from the broader medical device community. The company’s executives have held leadership positions at Alcon, AMO, Intralase, Wavelight, Coherent, Intuitive Surgical, Boston Scientific, Medtronic, and Guidant.
Future Developments and Upgradability
OptiMedica has a strong and highly innovative research and development organization that is working on a range of enhancements to the Catalys Precision Laser System as well as next generation products.
References
Bol’shunov AV. The first experience in clinically using a PASCAL laser photocoagulator (OptiMedica, USA). Vestn Oftalmol. 2009;125(4):37–8.
Sanghvi C, McLauchlan R, Delgado C, et al. Initial experience with the Pascal photocoagulator: a pilot study of 75 procedures. Br J Ophthalmol. 2008;92(8):1061–4 [Epub 2008 Jun 27].
Modi D, Chiranand P, Akduman L. Efficacy of patterned scan laser in treatment of macular edema and retinal neovascularization. Clin Ophthalmol. 2009;3:465–70 [Epub 2009 Aug 20].
Bolz M, Kriechbaum K, Simader C, Diabetic Retinopathy Research Group Vienna, et al. In vivo retinal morphology after grid laser treatment in diabetic macular edema. Ophthalmology. 2010;3:538–44 [Epub 2010 Jan 4].
Yoo SH, Kymionis GD, Koreishi A, Ide T, Goldman D, Karp CL, O’Brien TP, Culbertson WW, Alfonso EC. Femtosecond laser-assisted sutureless anterior lamellar keratoplasty. Ophthalmology. 2008;115:1303–7.
Kymionis GD, Yoo SH, Ide T, Culbertson WW. Femtosecond-assisted astigmatic keratotomy for post-keratoplasty irregular astigmatism. J Cataract Refract Surg. 2009;35:11–3.
Culbertson WW. Presented at the Intralase Users Meeting AAO 11/2006 AAO was in Las Vegas, USA.
Palanker DV, Blumenkranz MS, Andersen D, Wiltberger M, Marcellino G, et al. Femtosecond laser-assisted cataract surgery with integrated optical coherence tomography. Sci Transl Med. 2010;2:58ra85.
Talamo JH. Optical interface characteristics for laser cataract surgery. In: Proceedings of the American Society of Cataract and Refractive Surgery (ASCRS) 2011 annual meeting, femtosecond laser cataract surgery, session 1-E, 26 March 2011, San Diego, CA. p. 134.
Friedman NJ, Palanker DV, Schuele G, et al. Femtosecond laser capsulotomy. J Cataract Refract Surg. 2011;37:1189–98.
Park TK, Chung SK, Baek NH. Changes in the area of the anterior capsule opening after intraocular lens implantation. J Cataract Refract Surg. 2002;28:1613–7.
Hayashi K, Hayashi H. Intraocular lens factors that may affect anterior capsule contraction. Ophthalmology. 2005;112:286–92.
Culbertson WW, Batlle JF, Feliz R, Koch D, et al. Facilitation of nuclear cataract removal by femtosecond laser pretreatment. In: Proceedings of the American Society of Cataract and Refractive Surgery (ASCRS) 2011 annual meeting, femtosecond laser cataract surgery, session 1-E, 26 March 2011, San Diego, CA. p. 134.
Koch DD, Culbertson WW, Batlle JF. The use of OCT guided femtosecond laser to facilitate cataract uclear disassembly and aspiration. In: Proceedings of the European Society of Cataract and Refractive Surgery (ESCRS) 2010 annual meeting, Free paper session, Paris, France.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Culbertson, W.W. (2013). Commercially Available Systems: OptiMedica’s Catalys Precision Laser System. In: Krueger, R., Talamo, J., Lindstrom, R. (eds) Textbook of Refractive Laser Assisted Cataract Surgery (ReLACS). Springer, New York, NY. https://doi.org/10.1007/978-1-4614-1010-2_17
Download citation
DOI: https://doi.org/10.1007/978-1-4614-1010-2_17
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-1009-6
Online ISBN: 978-1-4614-1010-2
eBook Packages: MedicineMedicine (R0)