
Abstract
Hypertension is one of the most common pathologic entities in the world and is associated with the development and exacerbation of a variety of cardiovascular disease, as well as morbid and mortal outcomes. In this chapter, we review the pathophysiology, diagnosis, treatment, and outcomes related to hypertension.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Chronic Kidney Disease
- Obstructive Sleep Apnea
- Primary Aldosteronism
- Resistant Hypertension
- Isolate Systolic Hypertension
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Hypertension is one of the most common pathologic entities in the world and is associated with the development and exacerbation of a variety of cardiovascular disease, as well as morbid and mortal outcomes. In this chapter, we review the pathophysiology, diagnosis, treatment, and outcomes related to hypertension.
Pathophysiology and Epidemiology of Hypertension
Essential Hypertension
-
The great majority (90–95 %) of hypertension is essential hypertension (otherwise known as primary hypertension)
-
The pathophysiology of essential hypertension is incompletely understood, but is thought to related to one or more of the following
-
Changes in the sympathetic nervous system and renin angiotensin aldosterone system (RAAS)
-
Renal dysfunction
-
Genetic and environmental factors
-
-
With the decreasing price of genomic studies, the pathophysiologic mechanisms are being elucidated
Hypertension and Aging
-
Clinical and Epidemiological Importance
-
The probability of having hypertension increases with age
-
At age ≥ 70, approximately 70 % of men and women have hypertension, compared with less than 20 % among those aged ≤ 44 [1]
-
The residual lifetime risk of hypertension among persons ≥60 years who had not developed hypertension is approximately 90 % [2]
-
In the 2007–2008 NHANES data, only 50 % of all patients with hypertension were controlled to <140/90 mmHg
-
The proportion of patients with controlled hypertension was lower among those ≥60 years than in younger (<40) individuals [3]
-
There is a wealth of evidence that antihypertensive pharmacologic therapy decreases mortal and morbid clinical events
-
Even in the very old, antihypertensive therapy decreases mortality
-
In the HYVET clinical trial of patients with hypertension (mean age 83.6 years), indapamide/perindopril therapy resulted in decreased mortality and was well tolerated [4]
-
-
-
Differences in Systolic and Diastolic Blood Pressure
-
With increasing age, systolic blood pressure (SBP) increases in all populations studied
-
Diastolic blood pressure (DBP) increases until approximately the fifth or sixth decade and declines thereafter ([5], Fig. 5-1)
Figure 5-1 
Changes in systolic and diastolic blood pressure with age (Used with permission from Burt et al. [5])
-
The increase of blood pressure (BP) with age is more pronounced in women ([6], Fig. 5-2)
Figure 5-2 
SBP by gender, age, and World Health Organization (WHO) subregion (Used with permission from Lawes et al. [6])
-
-
Isolated Systolic Hypertension (ISH)
-
The great majority of older patients with hypertension have ISH, with diastolic hypertension occurring in a minority (10 % among those aged 70)
-
ISH is primarily due to decreased compliance of the large arteries and increased pulse wave velocity
-
Age-related changes in the histology of the large vessels (especially the aorta) with a decrease in elastic fibers and replacement with collagen result in increased aortic wall stiffness and decreased compliance [5]
-
-
-
ISH is a result of the following phenomena ([7], Fig. 5-3):
Figure 5-3 
Effect of arterial stiffening on pulse wave velocity, reflected pressure waves and central arterial pressure in younger and older persons. PWV pulse wave velocity (Modified from Asmar [7])
-
Increased pulse pressure (due to central arterial stiffness) for a given stroke volume, with higher SBP and lower DBP
-
High pulse wave velocity, which results in the reflected pulse waves arriving at the central aorta during systole rather than after the dicrotic notch (as occurs in younger individuals)
-
Endothelial dysfunction, which results in impaired flow-mediated arterial dilation
-
-
These physiologic and pathologic effects of aging are modulated to a significant extent by behavioral and environmental influences including physical activity, diet (e.g. caloric and sodium intake, low potassium intake, atherogenic diet, etc.) [8, 9].
