
Abstract
In 1993 Genant et al. [1], during their osteoporosis related research, described a semi quantitative method based on the height of T4-L4 vertebras as shown on lateral views. Vertebral fractures are the most common osteoporotic fractures and it was therefore assumed that they can be used as outcome variables in osteoporosis preventing and treatment studies. Vertebrae T4-L4 were graded on visual inspection and without direct vertebral measurement as:
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Description
In 1993 Genant et al. [1], during their osteoporosis related research, described a semi quantitative method based on the height of T4-L4 vertebras as shown on lateral views. Vertebral fractures are the most common osteoporotic fractures and it was therefore assumed that they can be used as outcome variables in osteoporosis preventing and treatment studies. Vertebrae T4-L4 were graded on visual inspection and without direct vertebral measurement as:
-
Normal (grade 0)
-
Mildly deformed (grade 1, approximately 20–25 % reduction in anterior, middle, and/or posterior height)
-
Moderately deformed (grade 2, approximately 25–40 % reduction in any height)
-
Severely deformed (grade 3, approximately 40 % reduction in any height)
-
Additionally, a grade 0.5 was given to designate borderline deformed vertebras (Fig. 56.1).
Fig. 56.1 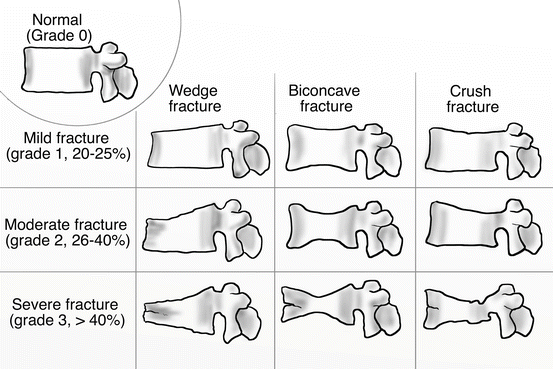
The nine types of osteoporotic vertebral fractures according to the shape of the vertebral body (wedge, biconcave, crush) and the height of the vertebral body from the T4-L4 (grade 0 normal height; grade 1 20–25 % reduction of height; grade 2 25–40 % reduction of height; grade 3 >40 % reduction of height)

Fractures were also classified as:
-
1.
Wedge.
-
2.
Biconcave
-
3.
Crush
whether the anterior, middle or posterior column was relevantly involved.
A vertebral body was considered to be fractured if graded I or higher and it was considered normal if graded 0 or 0.5. In addition, a spinal fracture index (SFI) was calculated for each patient by summing the individual vertebral deformity scores and dividing by the number of vertebrae evaluated.
Treatment Strategy [2–6]
Osteoporotic vertebral compression fractures may remain asymptomatic or minimally symptomatic. Nonetheless, a large number of patients will experience significant pain, affecting their quality of life and causing disability. Non-operative medical treatment for these patients includes pain medication, activity limitation, physical therapy, and (possibly) bracing. In general terms patients with osteoporotic vertebral compression fractures are usually treated non-operatively.
The main operative techniques to surgically treat osteoporotic vertebral compression fractures are kyphoplasty and vertebroplasty. Surgical treatment shall be decided on the basis of pain and percentage of vertebral collapse. If a patient rates his/her pain as being greater than 4 out of 10 (if 10 equals the worst pain imaginable and 0 equals no pain) or the vertebral bodies are collapsed more than 40 %, then kyphoplasty or vertebroplasty is indicated as an initial intervention. Practically this means that grade I and II fractures shall be initially treated non-operatively whereas grade III fractures initial treatment shall be surgical.
Other indications for vertebroplasty or kyphoplasty may be pain-requiring medication persisting for longer than 1 month or advancement of kyphosis despite adequate non-operative care. In cases of neurologic impairment or radiographic evidence of instability more invasive procedures (e.g. decompression and fusion) shall be considered.
