
Abstract
Atherosclerotic cardiovascular disease is a leading cause of mortality worldwide. Structural and functional evidence of early vascular disease is present in children and adolescents and can be assessed noninvasively. This chapter details the noninvasive techniques commonly used to assess arterial structure and function and their research and clinical application in children and adolescents. The use of these techniques in describing the “at-risk” individual and the potential for assessing early prevention strategies are also discussed.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Adventitia
- Arterial stiffness
- Arteriosclerosis
- Artery
- Atherosclerosis
- Cardiovascular disease
- Cerebrovascular disease
- CT
- Endothelium
- Flow-mediated dilatation
- MRI
- Noninvasive detection
- Plethysmography
- Risk factors
- Ultrasound
Introduction
Cardiovascular and cerebrovascular diseases are common and related diseases that affect the heart and blood vessels. They have differing presentations – including ischemic stroke, angina, and myocardial infarction – but a common pathogenesis. Together they are the leading cause of morbidity and mortality in both developed and developing nations.
Cardiovascular events occur almost uniquely in adults, with approximately 95 % of first myocardial infarctions occurring in those over 40 years of age [1]. Cardiovascular events often occur suddenly, without prior symptoms or clinical signs. This frequent lack of identifiable prior symptoms belies the chronic nature of the diseases of the blood vessels that account for the majority of these events. These vascular diseases can be categorized loosely as atherosclerosis and arteriosclerosis, the former being characterized by low level inflammation and lipid deposition in the arterial wall and the latter being defined as a hardening of the arteries. Indeed, the structural and functional antecedents of atherosclerosis and arteriosclerosis may begin in the first decade of life [2–4]. Logically, early detection is valuable to identify high-risk subjects and to maximize chances of disease reversibility by early prevention strategies.
Atherosclerosis
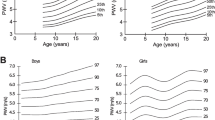
Atherosclerosis is an inflammatory disease of the blood vessels, involving the formation of plaque-like lesions through a process of adaptive thickening of the intima, foam cell formation with subsequent appearance of lipid pools, and fibrous thickening of the arterial wall over the lesion. Of importance to the noninvasive detection of atherosclerosis, the disease process results in arterial wall thickening, calcium deposition in or near arterial atheromatous lesions, and dysregulation of the functional properties of the vasculature. These occur at varying stages of disease progression; however, the earliest structural changes to the arterial wall seem to be ubiquitous and can appear in the first decade of life [3, 4]. The earliest structural evidences consistent with the atherosclerotic disease process are lipid deposits in the aortic wall, present in all individuals, but the extent and severity of which are influenced by putative risk factors, especially hyperlipidemia [3]. By late childhood, the influence of risk factors on disease progression becomes more pronounced, especially in “at-risk” parts of the vasculature, resulting in widespread fatty streaks and the development of aortic fibrofatty lesions in some individuals (Fig. 31.1) [4]. More advanced atheromatous and complex lesions follow, often in early adult life, but these are rare in children and adolescents. Despite structural evidence of the atherosclerotic disease process being present in some form in all individuals, the extent and severity of the disease differs greatly among adults.

Prevalence of fatty streaks and raised lesions in the abdominal aorta stratified by age and sex [4]. Proximal portion at left; distal, right; dorsal, lower edge. Bottom, color intensity scales for prevalence of fatty streaks and raised lesions (Reprinted from McGill et al. [4]., Lippincott Williams & Wilkins)
There is now a large body of literature, however, indicating that the functional properties of the arterial wall are important contributors to the initiation, progression, and clinical risk of atherosclerosis. The endothelial layer is the most well-characterized functionally active layer of the arterial vasculature. The healthy endothelium generally has an atheroprotective influence on the vasculature; however, in the presence of risk factors or other pro-atherosclerotic stimuli, it can promote or favor the initiation and progression of atherosclerosis [5].
Functional properties of the arterial adventitia and periadventitial tissues may also contribute to the progression of atherosclerosis. While less well understood, there is evidence that the adventitia and periadventitia may be involved in cross talk with the other arterial layers, including via the release vasoactive substances [6], and as such may be important mediators of vascular health and disease.
Risk Factors for Cardiovascular Disease: Relevance in Childhood
There are a number of risk factors that are considered to be established independent risk factors for cardiovascular disease, including hypertension, hypercholesterolemia, diabetes, smoking (active or passive), male gender, aging, and a family history of premature cardiovascular disease. Many of these can be relevant in children and adolescents. While these are considered risk factors for cardiovascular disease as a whole, the strength of risk associated with each factor differs for each specific type of cardiovascular disease and hence may also differ for each specific measure of arterial health. These associations may also be population dependent.
More recently, obesity has emerged as a risk factor of considerable interest, although whether it is an independent risk factor remains contentious, as much of the risk of atherosclerotic cardiovascular disease associated with obesity is mediated at least in part by other established coexisting risk factors, such as hypertension and diabetes. There is a variety of other emerging risk factors, including sleep apnea, periodontal disease, and sedentary lifestyle.
Noninvasive measures of arterial health reflect only specific aspects of cardiovascular risk and do not fully capture an individual’s risk of cardiovascular events. As with specific risk factors, the association of different measures of arterial health with different cardiovascular disease endpoints differs [7]. Accordingly, while noninvasive measures of arterial health provide some indication of the impact of risk factors and disease prevention strategies, they are inherently a surrogate measure for cardiovascular events. Nonetheless, they provide an excellent means by which to assess vascular health in asymptomatic individuals, including children, and provide insight into potential risk factors and prevention strategies.