-
-
Additional Differences with Aging
-
The autonomic nervous system undergoes significant changes with aging
-
Downregulation and decreased responsiveness of beta-receptors and increased ambient catecholamine concentrations
-
The increased norepinephrine concentrations common in older individuals may be due to homeostatic mechanisms counterbalancing decreased responsiveness of the adrenergic receptors [10]
-
-
Elderly hypertensives usually have low renin, low aldosterone, salt-sensitive hypertension because of decreased natriuretic activity of the nephrosclerotic kidney and increased sodium reabsorption [11]
-
Renal function declines with age
-
Between the ages of 30 and 85, approximately one quarter of the cortex is lost due to glomerulosclerosis and interstitial fibrosis with impairment of renal hemodynamics [12]
-
Renal changes from nephrosclerosis and changes of the juxtaglomerular apparatus result in low renin and aldosterone levels. This may be related to expansion of total body water and suppression of renin activity [13]
-
The decreased renal function in hypertension may impair excretion of medications or their metabolites, especially in the elderly with polypharmacy and associated comorbidities (e.g. coronary heart disease (CHD), diabetes, dyslipidemia, and osteoarthritis)
-
-
Renal dysfunction predicts cardiovascular (CV) outcomes and mortality in older hypertensives [14]
-
-
Polypharmacy
-
Polypharmacy and cost result in decreased adherence to therapy
-
Polypharmacy in combination with decreased renal function increases the probability of drug interactions and adverse events
-
-
Non-steroidal anti-inflammatory agents (NSAIDs)
-
There is increased use of NSAIDs among older patients (see Drug-Induced Hypertension)
-
-
Orthostatic hypotension
-
Related to impaired baroreflex function (probably also related to stiffening of the carotid arteries [15]), venous insufficiency, varicosities, and diabetic neuropathy
-
A significant problem, especially in older hypertensives
-
Orthostatic hypotension is a predictor of poor outcomes in older individuals, and when compounded by changes in skeletal health and impaired equilibrium, may cause falls
-
-



Secondary Hypertension
-
Acute Kidney Disease
-
Acute glomerular disease may result in volume retention and hypertension due to increased sodium reabsorption
-
Acute vascular injury due to vasculitis or connective tissue disease (e.g. SLE, scleroderma) may induce hypertension by increased activation of the RAAS triggered by ischemia
-
-
Chronic Kidney Disease (CKD)
-
Many causes of CKD may lead to hypertension through sodium retention and volume expansion, increased activity of the RAAS due to ischemia, and enhanced sympathetic tone
-
-
Renovascular Hypertension
-
Most common form of secondary hypertension
-
Usually related to renal artery stenosis (RAS) due to atherosclerosis of the large renal arteries or their ostia
-
When stenosis exceeds 70 % of the diameter (about 90 % reduction in cross-sectional area), a hemodynamically significant decrease in blood flow results in decrease of intraglomerular pressure with subsequent activation of the RAAS and increased sodium reabsorption
-
-
RAS is a manifestation of widespread atherosclerosis that may involve other arterial beds (cerebrovascular, coronary, peripheral)
-
Stenoses of renal arteries, detected by invasive or non-invasive diagnostic modalities are not uncommon in the elderly, but these may be incidental and non-hemodynamically-significant
-
In addition to controlling hypertension, revascularization of significant RAS should improve GFR or slow the decline of renal function if the stenosis is the primary cause of renal dysfunction, which is not always the case [18]
-
In clinical trials of patients with RAS, there has not been a marked clinical benefit from revascularization procedures
-
-
-
Primary Aldosteronism (PA)
-
Relatively common cause of resistant hypertension (hypertension despite the use of at least three antihypertensives)
-
Usually associated with adrenal hyperplasia (usually bilateral) or an adrenal adenoma
-
May also be caused by familial hyperaldosteronism, adrenal carcinoma, or ectopic aldosterone-producing tumors
-
Diagnostic clues include suppressed plasma renin activity, high aldosterone, and hypokalemia (may not be present) in a hypertensive patient [19]
-
Diagnostic approach includes measurement of
-
Plasma renin activity (PRA), plasma renin concentration (PRC), and plasma aldosterone concentration (PAC), as well as random plasma aldosterone concentration-to-plasma renin activity (PAC/PRA) ratio
-
PAC/PRA ratio > 25 suggests PA, while normal and hypertensives without PA have ratios < 10
-
-
If PAC/PRA ratio suggests PA, one or more confirmatory tests should be performed, including [20]
-
Measurement of urinary aldosterone excretion after oral sodium chloride loading (>12 μg/24 h after 200 mmol/day (∼6 g/day) sodium intake suggests PA)
-
Measurement of PAC after IV sodium chloride loading (PAC > 10 ng/dL) after infusion of 2 L normal saline over 4 h suggests PA
-
Fludrocortisone suppression test (upright PAC > 6 ng/dL after 4 days suggests PA)
-
Captopril challenge (PAC, normally suppressed by 25–50 mg of captopril, remains elevated in PA, while PRA remains low)
-
Certain medications (e.g. aldosterone receptor antagonists (ARA)) must be held during testing
-
-
If confirmatory tests are positive, patients should undergo adrenal CT
-
Selective adrenal vein sampling may be used to distinguish unilateral from bilateral adrenal involvement in cases where surgery (unilateral adrenalectomy) is an option
-
For unilateral adrenal involvement or for extra-adrenal lesions, surgical resection is often primary therapy
-
Medical treatment (e.g. for bilateral adrenal hyperplasia) is based on the use of ARAs
-
-
Thyroid Disease
-
Both hyperthyroidism and hypothyroidism may be associated with hypertension.
-
-
Cushing’s Syndrome
-
Increased ACTH levels, whether iatrogenic, from adrenal tumors, or from other paraneoplastic activity, can lead to hypertension, which may be severe
-
-
Pheochromocytomas
-
Rare catecholamine-producing tumors that can cause paroxysmal hypertension
-
-
Aortic Coarctation
-
Relatively common congenital abnormality that leads to predominately upper-extremity hypertension secondary to mechanical obstruction (typically distal to the brachiocephalic circulation)
-
-
Obstructive sleep apnea (OSA)
-
Associated with an increased incidence of hypertension
-
OSA should be treated due to a variety of sequelae, including fatigue, systemic and pulmonary hypertension, and all-cause and CAD-related mortality
-
May be related to other conditions (e.g. obesity and dyslipidemia) and to morbid events (e.g. HF and stroke) [21]
-
-
-
Drug-Induced Hypertension
-
Medication use is an important cause of secondary hypertension
-
Causes include NSAIDs, stimulants, and sympathomimetic decongestant agents and oral contraceptive pills.