In any case patients with osteoporotic vertebral fractures shall be consulted to start anti-osteoporotic medication even if their BMD index is within normal or osteopenic range.
Osteoporotic vertebral fractures – evidence according to Genant classification | |||
|---|---|---|---|
Classification | Cochrane library | ||
Grade 1 | Percutaneous balloon kyphoplasty or vertebroplasty for symptomatic vertebral fractures | Cement augmentation provides greater pain relief than non-operative treatment | Lack of evidence |
Grade 2 | Percutaneous balloon kyphoplasty or vertebroplasty for symptomatic vertebral fractures | Cement augmentation provides greater pain relief than non-operative treatment | Lack of evidence |
Grade 3 | Percutaneous balloon kyphoplasty or vertebroplasty for symptomatic vertebral fractures | Cement augmentation provides greater pain relief than non-operative treatment | Lack of evidence |
References
Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 1993;8(9):1137–48.
Chiras J, Depriester C, Weill A, Sola-Martinez MT, Deramond H. Percutaneous vertebral surgery. Technics and indications. J Neuroradiol. 1997;24(1):45–59.
Freedman BA, Potter BK, Nesti LJ, Giuliani JR, Hampton C, Kuklo TR. Osteoporosis and vertebral compression fractures-continued missed opportunities. Spine J. 2008;8(5):756–62.
Karlsson MK, Hasserius R, Gerdhem P, Obrant KJ, Ohlin A. Vertebroplasty and kyphoplasty: new treatment strategies for fractures in the osteoporotic spine. Acta Orthop. 2005;76(5):620–7.
Prather H, Watson JO, Gilula LA. Nonoperative management of osteoporotic vertebral compression fractures. Injury. 2007;38 Suppl 3:S40–8.
Skedros JG, Holyoak JD, Pitts TC. Knowledge and opinions of orthopaedic surgeons concerning medical evaluation and treatment of patients with osteoporotic fracture. J Bone Joint Surg Am. 2006;88(1):18–24.
Anderson PA, Froyshteter AB, Tontz Jr WL. Meta-analysis of vertebral augmentation compared with conservative treatment for osteoporotic spinal fractures. J Bone Miner Res. 2013;28(2):372–82.
Shi MM, Cai XZ, Lin T, Wang W, Yan SG. Is there really no benefit of vertebroplasty for osteoporotic vertebral fractures? A meta-analysis. Clin Orthop Relat Res. 2012;470(10):2785–99.
Taylor RS, Fritzell P, Taylor RJ. Balloon kyphoplasty in the management of vertebral compression fractures: an updated systematic review and meta-analysis. Eur Spine J. 2007;16(8):1085–100.
McGirt MJ, Parker SL, Wolinsky JP, Witham TF, Bydon A, Gokaslan ZL. Vertebroplasty and kyphoplasty for the treatment of vertebral compression fractures: an evidenced-based review of the literature. Spine J. 2009;9(6):501–8.
Papanastassiou ID, Phillips FM, Van Meirhaeghe J, Berenson JR, Andersson GB, Chung G, Small BJ, Aghayev K, Vrionis FD. Comparing effects of kyphoplasty, vertebroplasty, and non-surgical management in a systematic review of randomized and non-randomized controlled studies. Eur Spine J. 2012;21(9):1826–43.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag London
About this chapter
Cite this chapter
Lasanianos, N.G., Triantafyllopoulos, G.K., Pneumaticos, S.G. (2015). Osteoporotic Vertebral Fractures. In: Lasanianos, N., Kanakaris, N., Giannoudis, P. (eds) Trauma and Orthopaedic Classifications. Springer, London. https://doi.org/10.1007/978-1-4471-6572-9_56
Download citation
DOI: https://doi.org/10.1007/978-1-4471-6572-9_56
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-6571-2
Online ISBN: 978-1-4471-6572-9
eBook Packages: MedicineMedicine (R0)