Early abnormalities can be structural (e.g., arterial wall thickening) or functional (e.g., impaired vascular reactivity). These aspects are reviewed in the next section.
Noninvasive Assessment of Arterial Structure
Carotid Intima–Media Thickness (IMT)
Carotid IMT is the most widely used noninvasive test for the assessment of preclinical atherosclerosis in adults. The test uses high-resolution external ultrasound to obtain a longitudinal scan of the carotid artery, near the bifurcation into the internal and external carotid arteries. There are a number of different scanning and measurement protocols for the assessment of carotid IMT, specifically differing by site (common carotid, carotid “bulb,” internal carotid, or a combination) and the type of measurement (mean, maximum, or the average of the maximum thickness from multiple sites).
There are numerous factors that enable the assessment IMT of the carotid artery and the relevance thereof. It is a large conduit artery that is sufficiently superficial to allow for detailed imaging using high-resolution ultrasound. The carotid IMT is measured near a major bifurcation, which allows for more marked intimal–medial thickening than that from a straight non-branching arterial segment.
In adults, increased carotid IMT is associated with multiple cardiovascular risk factors, including male gender, systolic blood pressure, type 2 diabetes, LDL cholesterol, cigarette smoking, obesity, and the metabolic syndrome [8–11]. Risk factors present during childhood and adolescence are also associated with increased carotid IMT and progression of carotid IMT in later adulthood [12, 13], independent of risk factors assessed during adulthood. Beyond being reflective of risk factor levels alone, carotid IMT is predictive of future cardiovascular events, even after taking into account the effect of established cardiovascular risk factors [7, 14]. These associations with incident cardiovascular events are similar, irrespective of measurement site or type of measurement [7], although a recent study indicates that in adults this association may be more pronounced for the single thickest measure derived from the internal carotid artery [14], a site prone to plaque development, rather than measuring the mean carotid IMT over a long segment of the common carotid.
Carotid IMT is readily obtained in older children and adolescents. In these groups carotid IMT is associated with cardiovascular risk factors, including obesity, familial hypercholesterolemia, low HDL cholesterol, type 1 diabetes, and increased blood pressure [15–19], and can be influenced by intervention strategies, most notably with weight loss and exercise [20]. Carotid IMT tracks well through adult life [21], but it is unknown whether or not it tracks well specifically from childhood to adolescence to adulthood.
Aortic IMT
While the carotid artery is the most common site for IMT assessment in adults and children alike, the earliest structural changes consistent with the atherosclerotic process and the first arterial lesions appear in the abdominal aorta [4]. Assessment of aortic wall structure is possible in adults using MRI; however, due to the depth of penetration required to scan the abdominal aorta in adults, the use of high-frequency, high-resolution ultrasound is potentially limited. In contrast, in infants and children it is possible to assess the IMT of the abdominal aorta [18, 22]. As with carotid IMT, aortic IMT is derived from a longitudinal ultrasound scan, typically obtained using a high-resolution linear array transducer (7–15 MHz). The abdominal aorta is routinely scanned in a non-branching segment, frequently localized near a specific landmark, such as the aortic bifurcation [18].
Aortic IMT may be a more sensitive marker of subclinical atherosclerosis during childhood than is carotid IMT, with respect to ascertaining the effects of risk factors on arterial structure [18]. For example, aortic IMT is significantly increased in newborns with impaired fetal growth (Fig. 31.2) [22], an emerging cardiovascular risk factor [23]. This observation provides potential mechanistic insight into the link between fetal growth and adult cardiovascular disease and suggests that measures of arterial structure may be a useful means by which to assess the putative benefits of early life interventions aimed at improving vascular health, in those with intrauterine or other early life risk factors [23].

Adventitial Thickness
Beyond IMT, recently developed noninvasive techniques allow for the assessment of arterial adventitial structure. A major constraint in the assessment of carotid adventitial structure is the poor differentiation by ultrasound of the outer interface of the adventitia. Emerging techniques directly, or indirectly, overcome this constraint through a variety of means.
Contrast-enhanced imaging allows for a quantitative measure of the carotid artery vasa vasorum, an important and major component of the adventitia, as opposed to the adventitia per se. The widespread application of this technique in children is restricted, however, by the requirement for contrast-enhanced imaging.
Very high-resolution ultrasound, using a much higher frequency transducer (25–55 MHz) than that used for traditional vascular scans, clearly delineates the outer edge of the adventitia [24]. The trade-off between frequency and depth of penetration means that this technique is only applicable in the most superficial, muscular arteries, such as the brachial and radial, and not the carotid artery or other central arteries, even in a pediatric population [24].
Carotid extra-medial thickness uses high-resolution longitudinal ultrasound of the carotid–jugular complex approximately 1.5–2 cm proximal to the bifurcation, where the jugular and carotid rest side by side [25], and avoids the need to delineate the outer edge of the artery by including the carotid wall from the media–adventitia interface through the jugular lumen–intima interface in the measure. For this technique the trade-off is the incorporation into the measure of the entire venous wall and any interstitial tissue that lies between the two vessels. Importantly though, these non-arterial components do not appear to be altered by cardiovascular risk factors [25], and while obviously being important contributors to the absolute thickness, they appear to be only minor contributors to variance in thickness [26]. As the carotid extra-medial thickness technique has only recently been described, there is currently limited evidence concerning associations with risk factors. A cross-sectional study indicated that carotid extra-medial thickness may be more closely related to modifiable risk factors than is carotid IMT and that these associations are independent of carotid IMT [25]. There are currently no published reports of the use of this technique in children. The similarity between this technique and carotid IMT in terms of acquisition methodology indicates that the measurement of carotid extra-medial thickness is most likely feasible in children, and indeed it has recently been successfully assessed in children aged 8 years of age (Skilton and Celermajer, unpublished results).