-
NSAIDs exert anti-inflammatory activity by inhibiting the production of prostaglandins that mediate inflammation. This inhibition, however, may result in decreased renal function, sodium and water retention, BP elevation, and HF
-
NSAIDs may impair the BP-lowering effect of ACE inhibitors, ARBs, and diuretics [22, 23]
-
-
-
Diagnosis of Hypertension
Techniques
-
Blood pressure, especially SBP in elderly individuals, exhibits variability with successive BP measurements and environmental changes such as temperature and emotional state
-
It is important to measure the pressure several times in a comfortable position after sitting for 5 min
-
Orthostatic changes should be ascertained by measuring the pressure after standing for 1–3 min
-
-
Pseudohypertension, a measurement of a high BP value in the presence of normal intraluminal BP because of noncompressible arteries
-
May occur in older individuals, but is uncommon
-
The Osler maneuver (palpable radial or brachial artery when the cuff is inflated above SBP), may be used, although sensitivity and specificity are not very high
-
Definitive diagnosis requires intraarterial measurement
-
-
Home BP monitoring
-
Should be performed using a reliable automated device
-
Measurements made three times in the morning and three times in the evening for seven consecutive days
-
An inexpensive and reliable method of monitoring antihypertensive therapy
-
-
Ambulatory BP is a predictor of target organ damage as well as outcomes that surpasses office BP [24]
-
Ambulatory BP measurement is now recommended in the National Institute for Health and Clinical Excellence (UK) guidelines to confirm the diagnosis following an initial elevated BP measurement in the clinic [25]
Association with Risk
-
Data from the Framingham Study have shown that in younger ages, DBP is more important in determining risk of CHD while in older individuals, the risk primarily is determined by SBP ([26], Fig. 5-4)
Figure 5-4 
Relative importance of DBP and SBP as predictors of CHD as a function of age. CHD coronary heart disease (Used with permission from Franklin et al. [26])
-
In older patients, lower DBP is associated with higher risk
-
Studying persons aged 50–79 years without clinical evidence of CHD, the investigators reported that CHD risk increased with lower DBP for a given SBP, suggesting that higher pulse pressure determines the risk in older individuals ([27], Fig. 5-5)
Figure 5-5 
Joint influences of SBP and pulse pressure on CHD risk (Used with permission from Franklin et al. [27])
-
This relationship could be explained by
-
Decreased coronary flow
-
A stiffer aortic reservoir related to older age
-
Comorbidities (e.g. diabetes)
-
Lifestyle factors (e.g. smoking)
-


Sequelae of Hypertension
Target Organ Damage
-
Hypertension results in damage to the arterial system, brain, heart, eyes, and kidneys.
-
Peripheral arterial disease (PAD) is frequently associated with hypertension
-
PAD is likely to occur in the same patients who have cerebrovascular disease and CHD and is associated with a marked increase in the occurrence of acute myocardial infarction (MI) and stroke
-
-
Hypertension is an important risk factor for the development of abdominal and thoracic aortic aneurysm and aortic dissection
-
The probability is increased among smokers and those with connective tissue disorders
-
BP control is very important and surgery is necessary when the aneurysms reach specific dimensions since mortality following rupture is extremely high
-
-
Hypertensive retinopathy with arteriovenous nicking, arteriolar narrowing, and in some cases hemorrhages, exudates, and papilledema increases in frequency with age and SBP [28]
-
Diabetes mellitus (DM), a current worldwide epidemic, increases the risk in hypertensive patients and interacts with hypertension in causing CV events, CKD, and HF [29, 30]
-
Obesity, another public health issue, is related to and may be causative of diabetes, with the majority of the population being either obese (BMI >30) or overweight (BMI > 25) [31]
-
Morbid and Mortal Events
-
Hypertension accounts for more attributable deaths worldwide than any other risk factor, whereas smoking and high cholesterol are second and third, respectively [32]
-
The causes of death related to hypertension are CHD, stroke, HF, and CKD, especially when hypertension coexists with diabetes ([33], Fig. 5-6)
Figure 5-6 
Elevated SBP is a strong risk factor for cardiovascular mortality (Used with permission from Flack et al. [33])
-
Age is a major determinant of risk for both stroke and CHD events
-
BP tends to increase with age and the relative risk imposed by a given BP level decreases with age
-
However, because of the higher baseline risk (risk at SBP of 110 mmHg), the absolute increase in risk due to a given level of hypertension is much higher at older ages
-
For patients aged 50–59, the relative risk for fatal stroke is approximately 16 for patients with SBP of 180 mmHg compared to those with SBP of 110 mmHg, while for patients aged 80–89, the relative risk is approximately 2
-
On the other hand, the increase in absolute risk for mortality from stroke is 15 (from 1 to 16) for the younger age group and about 75 for the older age group ([34], Fig. 5-7, left panel). Similar increases in mortality from CHD are seen with increasing age and BP (Fig. 5-7, right panel). These linear-log plots demonstrate the exponential relationship of a given SBP to risk.
