
Abstract
The population of adults with congenital heart disease (CHD) is rapidly growing and presently exceeds one million individuals in the United States. It is a heterogeneous patient group comprising those with previously unrecognized and untreated lesions, as well as many prior palliated or corrective interventions. Most congenital heart disease patients benefit from ongoing cardiac supervision and a substantial number require highly specialized management and further intervention [1].
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Right Ventricle
- Patent Ductus Arteriosus
- Atrial Septal Defect
- Aortic Regurgitation
- Ventricular Septal Defect
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Background
The population of adults with congenital heart disease (CHD) is rapidly growing and presently exceeds one million individuals in the United States. It is a heterogeneous patient group comprising those with previously unrecognized and untreated lesions, as well as many prior palliated or corrective interventions. Most CHD patients benefit from ongoing cardiac supervision and a substantial number require highly specialized management and further intervention [1].
-
1.
Left-to-Right Shunt Lesions
-
2.
Obstructive Lesions
-
3.
Complex Lesions
Left-To-Right Shunt Lesions
-
Atrial septal defect (ASD)
-
Epidemiology:
-
Most common congenital heart lesion in adults, female predominance
-
Rule out Holt Oram syndrome: autosomal dominant, congenital abnormality of the hand and radius, families should be screened
-
-
Types (Fig. 21-1a):
FIGURE 21-1 
Atrial septal defects. (a) Depiction of types of atrial septal defects. (b) CXR of patient with Scimitar syndrome. Anomalous pulmonary venous drainage to the IVC (arrow). (c) Four chamber view with drop out of the intraatrial septum consistent with secundum ASD (arrow). (d) Parasternal short axis view, cleft mitral valve often associated with primum ASD (arrow)
-
Secundum (65 %): varies in size, usually isolated lesion, mitral regurgitation (MR) occurs in elderly
-
Primum (10–15 %): often large and associated with cleft anterior mitral leaflet with MR
-
Sinus venosus (10–15 %): commonly associated with partial anomalous pulmonary venous drainage (superior sinus venosus defect – right upper pulmonary venous anomaly; inferior sinus venosus defect- right lower pulmonary venous anomaly: Scimitar)
-
Coronary sinus septal defects: rare, associated with complex cardiac lesions
-
-
Clinical Presentation: ASD presents with a volume load to the right atrium (RA) and right ventricle (RV)
-
Varies from asymptomatic (incidentally found), to progressive RA and RV dilation with larger defects causing supraventricular tachyarrhythmia, fatigue, exercise intolerance.
-
In older individuals (age >60): atrial fibrillation, and with a significant shunt, right heart dilation and hypocontractility. Left-to-right shunt may increase with advancing age as left ventricular (LV) compliance worsens, or systemic hypertension, MR, or LV disease develops
-
Right ventricular hypertension may lead to right –to-left shunting, hypoxemia, cyanosis and rarely paradoxical embolus.
-
Reversible flow-related pulmonary hypertension is common with large defects in older patients; irreversible pulmonary vascular obstruction is less common (Eisenmenger syndrome).
-
-
Physical exam:
-
Wide and fixed splitting of the second heart sound
-
Soft systolic pulmonary flow murmur
-
Precordial lift (RV enlargement)
-
-
ECG findings:
-
Incomplete right bundle branch block (RBBB), may progress to complete with larger shunts and age.
-
Primum defects typically have left axis deviation, sinus venosus and secundum generally have a rightward axis.
-
Sinus venosus may have a low ectopic atrial rhythm (negative p waves in leads II, III, aVF).
-
-
Chest X Ray (CXR): may reveal the curvilinear shadow of an anomalous pulmonary vein (with inferior sinus venosus defects, Scimitar sign Fig. 21-1b)
-
Echo findings:
-
Right heart enlargement.
-
Atrial septal drop out (Fig. 21-1c).
-
Main pulmonary artery (PA) enlargement and increased transpulmonic flow.
-
In primum ASD, evaluation for mitral valve (MV) anterior leaflet cleft (Fig. 21-1d) and MR is important, rule out caval type ventricular septal defect (VSD).