These techniques do not allow for the differentiation between different tissue types and cell populations within the adventitia, such as resident fibrocyte populations or progenitor cells, with the exception of imaging of the vasa vasorum.
Carotid and Aortic Wall Thickness by Magnetic Resonance Imaging (MRI)
Carotid and aortic wall thickness can be assessed noninvasively by MRI without the use of contrast agents. The artery is routinely imaged in cross section with MRI, in keeping with the slice direction of the acquisition sequence, which is in contrast to the ultrasound-based techniques described above. This allows for a circumferential measure of thickness, which may capture greater heterogeneity of arterial wall structure including areas that are prone to lesion development [27]. The arterial wall when imaged with MRI appears as a single layer, so differentiation between the intima, media, and adventitia is not possible. Whether arterial wall thickness derived by MRI includes all three layers or only the intima and media is open to conjecture [26–28]. This may be dependent upon the spatial resolution, which is greater for larger 3T MRI, when compared with 1.5T MRI. The spatial resolution limitations of 1.5T MRI are also likely to limit the accuracy of MRI in children, as a means by which to serially monitor arterial wall thickness or to determine the associations of wall thickness with risk factors. Despite this limitation, MRI may provide a useful means by which to diagnose and monitor diseases that involve aortic wall thickening and vascular inflammation, such as Takayasu’s arteritis [29].
Coronary Artery Calcium by Computed Tomography (CT)
As noted earlier, calcium deposits form in advanced atherosclerotic lesions. These are detectable in the coronary arteries by CT. In adults, the extent of coronary artery calcium is associated with cardiovascular risk factors [30] and is inversely associated with coronary vasoreactivity; independent of such risk factors [31], coronary calcium also appears to be predictive of future cardiovascular events [32].
There are two underlying limitations for the use of CT for detecting coronary artery calcium in children and adolescents. The first is that CT scanning involves some radiation exposure, so coronary artery calcium CT is not recommended for clinical use or clinical research in children. Accordingly, there have only been a few studies detailing the use of CT for coronary artery calcium in children and adolescents, and in general the application of the technique is restricted to high-risk groups in which the perceived benefit outweighs the known risks [33].
Published reports indicate that in asymptomatic adolescents and young adults, aged 14–29 years, the prevalence with any measurable coronary artery calcium is 11 % for males and 6 % for females, although the latter was derived from a single individual with detectable coronary calcium (from 17 individuals assessed) [34]. While asymptomatic, the majority of patients described in this chapter were referred because of known cardiovascular risk factors or self-referred, so the population prevalence of detectable coronary calcium in this age group is likely to be lower. At the other end of the risk spectrum are those with familial hypercholesterolemia, a major risk factor for premature cardiovascular events. In patients with familial hypercholesterolemia, one third of individuals aged 11–23 years have no detectable evidence of coronary calcium [35]. “High” coronary calcium scores were found in 24 % of these patients, suggesting that CT for coronary artery calcium may potentially allow further risk discrimination for adolescents and young adults with a high-risk profile. These studies underline the second limitation of CT for detection of coronary artery calcium in children and adolescents, that it measures a level of disease that is generally more advanced than that seen in children and adolescents.
Arterial Function: Endothelial and Smooth Muscle
Conduit Artery Flow-Mediated Dilatation (FMD)
As noted earlier, the arterial endothelium is an active cell layer that forms the interface with the blood. Of importance, a healthy functional arterial endothelium has a host of antiatherogenic properties, many mediated by the release of nitric oxide. Nitric oxide plays a key role in maintaining vascular homeostasis, in addition to other anti-atherosclerotic properties such as reducing coagulation and leukocyte adhesion to the endothelium [5]. Nitric oxide is difficult to assess in the circulation; however, its dilatory effects on the arterial vasculature in response to various stimuli can be assessed in the coronary arteries by invasive techniques and in the peripheral vasculature by noninvasive techniques.
The gold-standard research methodology for the noninvasive determination of conduit artery endothelial function is arterial FMD assessed by high-resolution ultrasound. The technique evaluates arterial endothelial function as the ability of the artery to dilate in response to a hyperemic stimulus, most commonly initiated by a period of arterial occlusion. Protocols differ on whether this occlusion is upstream or downstream from the site of assessment, and this choice may alter the proportion of the subsequent dilatation resulting from endothelial release of nitric oxide [36] and therefore endothelial function. Nonetheless, the technique itself has changed little since its initial description [2]. In adults, the brachial or radial arteries are most frequently imaged; however, in children the femoral is also utilized (see subsequent discussion below for further details). Importantly, the FMD of peripheral conduit vessels correlates with coronary endothelial function [37].