Figure 5-7 
Cardiovascular disease mortality with increasing SBP by age (Used with permission from Lewington et al. [34])
-
-
-
Similarly, the relationship of age to mortality risk for any given level of BP can be redrawn with other risk factors (e.g. total cholesterol, LDL), alone or in combination, substituted for age
-
Hypertension, when it is the only risk factor (usually in a young person), imparts a small or moderate risk of cardiovascular and renovascular events
-
It is the combined presence of additional risk factors interacting with age that increase the risk ([35], Fig. 5-8)
Figure 5-8 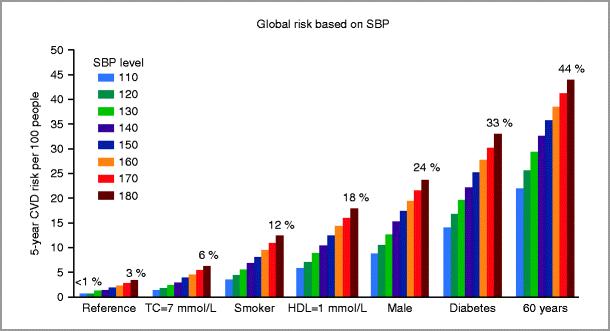
Global risk as a function of SBP interacting with other risk factors (Used with permission from Jackson et al. [35])
-
-
Among risk factors, obesity and diabetes have become an epidemic in the U.S. and worldwide
-
There are 285 million people with diabetes worldwide. This number will increase to 438 million by the year 2030 [36]
-
The great majority have type 2 diabetes that is related to obesity and frequently coexists with hypertension
-
Diabetes markedly increases the risk of CV events at any level of BP [37]
-
One way to visualize the effect of diabetes is presented in Fig. 5-9 (modified from [38])
Figure 5-9 
Effect of diabetes and age on risk of cardiovascular events (Modified from Booth et al. [38])
-




Hypertension and Heart Failure
-
Left ventricular systolic dysfunction (LVSD) and HF are common complications of aging and hypertension, in part because of increased survival after MI
-
Hypertension may result in HF via two pathways:
-
The development of acute MI leading to HF with impaired LV systolic function
-
The development of left ventricular hypertrophy (LVH) leading to HF with preserved EF (HFPEF), probably related to diastolic dysfunction
-
Patients with HFPEF tend to have concentric left ventricular (LV) remodeling with high LV mass/volume ratio as well as cardiomyocyte hypertrophy
-
Those with HF with reduced EF (HFREF) tend to have eccentric LV remodeling with low LV mass/volume ratio with loss of myofibers [39]
-
-
-
Hypertension, when untreated, results in increased LV wall thickness and decreased diastolic function causing impaired early diastolic filling due to delayed myocardial relaxation and decreased passive mid-diastolic filling due to a stiffer left ventricle
-
Decreased diastolic filling and afterload mismatch may cause HFPEF. The impedance mismatch can result in flash acute pulmonary edema.
-
-
Treatment of ISH with chlorthalidone-based stepped therapy resulted in marked decrease in the occurrence of HF in the Systolic Hypertension in the Elderly Program (SHEP) [40]
-
The occurrence of HF was related to SBP, as expected, but also to pulse pressure, after accounting for SBP.
-
This may be due to concomitant and parallel decreases in both large artery and left ventricular compliance or potentially to a decrease in coronary flow related to low DBP [41].
-
-
Uncontrolled hypertension and aging interact to exacerbate the development of HF, especially in the presence of obesity or diabetes, which further contribute to increased LV mass, LV wall thickness, and abnormal diastolic LV filling patterns
-
Impairment of systolic function is initially compensated for by increased LV thickness, but ultimately, LV remodeling associated with neurohormonal activation, increased wall tension, apoptosis, myocyte loss, fibrosis, chamber dilatation, and depressed systolic function leads to HF
-
In the Cardiovascular Health Study, LVSD in the absence of HF was associated in a graded fashion with higher incidence of future clinical HF, as well as with higher mortality [42]
-
-
Prevention of HF is a major objective of antihypertensive therapy.