-
In secundum ASD, a transesophageal echocardiogram (TEE) defines location and anatomy to determine candidacy for device closure.
-
Diagnosis of sinus venosus defect difficult with 2D echo and usually requires TEE.
-
-
CT/MR: May be used for sinus venosus defect and partial vein imaging if not seen on echocardiogram.
-
Cardiac catheterization: hemodynamic assessment of pulmonary vascular resistance (PVR) and reversibility (response to pulmonary vasodilator therapy: 100 % O2, nitric oxide [NO]), and shunt calculation is essential to determine closure candidacy. In some, test balloon occlusion in the catheterization lab may facilitate decision process.
-
Management:
-
ACC/AHA Class I recommendation: closure of an ASD either percutaneously or surgically is indicated for RA or RV enlargement with or without symptoms in predominantly left-to-right shunts, or bidirectional shunting through a larger ASD with low or responsive PVR [2].
-
ACC/AHA Class III recommendation: closure not indicated if severe irreversible pulmonary hypertension (Eisenmenger physiology) [2].
-
Percutaneous closure: uncomplicated secundum defects with appropriate anatomy [3]
-
Surgical closure: large secundum ASDs, unusual anatomy, and all sinus venosus, primum ASDs and coronary sinus defects; Pre-operative imaging will define anomalous pulmonary venous drainage and MV abnormalities that may also require repair. For sinus venosus defects with anomalous pulmonary venous drainage, a Warden technique is sometimes used.
-
Post-operative complications: residual shunt, MR and atrioventricular (AV) conduction abnormality (rare, and all more likely with primum ASD repair). Sinus venosus surgical complications include sinus node dysfunction/supraventricular tachycardia (SVT), pulmonary venous obstruction at anastomosis site, and rarely superior vena cava (SVC) obstruction. Typically, RV size and function improve post operatively even in advanced age.
-
-
Pregnancy and delivery: well tolerated in most patients. Ideal to discuss and repair if needed preconception. With large bidirectional shunts, IV filters are recommended.
-
-
Ventricular septal defects (VSD)
-
Epidemiology: among most common congenital heart entities in early childhood, 2/3 close by early school age; larger VSDs present volume burden to the left atrium (LA) and LV and in some, the RV
-
Types (Fig. 21-2a):
FIGURE 21-2 
Ventricular septal defects. (a) Depiction of types of VSDs. (b) Parasternal short axis view of perimembraneous VSD, systolic flow noted around 10’o clock
-
Perimembranous: 60–70 %
-
Muscular: singular or multiple (10 %), in adults generally small and restrictive
-
Supracristal: (5 %) more common in Asian populations, usually small defects located beneath the aortic annulus, may lead to progressive aortic leaflet prolapse and insufficiency (right and noncoronary cusp); typically asymptomatic until aortic regurgitation (AR) is severe.
-
AV canal defect: common in Down’s syndrome, typically involves anterior mitral cleft and occasionally cleft tricuspid septal leaflet; primum ASD may coexist
-
-
Clinical presentation: varies depending on prior management
-
If small isolated restrictive defect, typically asymptomatic with a murmur
-
If well repaired earlier, typically asymptomatic. Residual VSD is usually small, heart block may occur, and residual or recurrent AR (in a supracristal VSD) or MR (in AV canal VSD)
If large defect uncorrected in childhood → Eisenmenger syndrome
-
-
ECG: typically RBBB (pre or post repair); marked left axis deviation (and sometimes AV block) with AV canal VSDs, right axis deviation/right ventricular hypertrophy (RVH) if significant pulmonary hypertension and in rare patients with progressive RV infundibular hypertrophy.
-
Physical exam:
-
Classic small restrictive VSD murmur is holosystolic, loud and harsh, augments with isometrics.
-
Associated diastolic murmur of AR if aortic cusp prolapse is present
-
In AV Canal patients, an MR or tricuspid regurgitation (TR) murmur from a cleft valve may also be appreciated
-
If prior pulmonary banding (previously done in infancy to avoid pulmonary volume overload until corrective repair could be undertaken), a loud systolic ejection murmur of supravalvular pulmonic stenosis can be appreciated, and if RVH, there may be a jugular venous a wave on exam
-
Eisenmenger exam-see below
-
-
Echocardiography:
-
Define detailed VSD anatomy (Fig. 21-2b), estimate RV pressure and gradient across the defect(s), and identify associated lesions
-
If corrected, evaluate for residual shunt and assess RV pressure and rule out associated lesions
-
-
Catheterization: performed pre-operatively for pulmonary vascular assessment, coronary screening in older patients, and define associated lesions.