A high-resolution, longitudinal B-mode ultrasound of the artery is acquired while the participant lies at rest. An occlusion cuff situated either proximal or distal to the site of assessment (see below for further details) is then inflated to suprasystolic pressure, typically 50 mm Hg above systolic blood pressure. After approximately 5-min occlusion, the cuff is rapidly deflated. The artery dilates in response to the ensuing hyperemia, typically reaching peak dilatation at around 45–60 s post cuff release in healthy young subjects; however, this may be markedly delayed in subjects with poor vascular health [38]. Protocols differ, however, and the FMD is most commonly taken as the percentage dilatation from the resting diameter at either a particular point in time (e.g., 45–60 s) or the peak dilatation within 3 min of cuff deflation, the latter of which appears to better discriminate between healthy and at-risk individuals [39]. Furthermore, the peak dilatation has been demonstrated to be largely due to endothelial release of nitric oxide [40]. After the arterial diameter has returned to baseline levels (approximately 10 min), endothelium-independent dilatation is assessed to ensure the smooth muscle dilatory capacity. This is typically tested using sublingual glyceryl trinitrate.
In addition to the timing of FMD measurement post-occlusion, there are a number of critical elements in the protocol that can introduce variance to the FMD measure if not standardized, including the duration of occlusion and the site of the occlusion cuff. These seemingly slight variations may have important implications [36], including altering the proportion of the dilatation due to endothelial nitric oxide release; however, they do not appear to alter the association of FMD with cardiovascular events [41].
This technique was originally described in a pediatric population and is thus readily applicable in children. There are, however, some minor changes to the protocol that are often introduced for use in children. These include the assessment of a larger conduit artery, such as the femoral, instead of the brachial artery as interrogated in adults. This is primarily a means by which to limit the excessively high FMD observed in arteries with small diameters [2] but also for ease of data acquisition. Another common alteration to the protocol is the removal of the endothelium-independent dilatation component of the protocol, involving administration of the smooth muscle vasodilator glyceryl trinitrate.
Arterial FMD has been demonstrated to be inversely associated with individual cardiovascular risk factors, including systolic blood pressure, male sex, smoking, age, and body mass index [42, 43], and independently with the total burden of cardiovascular risk, as determined by the number of risk factors [44]. The use of arterial FMD as a surrogate has also aided in the description of emerging risk factors, such as fetal growth, allowing for greater refinement of the “at-risk” individual, in addition to more complete mechanistic insight [45, 46].
Beyond associations with risk factors, arterial FMD is associated with carotid IMT in cross-sectional examinations [47], and also with progression of carotid IMT [48], and is predictive of cardiovascular events [41]; however, this has not been the case in all studies. The majority of studies showing this association with incident cardiovascular events suggest that the association is independent of established risk factors and is similar in those with preexisting cardiovascular disease and asymptomatic individuals [41].
In childhood, FMD is associated with risk factors, and putative risk factors, including hyperlipidemia (especially familial hypercholesterolemia; Fig. 31.3), low HDL cholesterol, type 1 diabetes, obesity, passive smoking, and impaired fetal growth [2, 15, 19, 45, 49, 50].

Children with familial hypercholesterolemia (FH) have impaired endothelium-dependent dilatation, as assessed by flow-mediated dilatation (FMD) [50]. Horizontal lines, group means; open circles, subjects with heterozygous FH; solid circles, subjects with homozygous FH (Reprinted from Sorensen et al. [50], with permission from The American Society for Clinical Investigation, Inc.)
FMD is a dynamic measure of arterial endothelial function and is thus well suited as a means to determine the efficacy on arterial health of putative prevention strategies and treatments. A limitation, however, is that it may be transiently impaired, for example, during a flu-like illness [51]. Reversibility studies with arterial FMD have included demonstrations of improvement in endothelial function with oral L-arginine supplementation in young adults with familial hypercholesterolemia (Fig. 31.4) [52], weight loss and exercise in obese children (Fig. 31.5) [20], and “cessation” of passive smoking [53].

Reversal of endothelial impairment with oral L-arginine in hypercholesterolemic young adults – a randomized placebo-controlled crossover trial of 4-week L-arginine supplementation on flow-mediated dilatation [52]. Results of P < 0.001 for comparison of L-arginine with placebo. Bold lines represent group means and standard deviation (Reprinted from Clarkson et al. [52], with permission from The American Society for Clinical Investigation, Inc.)

Reversal of endothelial impairment with weight loss and exercise in overweight children – a randomized trial of dietary modification and supervised exercise versus dietary modification alone [20]. Top panel shows improvement in flow-mediated dilatation in both groups; however, this improvement was greater in the diet and exercise group (P = 0.01). Group data are means and standard deviation. Bottom panel shows the continued improvement in flow-mediated dilatation in those who maintained exercise training through 1 year, whereas the endothelial function in those who “detrained” and reverting to dietary modification alone returned toward baseline levels (P = 0.035 for comparison at 1 year). Box, line, and error bars represent 2.5th, 25th, 50th (median), 75th, and 97.5th percentiles (Reprinted from Woo et al. [20], Lippincott Williams & Wilkins)
Small-Vessel Function
There are a number of techniques that allow for the study of small-vessel function. The gold-standard measure of resistance vessel endothelial function is the forearm blood flow response to acetylcholine infusions, assessed by venous-occlusion strain-gauge plethysmography. This technique is not routinely used in pediatric research due to the need for an arterial line; however, like arterial FMD, plethysmography can also be used to quantify the vascular response to a hyperemia.