-
Controlling hypertension prevents LV hypertrophy and acute MI, both of which reduce the incidence of HF
-
-
HF is associated with neurohormonal activation involving the sympathetic, endothelin, vasopressin, and renin-angiotensin systems, which maintain and worsen the myocardial changes described above, while at the same time contribute to inadequate peripheral circulatory adaptation
Treatment of Hypertension
General Guidelines
-
Nonpharmacologic therapy and lifestyle modification are important in treating hypertension
-
Nonpharmacologic therapy may delay the need for pharmacologic therapy in some and may facilitate control of BP with lower doses or lower number of medications in most patients [43, 44]
-
Weight loss, sodium reduction, and their combination were found useful in controlling hypertension without pharmacotherapy in older hypertensive patients who needed one or two medications for control in TONE
-
The combination was more effective than either of the two interventions alone [45]
-
Patients randomized to sodium restriction maintained their improved dietary habits even 5 years after discontinuing contact with the clinical trial center, while this was not true for caloric restriction and weight loss [46]
-
Excessive alcohol consumption is associated with increased BP, probably resulting from sympathetic activation and cortisol increase
-
-
-
The effect of antihypertensive therapy in decreasing cardiovascular events is more pronounced when the BP drop is bigger ([47], Fig. 5-10)
Figure 5-10 
Odds ratio of stroke based on SBP difference achieved between randomized groups (Used with permission from Turnbull et al. [47])

Differing Patient Subsets
-
Among the medications approved for control of hypertension, diuretics, calcium channel blockers (CCBs), ACE inhibitors (ACEI), and beta blockers (BB) may be used as a first line drug in patients with hypertension (Table 5-1)
Table 5-1 Drug treatment of arterial hypertension in patients with coexisting conditions -
A number of coexisting conditions as well as demographic differences may alter the preferred agents used to treat hypertension and the BP targets to be achieved
-
Adverse effects of medications become important in different patient subsets (e.g. bronchospastic disease for beta-blockers)
-
The use of diuretics in treating hypertension in older people is associated with hyperglycemia, compared to CCBs, which have a neutral effect, and to agents affecting the renin angiotensin system which are associated with lower glucose concentrations [48, 49]
-
The hyperglycemia associated with chlorthalidone in the Systolic Hypertension in the Elderly Program (SHEP) was not associated with impaired outcomes compared to patients who had diabetes at baseline at 14-year follow-up [50]
-
Thiazide-type diuretics produce hyperglycemia in part by impaired insulin release related to hypokalemia rather than through insulin resistance, the common mechanism of diabetes in older adults [51, 52]
-
-
Gout is another adverse effect associated with thiazide diuretics and both hypertension and diuretic use increase the chance of developing this condition [53]
-
-
Treatment targets
-
The Seventh Report of the Joint National Commission (JNC), JNC 7 guidelines for antihypertensive treatment targets [43] include:
-
General: <140/90 mmHg
-
DM or CKD: 130/80 mmHg
-
CHD or CVA: There is no unanimity on different BP targets in these populations
-
-
-
The ACCF/AHA 2011 expert consensus document suggests a comprehensive approach to treatment ([54], Fig. 5-11)
Figure 5-11 
Algorithm for treatment of hypertension in the elderly (Used with permission from Aronow et al. [54])
-
Special considerations
-
In the U.S., older Black Americans have more severe hypertension and have high rates of stroke, LVH and CKD [43]
-
Blacks in NHANES III were less likely to have their BP controlled. They are also more likely to have diabetes and increased BMI.
-
Blacks are more likely high-volume/low-renin hypertensives, and hence diuretics as well as CCB may be reasonable agents to start with, however responsiveness to ACEI and ARB remains in this patient subgroup, so their use should not be discouraged.
-
-
Controlling hypertension alone is not sufficient since other risk factors (e.g. hypercholesterolemia, diabetes, and smoking) have an additive and possibly multiplicative effect in causing cardiovascular disease
-
In the TNT clinical trial, the best outcomes were observed among patients in the lowest SBP and lowest LDL tertiles [55]
-
-
While tight blood pressure control is desirable in advanced CKD, the use of ACEI plus ARBs, or ACE (or ARB) plus aliskerin (a direct renin inhibitor) is to be avoided, given the risk of hypotension, hyperkalemia, and risk for progressive renal failure.
-

Resistant Hypertension
-
BP above goal despite the concurrent use of 3 antihypertensive medications of different classes
-
Occurs in about 20–30 % of patients
-
Causes include secondary hypertension, such as renal artery stenosis, as well as medication induced hypertension
-
-
More common in older and obese patients
-
Carries high CV risk as it is associated with severe hypertension, DM, CKD.
-
Pseudoresistance refers to lack of control due to poor adherence, white coat hypertension, lack of appropriate medication dose titration, etc.
-
Clinical evidence suggests that addition of a thiazide diuretic and/or ARA in those with resistant hypertension is an effective intervention
-
Additional antihypertensive classes that may be helpful as third-fifth line agents include
-
Aldosterone receptor antagonists (ARA) (e.g. spironolactone, eplerenone), with particular benefit in HF
-
Centrally-acting alpha-2 agonists (e.g. clonidine, alpha-methyldopa (also useful during pregancy or for pregnancy-induced hypertension due to lack of teratogenicity))
-
Alpha-blocking agents (e.g. doxazosin (had higher incidence of HF in ALLHAT), phentolamine (for hypertensive emergency))
-
Hydralazine, a peripheral vasodilator, has been shown to be especially effective in combination with BB or spironolactone
-
Minoxidil (another peripheral vasodilator) is also used to prevent hair loss
-
Severe/Malignant Hypertension and Hypertensive Crises
-
Hypertensive crisis refers the sudden or rapid development of severe hypertension (SBP ≥180 mmHg and/or DBP ≥120 mmHg)
-
Hypertensive crises tend to occur among patients with poor medication adherence, acute sodium load
-
A hypertensive crisis constitutes a hypertensive emergency when the patient develops acute complications, including
-
Retinal hemorrhages, exudates, or papilledema.