-
Management:
-
Small, restrictive lesions rarely require specific management
-
ACC/AHA Class I recommendation: closure of a VSD is indicated when there is a Qp/Qs (pulmonary-to-systemic blood flow ratio) of 2.0 or more and clinical evidence of LV volume overload, OR if a patients has had a history of endocarditis [2]
-
ACC/AHA Class III recommendation: closure of a VSD is not recommended in patients with severe irreversible pulmonary hypertension [2]
-
Role for percutaneous approach is evolving for VSDs remote from the tricuspid valve (TV) and aorta
-
-
Complications:
-
Endocarditis
-
Potential right-to-left thrombotic complication avoid intracardiac RV pacer or implantable cardioverter defibrillator (ICD) wires
-
Progressive aortic cusp prolapse and insufficiency, and rarely sinus of Valsalva aneurysm or fistula (fistula will result in continuous murmur)
-
Large VSDs left untreated may lead to increased PVR from long term increased pulmonary flow, and reversal of the shunt (Eisenmenger syndrome).
-
Heart block is an occasional early or late post operative complication
-
-
-
Patent ductus arteriosus (PDA)
-
General: PDA is essential for prenatal survival. It typically closes early in infancy, with a higher incidence of PDA in premature infants and those living at high altitudes. Commonly associated with Congenital Rubella Syndrome as is branch pulmonic stenosis.
FIGURE 21-3 
Patent ductus arteriosus: modified parasternal view with laminar flow across the pulmonic valve leaflets and main PA, and PDA flow from the aorta into the LPA (red arrow)
-
Clinical Presentation: varies according to size, from asymptomatic (incidentally noted), to LA and LV volume overload or Eisenmenger syndrome when large and unrepaired
-
Physical Exam:
-
Small PDA: soft continuous infraclavicular, left sternal border or left upper back murmur, enhanced with isometrics (Fig. 21-3)
-
Moderate PDA: ventricular enlargement and a displaced point of maximal impulse on palpation
-
Large PDA: LA and LV enlargement; If pulmonary hypertension, there will be a prominent pulmonic component to the second heart sound and RV heave with cyanosis and clubbing [Eisenmenger individual: may have differential cyanosis: cyanosis of feet (clubbing of toes) and perhaps left hand with normal right hand pulse oximetry]
-
Differential for continuous murmur includes: PDA, coronary AV fistula, aortopulmonary window, pulmonary AV malformation (Peutz Jaeger syndrome) or the systolic/diastolic murmur of aortic stenosis (AS)/AR
-
-
Complications: endarteritis, left heart failure, pulmonary vascular disease if large and unrepaired; in older adults calcification, aneurysm and dissection risk which may complicate repair
-
Management:
-
ACC/AHA Class I recommendation: closure of PDA either percutaneously or surgically is indicated if there is LA and or LV enlargement, if pulmonary hypertension is present in the presence of net left-to-right shunting OR prior endarteritis. Surgical closure is most appropriate when PDA is too large for percutaneous closure device, or if PDA is aneurysmal, or there is endarteritis [2]
-
ACC/AHA Class III recommendations: closure is not indicated if pulmonary hypertension with net right-to-left shunt [2]
-
-
-
Sinus of Valsalva fistula:
-
Description: Typically arise from the right or noncoronary sinus of Valsalva and enter the right heart. May be associated with a VSD high in the basal septum; Commonly associated with connective tissue abnormality
-
Clinical presentation: new onset prominent diastolic or continuous murmur, occasionally precipitated by strenuous isometric exertion
-
Management:
-
Endocarditis and AR risks exist
-
Surgical repair; transcatheter occlusion for selected patients
-
Recurrence may occur
-
-



Obstructive Lesions
Left Ventricular Outflow Tract (LVOT) Obstruction
-
Congenital Aortic Valvular Stenosis:
-
Bicuspid Aortic Valve (BAV):
-