Two distinct plethysmographs are commonly used – strain-gauge plethysmography and fingertip plethysmography. With the former, the measuring device – a mercury in Silastic strain gauge – is placed around the forearm at the point of greatest circumference and is able to assess the pulsatile changes in forearm circumference. Periodic upper arm venous occlusion allows for the quantification of forearm blood flow, either at rest or during post-occlusion hyperemia.
The fingertip method has recently become popular, with devices such as the EndoPAT (Itamar Medical Ltd, Israel), an FDA-approved device for the noninvasive assessment of endothelial function, streamlining and simplifying the assessment of arterial function and providing good reproducibility, including in adolescents [54].
With these two techniques, the site of measurement is distal to the occlusion site, as it is with the upper arm cuff position used in some FMD protocols. Accordingly, the proportion of the measure due to endothelial-derived nitric oxide may be lower, with ischemic metabolites potentially having a larger influence. This may be more pronounced for strain-gauge plethysmography around the forearm, as this measures a larger, more muscular body of tissue, as opposed to the fingertip-derived EndoPAT. Indeed, nitric oxide is only a minor contributor to the hyperemic response of the forearm [55], whereas the EndoPAT-assessed response has been reported to be ∼50 % due to endothelial nitric oxide release [56]. Both methods correlate with more established measures of endothelial function; forearm plethysmography with acetylcholine-induced dilatation of the same vascular bed [57], and EndoPAT with both brachial FMD from the same hyperemic stimulus [58], and coronary microcirculatory function [59]. Similarly, there is evidence that both techniques may predict cardiovascular events independent of established risk factors [60, 61].
Both techniques are applicable in adolescents, with the response to hyperemia measured by EndoPAT being impaired in adolescents with type 1 diabetes [62] and the forearm hyperemic response being impaired in African American adolescents [63].
Arterial Stiffness
Pulse Wave Velocity (PWV)
PWV can be noninvasively assessed through the comparison of the timing of pulse waves at two peripheral arterial sites. The most common techniques involve the use of (a) two tonometers recording simultaneously or (b) a single tonometer used to assess two sites sequentially, with concurrent ECG reading. With both techniques, the distance between the sites is required to calculate the velocity. There are three different measurement methods – total distance between sites, subtracting the carotid to sternal notch distance from the total distance, or subtracting the carotid to sternal notch distance from the sternal notch to femoral distance. These differing methods introduce variance to the absolute PWV values reported in the literature. This stresses the importance of consistency of methods for cross-sectional studies or when undertaking serial measures [64].
With the “two tonometer” technique, the PWV (in m/s) is calculated as the distance between the two sites divided by the difference in time between the arrival of the pulse wave (as indicated by the upstroke of the pulse waveform) at the two sites of assessment.
With the “single tonometer” technique, each pulse wave is assessed independently, and the transit time from the heart to the site is derived from a comparison with the ECG.
In adults, the two sites most frequently assessed are the carotid artery and the femoral artery, and the carotid–femoral PWV is considered the gold-standard noninvasive test of arterial stiffness [64]. Importantly, using these two sites provides a measure of PWV principally due to aortic arterial stiffness.
Subject acceptability potentially limits the use of the femoral artery site as a component of a noninvasive research methodology in otherwise healthy children. One alternative is to use other more readily accessible distal sites, such as carotid–radial PWV, carotid–dorsalis pedis PWV, or brachial–ankle PWV. There is limited evidence available to support the use of one site over the other; however, carotid–dorsalis pedis PWV and brachial–ankle PWV will at least partially reflect central (aortic) stiffness. Furthermore, there are distinct structural differences between muscular arteries, such as the brachial and radial arteries, and the central arteries, which are predominantly elastic in nature, and as such the PWV along these distinct segments may differ.
In adults, aortic PWV is an independent predictor of cardiovascular events in both asymptomatic and “at-risk” populations [65, 66]. For children, the available evidence indicates that age, sex, type 1 diabetes, blood pressure, and obesity may be important childhood risk factors for increased PWV [67–69].
Cross-Sectional Distensibility
Site-specific measures of arterial stiffness can be assessed in the aorta, carotid, or brachial artery using ultrasound or MRI. The ultrasound techniques can be added to an IMT or FMD protocol using standard equipment or undertaken using dedicated echo-tracking equipment. Ideally, a simultaneous pressure measurement is required to allow calculation of stiffness indices, such as distensibility and compliance, likely more meaningful for cardiovascular risk than measuring the change in diameter alone. Regional measures of carotid stiffness may not be as relevant as aortic stiffness derived by PWV, with regard to their prediction of incident cardiovascular events [70], possibly related to inherent differences in the determinants of carotid and aortic stiffness [71]. In children and adolescents, carotid stiffness is associated with LDL-cholesterol levels, obesity, and insulin resistance [72, 73]. Aortic stiffness can be assessed in newborns by ultrasound and is increased in those born with impaired fetal growth [74].
Conclusion
Atherosclerosis begins in childhood and is detectable using noninvasive techniques to assess structural and functional changes in the arterial vasculature (Table 31.1). At this early stage, such changes are potentially reversible. Accordingly, noninvasive detection of atherosclerosis provides important insights into the pathogenesis and prevention of atherosclerosis. These techniques are not currently recommended for clinical use, however, and there remain important gaps in the current knowledge, especially concerning the relevance of these measures in children, as surrogates for cardiovascular risk.
Specifically, do measures of arterial structure and function assessed in childhood and adolescence predict future cardiovascular events?