-
Renal involvement (malignant nephrosclerosis, proteinuria, hematuria)
-
Hypertensive encephalopathy with cerebral edema; may cause headache, nausea vomiting, confusion, seizures, coma
-
This may predominantly affect the posterior circulation, presenting with a reversible leukoencephalopathy
-
-
Stroke (ischemic or hemorrhagic)
-
Myocardial ischemia or infarction
-
Aortic dissection
-
-
Management of hypertensive emergency involves immediate control of BP using sodium nitroprusside, clevidipine, nicardipine, or labetalol
-
Lower DBP initially by up to 25 %
-
Aim for DBP 100–105 mmHg within 6–8 h
-
Avoid lowering SBP below 160 mmHg in the acute setting (given change in cerebral autoregulation)
-
Exception: aortic dissection, where goals are SBP 120 mmHg, MAP 80 mm, achieved over 5–10 min
-
Reduce blood pressure to goal on oral medications, gradually over 2–3 months
-
-
Hypertensive urgency refers to a hypertensive crisis without symptoms or the above acute target organ damage
-
Reduce blood pressure more gradually, over 24–48 h
-
Review Questions
-
1.
The preferred treatment strategies for nephroprotection in patients with diabetes are:
-
(a)
ACE inhibition
-
(b)
Angiotensin receptor blockade
-
(c)
Direct renin inhibition
-
(d)
Aldosterone antagonist
-
(e)
All of the above
-
(f)
a and b only
-
(a)
-
2.
Potential testing methodologies for hyperaldosteronism include:
-
(a)
Aldosterone levels after IV sodium chloride loading
-
(b)
Aldosterone levels after high dose oral salt intake
-
(c)
Selective adrenal vein sampling
-
(d)
Supine and upright posture renin-aldosterone profiling
-
(e)
All of the above
-
(a)
-
3.
Initial therapies for the treatment of essential hypertension may include:
-
(a)
Thiazide diuretics
-
(b)
Beta blockers
-
(c)
ACE inhibitors
-
(d)
Angiotensin receptor blockers
-
(e)
Calcium channel blockers
-
(f)
Alpha adrenergic blockers
-
(g)
All of the above
-
(h)
All of the above except f
-
(a)
-
4.
In patients with renovascular hypertension, the following drugs are contraindicated:
-
(a)
ACE inhibitors
-
(b)
Angiotensin receptor blockers
-
(c)
Direct renin inhibitors
-
(d)
All of the above
-
(e)
None of the above
-
(a)
Answers
-
1.
(f) Control hypertension in diabetics to below 140/90 mmHg and. with less strong evidence but recommended by the JNC7 and ADA guidelines, to below 130/80. ACEI have been shown to confer nephroprotection in patients with both type 1 and type 2 DM, where they slow progression of microalbuminuria and may decrease blood glucose and the progression of retinopathy. There is a wealth of evidence supporting the use of ARBs in DM. Clinical trials such as RENAAL (losartan) and IDNT (irbesartan) showed evidence of nephroprotection in patients with DM type 2 and nephropathy. The ALTITUDE clinical trial of aliskiren vs. placebo on background therapy of ACEI or ARB in patients with type 2 DM and renal impairment was stopped by the DSMB because of higher rate of adverse events without benefit with the direct renin inhibitor alikiren. Although spironolactone and eplerenone have shown mortality benefits in patients with HF and CHD and these agents may be included in combination therapy of hypertensive patients with DM, there are no large clinical trials demonstrating nephroprotection. A presumed superiority of ACEI and ARB on cardiovascular and all-cause mortality in patients with DM has not been proven in large clinical trials such as ALLHAT or meta-analyses.
-
2.
(e) Common diagnoses to consider are bilateral adrenal hyperplasia and aldosterone-producing adenomas, but ectopic aldosterone-producing tumors, familial hyperaldosteronism types 1 and 2, and aldosterone-producing adrenocortical carcinomas should also be considered. Aldosterone levels after IV sodium chloride loading (2 L of isotonic saline over 4 h) in a patient who is resting lying down as well as aldosterone levels after high dose oral salt intake (200 mmol (∼6 g) sodium diet for 3 days) may be used to confirm primary hyperaldosteronism. Lack of suppression of the plasma aldosterone concentration to below 10 ng/dL (277 pmol/L) or urine aldosterone excretion >12 mcg/24 h (33 nmol/day) are consistent with primary aldosteronism. Selective adrenal vein sampling is the most definitive way to differentiate between bilateral adrenal hyperplasia and unilateral aldosterone producing adenomas. In the latter, there is more than 4-fold difference in venous plasma aldosterone concentration between the two sides, while there is no significant difference in the former. This test is ordinarily performed before surgery, especially when a diagnosis cannot be made by CT or other means. Each of the tests listed would likely follow initial screening with PAC/PRA testing.
-
3.
(h) All the antihypertensive drug classes listed above include effective first-line antihypertensive medications with exception of alpha adrenergic blockers. Doxazocin, an example of the latter class was associated with high (double) rate of occurrence of heart failure compared to chlorthalidone in ALLHAT. The other medication classes result in control of BP to <140/90 in about 50–70 % of the cases as monotherapy. The choice among classes is guided by demographics, comorbidities, and adverse effects.
-
4.
(e) ACEI and ARB are effective in controlling BP alone or in combination with diuretics or CCBs. A major problem is a decrease in intraglomerular pressure due to ACEI/ARB-induced dilatation of the efferent arterioles with decrease in GFR and increase in serum creatinine (which should be monitored). Progression of the stenosis(es) and loss of renal parenchyma with worsening of renal function are additional concerns.