Epidemiology: most common congenital heart lesion, male predominance, estimated 1–2 % of population, may be familial, multiple morphologic variants, may be undiagnosed for many years
-
Can be associated with aortic coarctation, should be ruled out in Turner’s Syndrome
-
Important association with medial connective tissue abnormalities of the ascending aorta
-
Abnormalities of smooth muscle, extracellular matrix, elastin and collagen of the ascending aorta sometimes result in progressive dilation and increase dissection risk with age
-
Ascending aortic dilation does not correlate with valve stenosis severity
-
-
Clinical presentation and physical exam: varies with severity of stenosis or regurgitation
-
Asymptomatic evident by only soft systolic flow murmur and early systolic ejection sound (uncommon after age 40 years)
-
Severe LV outflow obstruction, syncope, chest pain, heart failure and endocarditis
-
Stenosis may be progressive in mid life as well as with advanced age and renal dysfunction
-
Regurgitation is less common than stenosis
-
-
Echocardiography:
-
Mean Doppler gradients correlate well with transcatheter pull back gradients
-
Important to assess ascending aortic dimensions serially (frequency of imaging varies with size of aorta at initial assessment: if <40 mm → every 2 years, if ≥40 mm → annually or more frequently if rapid change or new symptoms) even in previously operated aortic valve patients who have not had prior ascending aortic intervention. CT angiography (CTA) is preferable as aortic size approaches surgical dimensions (see below).
-
-
Intervention: transcatheter balloon dilation may be appropriate in younger adults with severe stenosis without significant AR, otherwise, surgical valvuloplasty or valve replacement per valve guidelines.
-
ACC/AHA Class I recommendation: aortic surgical intervention is indicated in a patient with a BAV and ascending aorta is 5.0 cm or more, or if there is progressive dilatation at a rate greater than 5 mm per year [2]
-
-
-
Unicuspid aortic valve: rare, may present with stenosis or regurgitation. It may be associated with ascending aortic dilation. Transcatheter balloon dilation may cause AR, therefore surgical intervention for severe obstruction or insufficiency is recommended.
-
Quadricuspid aortic valve: very rare. Presents typically late in life with AR requiring aortic valve replacement, stenosis is rare.
-
-
Discrete subaortic membrane:
-
General:
-
Congenital or acquired, (occasionally associated with primum ASD, double chamber RV, or tetralogy of Fallot [TOF])
-
Prevalence among patients with ACHD is approximately 6.5 %.
-
Membranes vary in thickness, morphology and distance below the aortic valve (Fig. 21-4), AR is common due to high velocity flow jet causing aortic valve sclerosis
FIGURE 21-4 
Subaortic membrane: (a) Transespophageal echocardiogram, membrane noted approximately 1.2 cm below the aortic valve along the anterior surface of the ventricular septum, as well as the anterior aspect of the mitral valve. Note the aortic valve leaflets appears thickened and degenerated. (b) Associated aortic insufficiency
-
Familial occurrence approaches 15 % among primary relatives (who should be screened)
-
Bacterial endocarditis occurs
-
Infrequent ascending aortic dilation
-
-
Physical exam:
-
Systolic crescendo decrescendo murmur and absence of ejection sound
-
AR murmur (more than 50 %)
-
-
Management:
-
Percutaneous balloon dilation is rarely successful
-
Surgical resection for significant obstruction or insufficiency, aortic valve should be evaluated at the time of surgery as well.
-
ACC/AHA Class I recommendation: Surgical intervention indicated with peak gradient of 50 mmHg or mean gradient of 30 mmHg by echocardiography OR for lesser gradients if progressive aortic regurgitation and LV dilation (end diastolic diameter of 50 mm or more or LV ejection fraction less than 55 %) [2] – however each case should be considered independently as significant heterogeneity exists.