The long time period that separates childhood from the typical age of onset of cardiovascular events will make this difficult to determine, but the latter may be inferred through a combination of tracking from childhood to early adulthood and studies that will soon report on whether or not measures of arterial structure and function assessed in early adulthood predict early cardiovascular events. While an important issue, the lack of this evidence need not distract from the consistency of association of these measures with the extent and severity of atherosclerosis in childhood and adolescence and their relevance in describing risk factors for, and designing preventive strategies to slow the progression of, early atherosclerosis. Further research will show whether early identification and reversibility studies can influence the natural history of cardiovascular events secondary to atherosclerosis.
References
Yusuf S, Hawken S, Ounpuu S et al (2004) Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case–control study. Lancet 364:937–952
Celermajer DS, Sorensen KE, Gooch VM et al (1992) Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 340:1111–1115
Napoli C, Glass CK, Witztum JL et al (1999) Influence of maternal hypercholesterolaemia during pregnancy on progression of early atherosclerotic lesions in childhood: fate of Early Lesions in Children (FELIC) study. Lancet 354:1234–1241
McGill HC Jr, McMahan CA, Herderick EE et al (2000) Effects of coronary heart disease risk factors on atherosclerosis of selected regions of the aorta and right coronary artery. PDAY Research Group. Pathobiological determinants of atherosclerosis in youth. Arterioscler Thromb Vasc Biol 20:836–845
Celermajer DS (1997) Endothelial dysfunction: does it matter? Is it reversible? J Am Coll Cardiol 30:325–333
Lohn M, Dubrovska G, Lauterbach B et al (2002) Periadventitial fat releases a vascular relaxing factor. FASEB J 16:1057–1063
Lorenz MW, Markus HS, Bots ML et al (2007) Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis. Circulation 115:459–467
Skilton MR, Sieveking DP, Harmer JA et al (2008) The effects of obesity and non-pharmacological weight loss on vascular and ventricular function and structure. Diabetes Obes Metab 10:874–884
Skilton MR, Moulin P, Serusclat A et al (2007) A comparison of the NCEP-ATPIII, IDF and AHA/NHLBI metabolic syndrome definitions with relation to early carotid atherosclerosis in subjects with hypercholesterolemia or at risk of CVD: evidence for sex-specific differences. Atherosclerosis 190:416–422
Ebrahim S, Papacosta O, Whincup P et al (1999) Carotid plaque, intima media thickness, cardiovascular risk factors, and prevalent cardiovascular disease in men and women: the British Regional Heart Study. Stroke 30:841–850
Salonen JT, Seppanen K, Rauramaa R et al (1989) Risk factors for carotid atherosclerosis: the Kuopio Ischaemic Heart Disease Risk Factor Study. Ann Med 21:227–229
Raitakari OT, Juonala M, Kahonen M et al (2003) Cardiovascular risk factors in childhood and carotid artery intima-media thickness in adulthood: the Cardiovascular Risk in Young Finns Study. JAMA 290:2277–2283
Juonala M, Viikari JS, Kahonen M et al (2010) Life-time risk factors and progression of carotid atherosclerosis in young adults: the Cardiovascular Risk in Young Finns study. Eur Heart J 31:1745–1751
Polak JF, Pencina MJ, Pencina KM et al (2011) Carotid-wall intima-media thickness and cardiovascular events. N Engl J Med 365:213–221
Skilton MR, Celermajer DS (2006) Endothelial dysfunction and arterial abnormalities in childhood obesity. Int J Obes (Lond) 30:1041–1049
Ayer JG, Harmer JA, Nakhla S et al (2009) HDL-cholesterol, blood pressure, and asymmetric dimethylarginine are significantly associated with arterial wall thickness in children. Arterioscler Thromb Vasc Biol 29:943–949
Wiegman A, de Groot E, Hutten BA et al (2004) Arterial intima-media thickness in children heterozygous for familial hypercholesterolaemia. Lancet 363:369–370
Jarvisalo MJ, Jartti L, Nanto-Salonen K et al (2001) Increased aortic intima-media thickness: a marker of preclinical atherosclerosis in high-risk children. Circulation 104:2943–2947
Jarvisalo MJ, Raitakari M, Toikka JO et al (2004) Endothelial dysfunction and increased arterial intima-media thickness in children with type 1 diabetes. Circulation 109:1750–1755
Woo KS, Chook P, Yu CW et al (2004) Effects of diet and exercise on obesity-related vascular dysfunction in children. Circulation 109:1981–1986
Raiko JR, Magnussen CG, Kahonen M et al (2010) Tracking of noninvasive ultrasound measurements of subclinical atherosclerosis in adulthood: findings from the Cardiovascular Risk in Young Finns Study. Ultrasound Med Biol 36:1237–1244
Skilton MR, Evans N, Griffiths KA et al (2005) Aortic wall thickness in newborns with intrauterine growth restriction. Lancet 365:1484–1486
Skilton MR (2008) Intrauterine risk factors for precocious atherosclerosis. Pediatrics 121:570–574
Sarkola T, Abadilla AA, Chahal N et al (2011) Feasibility of very-high resolution ultrasound to assess elastic and muscular arterial wall morphology in adolescents attending an outpatient clinic for obesity and lipid abnormalities. Atherosclerosis 219:610–615