Abbreviations
- ACEI:
-
Angiotensin Converting Enzyme inhibitors
- ARA:
-
Aldosterone receptor antagonists
- ARB:
-
Angiotensin receptor blockers
- BB:
-
Beta blockers
- BP:
-
Blood pressure
- CCB:
-
Calcium channel blockers
- CHD:
-
Coronary heart disease
- CKD:
-
Chronic kidney disease
- CV:
-
Cardiovascular
- DBP:
-
Diastolic blood pressure
- DM:
-
Diabetes mellitus
- HF:
-
Heart failure
- ISH:
-
Isolated systolic hypertension
- LVH:
-
Left ventricular hypertrophy
- LVSD:
-
Left ventricular systolic dysfunction
- MI:
-
Myocardial infarction
- PA:
-
Primary aldosteronism
- PAC:
-
Plasma aldosterone concentration
- PAD:
-
Peripheral arterial disease
- PRA:
-
Plasma renin activity
- PRC:
-
Plasma renin concentration
- RAAS:
-
Renin angiotensin aldosterone system
- SBP:
-
Systolic blood pressure
- WHO:
-
World Health Organization
References
Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics—2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:e21–181.
Vasan RS, Beiser A, Seshadri S, et al. Residual lifetime risk for developing hypertension in middle-aged women and men. The Framingham Heart Study. JAMA. 2002;287:1003–10.
Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303(20):2043–50.
Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358:1887–98.
Burt VL, Whelton P, Roccella EJ, et al. Prevalence of hypertension in the U.S. adult population: results from the Third National Health and Nutrition Examination Survey, 1988–1991. Hypertension. 1995;25:305–13.
Lawes CMM, Vander Hoorn S, Law MR, Elliott P, MacMahon S, Rodgers A. Blood pressure and the global burden of disease 2000. Part 1: estimates of blood pressure levels. J Hypertens. 2006;24(3):413–22.
Asmar R. Arterial stiffness and pulse wave velocity: clinical applications. Paris: Elsevier; 1999.
Vaitkevicius PV, Fleg JL, Engel JH, et al. Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation. 1993;88:1456–62.
Celermajer DS, Sorensen KE, Spiegelhalter DJ, et al. Aging is associated with endothelial dysfunction in healthy men years before the age-related decline in women. J Am Coll Cardiol. 1994;24:471–6.
Fleg JL. Effects of aging on the cardiovascular system. In: ACCSAP 6. Washington, D.C.: American College of Cardiology; 2005. p. 6–20.
Fotherby MD, Potter JF. Effects of moderate sodium restriction on clinic and twenty-four-hour ambulatory blood pressure in elderly hypertensive subjects. J Hypertens. 1993;11:657–63.
Beck LH. The aging kidney: defending a delicate balance of fluid and electrolytes. Geriatrics. 2000;55:26–8.
Fliser D, Ritz E. Relationship between hypertension and renal function and its therapeutic implications in the elderly. Gerontology. 1998;44:123–31.
Fried LF, Shlipak MG, Crump C, et al. Renal insufficiency as a predictor of cardiovascular outcomes and mortality in elderly individuals. J Am Coll Cardiol. 2003;41:1364–72.
Masaki KH, Schatz IJ, Burchfiel CM, et al. Orthostatic hypotension predicts mortality in elderly men: the Honolulu Heart Program. Circulation. 1998;98:2290–5.
Levin A, Linas S, Luft FC, et al. Controversies in renal artery stenosis: a review by the American Society of Nephrology Advisory Group on Hypertension. Am J Nephrol. 2007;27:212–20.
Kendrick J, Chonchol M. Renal artery stenosis and chronic ischemic nephropathy: epidemiology and diagnosis. Adv Chronic Kidney Dis. 2008;15:355–62.
Pearce JD, Craven BL, Craven TE, et al. Progression of atherosclerotic renovascular disease: a prospective population-based study. J Vasc Surg. 2006;44:955–62.
Mosso L, Carvajal C, Gonzalez A, et al. Primary aldosteronism and hypertensive disease. Hypertension. 2003;42:161–5.
Funder JW, Carey RM, Fardella C, et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2008;93(9):3266–81.
Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA. 2000;283:1829–36.
Bjorkman DJ. The effect of aspirin and nonsteroidal anti-inflammatory drugs on prostaglandins. Am J Med. 1998;105:8S–12.
Koopmans PP, Thien T, Gribnau FW. The influence of ibuprofen, diclofenac and sulindac on the blood pressure lowering effect of hydrochlorothiazide. Eur J Clin Pharmacol. 1987;31:553–7.
Parati G, Stergiou GS, Asmar R, et al. European Society of Hypertension guidelines for blood pressure monitoring at home: a summary report of the Second International Consensus Conference on Home Blood Pressure Monitoring. J Hypertens. 2008;26(8):1505–26.
Krause T, Lovibond K, Caulfield M, McCormack T, Williams B, Guideline Development Group. Management of hypertension: summary of NICE guidance. BMJ. 2011;343:d4891.
Franklin SS, Larson MG, Khan SA, et al. Doses the relation of blood pressure to coronary heart disease risk change with aging? The Framingham Heart Study. Circulation. 2001;103(9):1245–9.
Franklin SS, Khan SA, Wong ND, Larson MG, Levy D. Is pulse pressure useful in predicting risk for coronary heart disease? The Framingham heart study. Circulation. 1999;100(4):354–60.
Wong TY, Mitchell P. Hypertensive retinopathy. N Engl J Med. 2004;351:2310–7.
Held C, Gerstein HC, Yusuf S, et al. Glucose levels predict hospitalization for congestive heart failure in patients at high cardiovascular risk. Circulation. 2007;115:1371–5.
Elliott WJ, Meyer PM. Incident diabetes in clinical trials of antihypertensive drugs: a network meta-analysis. Lancet. 2007;369:201–7.
Cutler JA, Sorlie PD, Wolz M, et al. Trends in hypertension prevalence, awareness, treatment, and control rates in United States adults between 1988–1994 and 1999–2004. Hypertension. 2008;52:818–27.
Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367:1747–57.
Flack JM, Neaton J, Grimm Jr R, et al. Blood pressure and mortality among men with prior myocardial infarction. Multiple Risk Factor Intervention Trial Research Group. Circulation. 1995;92(9):2437–45.
Lewington S, Clareke R, Qizilbash N, Peto R, Collins R. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–13.
Jackson R, Lawes CM, Bennett DA, Milne RJ, Rodgers A. Treatment with drugs to lower blood pressure and blood cholesterol based on an individual’s absolute cardiovascular risk. Lancet. 2005;365(9457):434–41.
Hu BH. Diet and exercise for new-onset type 2 diabetes. Lancet. 2011;387:101–2.
Opie LH. Glycemia and heart failure in diabetes types 1 and 2. Lancet. 2011;387:103–4.
Booth GL, Kapral MK, Fung K, Tu JV. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet. 2006;368:29–36.
Jessup M, Brozena S. Heart failure. N Engl J Med. 2003;348:2007–18.
Kostis JB, Davis BR, Cutler J, et al. Prevention of heart failure by antihypertensive drug treatment in older persons with isolated systolic hypertension. SHEP Cooperative Research Group. JAMA. 1997;278:212–6.
Kostis JB, Lawrence-Nelson J, Ranjan R, Wilson AC, Kostis WJ, Lacy CR. Association of increased pulse pressure with the development of heart failure in SHEP. Am J Hypertens. 2001;14(8):798–803.
Gottdiener JS, McClelland RL, Marshall R, et al. Outcome of congestive heart failure in elderly persons: influence of left ventricular systolic function. The Cardiovascular Health Study. Ann Intern Med. 2002;137:631–9.
Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC 7 report. JAMA. 2003;289:2560–72.
Mancia G, De Backer G, Dominiczak A, et al. 2007 ESH-ESC practice guidelines for the management of arterial hypertension. J Hypertens. 2007;25(9):1751–62.
Whelton PK, Appel LJ, Espeland MA, et al. Efficacy of sodium reduction and weight loss in the treatment of hypertension in older persons: main results of the randomized, controlled trial of nonpharmacologic interventions in the elderly. JAMA. 1998;279:839–46.
Kostis JB, Wilson AC, Shindler DM, Cosgrove NM, Lacy CR. Persistence of normotension after discontinuation of lifestyle intervention in the trial of TONE. Am J Hypertens. 2002;15:732–4.
Turnbull F, Blood Pressure Lowering Treatment Trialists’ Collaboration, et al. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2003;362:1527–35.
Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999;130:461–70.
Whelton PK, Barzilay J, Cushman WC, et al. Clinical outcomes in antihypertensive treatment of Type 2 diabetes, impaired fasting glucose concentration, and normoglycemia. Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Arch Intern Med. 2005;165:1401–9.
Kostis JB, Wilson AC, Freudenberger RS, Cosgrove NM, Pressel SL, Davis BR, et al. Long-term effect of diuretic-based therapy on fatal outcomes in subjects with isolated systolic hypertension with and without diabetes. Am J Cardiol. 2005;95:29–35.
Swislocki AL, Hoffman BB, Reaven GM. Insulin resistance, glucose intolerance and hyperinsulinemia in patients with hypertension. Am J Hypertens. 1989;2:419–23.
Siegel D, Saliba P, Haffner S. Glucose and insulin levels during diuretic therapy in hypertensive men. Hypertension. 1994;23:688–94.
Choi HK, Atkinson K, Karlson EW, et al. Obesity, weight change, hypertension, diuretic use, and risk of gout in men: the health professionals follow-up study. Arch Intern Med. 2005;165:742–8.
Aronow WS, Fleg JL, Pepine CJ, et al. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol. 2011;57(20):2037–114.
Kostis JB, Breazna A, Deedwania PC, LaRosa JC. The benefits of intensive lipid lowering in patients with stable coronary heart disease with normal or high systolic blood pressure: an analysis of the Treating to New Targets (TNT) Study. J Clin Hypertens. 2008;10:367–76.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
Kostis, W.J., Zusman, R.M., Zusman, R.M. (2014). Hypertension. In: Gaggin, H., Januzzi, Jr., J. (eds) MGH Cardiology Board Review. Springer, London. https://doi.org/10.1007/978-1-4471-4483-0_5
Download citation
DOI: https://doi.org/10.1007/978-1-4471-4483-0_5
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-4482-3
Online ISBN: 978-1-4471-4483-0
eBook Packages: MedicineMedicine (R0)