Skilton MR, Serusclat A, Sethu AH et al (2009) Noninvasive measurement of carotid extra-media thickness: associations with cardiovascular risk factors and intima-media thickness. JACC Cardiovasc Imaging 2:176–182
Skilton MR, Boussel L, Bonnet F et al (2011) Carotid intima-media and adventitial thickening: comparison of new and established ultrasound and magnetic resonance imaging techniques. Atherosclerosis 215:405–410
Boussel L, Serusclat A, Skilton MR et al (2007) The reliability of high resolution MRI in the measurement of early stage carotid wall thickening. J Cardiovasc Magn Reson 9:771–776
Duivenvoorden R, de Groot E, Elsen BM et al (2009) In vivo quantification of carotid artery wall dimensions: 3.0-Tesla MRI versus B-mode ultrasound imaging. Circ Cardiovasc Imaging 2:235–242
Aluquin VP, Albano SA, Chan F et al (2002) Magnetic resonance imaging in the diagnosis and follow up of Takayasu’s arteritis in children. Ann Rheum Dis 61:526–529
Mahoney LT, Burns TL, Stanford W et al (1996) Coronary risk factors measured in childhood and young adult life are associated with coronary artery calcification in young adults: the Muscatine Study. J Am Coll Cardiol 27:277–284
Wang L, Jerosch-Herold M, Jacobs DR Jr et al (2006) Coronary artery calcification and myocardial perfusion in asymptomatic adults: the MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol 48:1018–1026
Arad Y, Goodman KJ, Roth M et al (2005) Coronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am Coll Cardiol 46:158–165
Brody AS, Frush DP, Huda W et al (2007) Radiation risk to children from computed tomography. Pediatrics 120:677–682
Janowitz WR, Agatston AS, Kaplan G et al (1993) Differences in prevalence and extent of coronary artery calcium detected by ultrafast computed tomography in asymptomatic men and women. Am J Cardiol 72:247–254
Gidding SS, Bookstein LC, Chomka EV (1998) Usefulness of electron beam tomography in adolescents and young adults with heterozygous familial hypercholesterolemia. Circulation 98:2580–2583
Pyke KE, Tschakovsky ME (2005) The relationship between shear stress and flow-mediated dilatation: implications for the assessment of endothelial function. J Physiol 568:357–369
Anderson TJ, Uehata A, Gerhard MD et al (1995) Close relation of endothelial function in the human coronary and peripheral circulations. J Am Coll Cardiol 26:1235–1241
Black MA, Cable NT, Thijssen DH et al (2008) Importance of measuring the time course of flow-mediated dilatation in humans. Hypertension 51:203–210
Donald AE, Halcox JP, Charakida M et al (2008) Methodological approaches to optimize reproducibility and power in clinical studies of flow-mediated dilation. J Am Coll Cardiol 51:1959–1964
Joannides R, Haefeli WE, Linder L et al (1995) Nitric oxide is responsible for flow-dependent dilatation of human peripheral conduit arteries in vivo. Circulation 91:1314–1319
Green DJ, Jones H, Thijssen D et al (2011) Flow-mediated dilation and cardiovascular event prediction: does nitric oxide matter? Hypertension 57:363–369
Benjamin EJ, Larson MG, Keyes MJ et al (2004) Clinical correlates and heritability of flow-mediated dilation in the community: the Framingham Heart Study. Circulation 109:613–619
Juonala M, Kahonen M, Laitinen T et al (2008) Effect of age and sex on carotid intima-media thickness, elasticity and brachial endothelial function in healthy adults: the cardiovascular risk in Young Finns Study. Eur Heart J 29:1198–1206
Celermajer DS, Sorensen KE, Bull C et al (1994) Endothelium-dependent dilation in the systemic arteries of asymptomatic subjects relates to coronary risk factors and their interaction. J Am Coll Cardiol 24:1468–1474
Leeson CPM, Whincup PH, Cook DG et al (1997) Flow-mediated dilation in 9- to 11-year-old children: the influence of intrauterine and childhood factors. Circulation 96:2233–2238
Skilton MR, Viikari JS, Juonala M et al (2011) Fetal growth and preterm birth influence cardiovascular risk factors and arterial health in young adults: the cardiovascular risk in young Finns study. Arterioscler Thromb Vasc Biol 31:2975–2981
Hashimoto M, Eto M, Akishita M et al (1999) Correlation between flow-mediated vasodilatation of the brachial artery and intima-media thickness in the carotid artery in men. Arterioscler Thromb Vasc Biol 19:2795–2800
Halcox JP, Donald AE, Ellins E et al (2009) Endothelial function predicts progression of carotid intima-media thickness. Circulation 119:1005–1012
Celermajer DS, Adams MR, Clarkson P et al (1996) Passive smoking and impaired endothelium-dependent arterial dilatation in healthy young adults. N Engl J Med 334:150–154
Sorensen KE, Celermajer DS, Georgakopoulos D et al (1994) Impairment of endothelium-dependent dilation is an early event in children with familial hypercholesterolemia and is related to the lipoprotein(a) level. J Clin Invest 93:50–55
Hingorani AD, Cross J, Kharbanda RK et al (2000) Acute systemic inflammation impairs endothelium-dependent dilatation in humans. Circulation 102:994–999
Clarkson P, Adams MR, Powe AJ et al (1996) Oral l-arginine improves endothelium-dependent dilation in hypercholesterolemic young adults. J Clin Invest 97:1989–1994
Raitakari OT, Adams MR, McCredie RJ et al (1999) Arterial endothelial dysfunction related to passive smoking is potentially reversible in healthy young adults. Ann Intern Med 130:578–581
Selamet Tierney ES, Newburger JW, Gauvreau K et al (2009) Endothelial pulse amplitude testing: feasibility and reproducibility in adolescents. J Pediatr 154:901–905
Tagawa T, Imaizumi T, Endo T et al (1994) Role of nitric oxide in reactive hyperemia in human forearm vessels. Circulation 90:2285–2290
Nohria A, Gerhard-Herman M, Creager MA et al (2006) Role of nitric oxide in the regulation of digital pulse volume amplitude in humans. J Appl Physiol 101:545–548
Higashi Y, Sasaki S, Nakagawa K et al (2001) A noninvasive measurement of reactive hyperemia that can be used to assess resistance artery endothelial function in humans. Am J Cardiol 87:121–125
Kuvin JT, Patel AR, Sliney KA et al (2003) Assessment of peripheral vascular endothelial function with finger arterial pulse wave amplitude. Am Heart J 146:168–174
Bonetti PO, Pumper GM, Higano ST et al (2004) Noninvasive identification of patients with early coronary atherosclerosis by assessment of digital reactive hyperemia. J Am Coll Cardiol 44:2137–2141
Rubinshtein R, Kuvin JT, Soffler M et al (2010) Assessment of endothelial function by non-invasive peripheral arterial tonometry predicts late cardiovascular adverse events. Eur Heart J 31:1142–1148
de Berrazueta JR, Guerra-Ruiz A, García-Unzueta MT et al (2010) Endothelial dysfunction, measured by reactive hyperaemia using strain-gauge plethysmography, is an independent predictor of adverse outcome in heart failure. Eur J Heart Fail 12:477–483
Mahmud FH, Earing MG, Lee RA et al (2006) Altered endothelial function in asymptomatic male adolescents with type 1 diabetes. Congenit Heart Dis 1:98–103
Duck MM, Hoffman RP (2007) Impaired endothelial function in healthy African-American adolescents compared with Caucasians. J Pediatr 150:400–406
Laurent S, Cockcroft J, Van Bortel L et al (2006) Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J 27:2588–2605
Hansen TW, Li Y, Staessen JA et al (2008) Independent prognostic value of the ambulatory arterial stiffness index and aortic pulse wave velocity in a general population. J Hum Hypertens 22:214–216
Laurent S, Boutouyrie P, Asmar R et al (2001) Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 37:1236–1241
Im JA, Lee JW, Shim JY et al (2007) Association between brachial-ankle pulse wave velocity and cardiovascular risk factors in healthy adolescents. J Pediatr 150:247–251
Niboshi A, Hamaoka K, Sakata K et al (2006) Characteristics of brachial-ankle pulse wave velocity in Japanese children. Eur J Pediatr 165:625–629
Pillsbury HC III, Hung W, Kyle MC et al (1974) Arterial pulse waves and velocity and systolic time intervals in diabetic children. Am Heart J 87:783–790
Mattace-Raso FU, van der Cammen TJ, Hofman A et al (2006) Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam Study. Circulation 113:657–663
Paini A, Boutouyrie P, Calvet D et al (2006) Carotid and aortic stiffness: determinants of discrepancies. Hypertension 47:371–376
Whincup PH, Gilg JA, Donald AE et al (2005) Arterial distensibility in adolescents: the influence of adiposity, the metabolic syndrome, and classic risk factors. Circulation 112:1789–1797
Leeson CP, Whincup PH, Cook DG et al (2000) Cholesterol and arterial distensibility in the first decade of life: a population-based study. Circulation 101:1533–1538
Mori A, Uchida N, Inomo A et al (2006) Stiffness of systemic arteries in appropriate- and small-for-gestational-age newborn infants. Pediatrics 118:1035–1041
Touboul PJ, Hennerici MG, Meairs S et al (2007) Mannheim carotid intima-media thickness consensus (2004–2006). Cerebrovasc Dis 23:75–80
Urbina EM, Williams RV, Alpert BS et al (2009) Noninvasive assessment of subclinical atherosclerosis in children and adolescents: recommendations for standard assessment for clinical research: a scientific statement from the American Heart Association. Hypertension 54:919–950
Crowe LA, Ariff B, Keegan J et al (2005) Comparison between three-dimensional volume-selective turbo spin-echo imaging and two-dimensional ultrasound for assessing carotid artery structure and function. J Magn Reson Imaging 21:282–289
Corretti MC, Anderson TJ, Benjamin EJ et al (2002) Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol 39:257–265
Higashi Y, Yoshizumi M (2003) New methods to evaluate endothelial function: method for assessing endothelial function in humans using a strain-gauge plethysmography: nitric oxide-dependent and -independent vasodilation. J Pharmacol Sci 93:399–404
Axtell AL, Gomari FA, Cooke JP (2010) Assessing endothelial vasodilator function with the Endo-PAT 2000. J Vis Exp 44:e2167
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this entry
Cite this entry
Skilton, M.R., Celermajer, D.S. (2014). Non-invasive Assessment of Arterial Structure and Function. In: Da Cruz, E., Ivy, D., Jaggers, J. (eds) Pediatric and Congenital Cardiology, Cardiac Surgery and Intensive Care. Springer, London. https://doi.org/10.1007/978-1-4471-4619-3_56
Download citation
DOI: https://doi.org/10.1007/978-1-4471-4619-3_56
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-4618-6
Online ISBN: 978-1-4471-4619-3
eBook Packages: MedicineReference Module Medicine