-
-
-
Post operative issues:
-
Residual hypertrophic LVOT obstruction, AR, left bundle branch block (LBBB) or surgical VSD can occur
-
Membranes may recur post operatively (15 %)
-
Supravalvular Aortic Stenosis: Ascending aortic narrowing (Fig. 21-5 ) commonly associated with Williams Syndrome. Obstruction may be discrete or diffuse, may extend variably cephalad in the ascending aorta and arch. Generally spares the coronary arteries and aortic valve. Surgical revision when obstruction is significant. Differential diagnosis includes: Takayasu and rarely homozygous hypercholesterolemia with secondary lipomatous deposition in the proximal ascending aorta.
FIGURE 21-5 
Supravalvular aortic stenosis (green arrow) in a patient with William syndrome, CT angiography, red arrow depicts collateral vessels (Sidhu MS et al. MGH cardiovascular imaging 2011)
-
-
Coarctation of the aorta:
-
Definition/anatomy:
-
Typically focal narrowing in the region of the ligamentum arteriosum adjacent to the origin of the left subclavian artery (Fig. 21-6a)
FIGURE 21-6 
Coarctation of the aorta. (a) Depiction of discrete coarctation (arrow) anatomy by CT angiography, sagittal section. (b) Classical CXR with the 3 sign (red arrow) and subtle rib notching. (c) Chest CTA, axial section, demonstrating prominent collateral flow axial imaging, small proximal descending aorta (arrow). (d) 2D Echocardiogram, Doppler profile of anterograde diastolic flow in the abdominal aorta. (e) Invasive hemodynamics with catheter pullback across the coarctation site demonstrating significant drop in pressure (approximately 50 mmHg) distal to the area of coarctation (arrow)
-
May be discrete obstruction or more diffuse narrowing extending proximally towards the arch, may involve associated stenosis of the left subclavian artery
-
Distal origin of the right subclavian below the coarctation site occurs in a small percentage and masks the hypertension seen by the coronary arteries and cerebral vasculature as both arm blood pressures may be reflective of post-coarctation pressure.
-
Presence of large collaterals may reduce the gradient across the coarctation site
-
Shone’s complex: coarctation associated with left heart obstructions (subaortic stenosis, BAV, parachute MV, or supramitral ring)
-
-
General:
-
Male predominance
-
Associated with BAV (50–60 %)
-
Associated circle of Willis aneurysm (ACC/AHA Class I recommendation: Intracranial vessels should be screened with MR or CT in all patients with coarctation [2])
-
-
Physical exam:
-
Pulse and blood pressure evaluation in all four extremities
-
BAV findings (when present): systolic ejection sound, precordial outflow murmur, AR murmur
-
Coarctation findings:
-
Systolic bruit over the upper left back
-
Radial-femoral delay
-
-
-
CXR findings:
-
Aortic indentation at the coarctation site “3 sign” (Fig. 21-6b)
-
Notching on the underside of the ribs from collateral vessels
-
-
Echocardiography:
-
Indications for surgical or percutaneous intervention:
-
ACC/AHA Class I recommendation: peak to peak catheterization gradient of 20 mmHg or greater (Fig. 21-6e) regardless or presence or absence of hypertension OR lesser gradient in the presence of imaging evidence of significant coarctation with significant collateral flow [2]
-
Percutaneous approach may be considered in experienced hands if narrowed site is amenable
-
Surgical intervention for complex anatomy, long segment tubular lesions, prior aneurysm, calcification or poorly compliant arterial system.
-
Advanced imaging, whether MRI or CT, may add to delineation and management
-
-
Long term follow up:
-
Lifelong adult congenital cardiology follow up is advised with interval assessment for development of resting or exercise-induced hypertension
-
Repair or re-repair is appropriate regardless of advanced age
-
For complex coarctation, bypass grafting from left subclavian artery to descending aorta or ascending to descending aorta is often advisable.
-
ACC/AHA Class I recommendation: evaluation of coarctation repair site by MRI/CT should be performed at intervals of 5 years or less (depending on anatomy of repair) to assess for coarctation site aneurysm or residual obstruction [2]
-
-
Pregnancy:
-
With unrepaired or postoperative recurrent coarctation, as well as with aneurysms, there is an increased risk of 3rd trimester or peripartum dissection, which may be fatal
-
Hypertension and pre-eclampsia may also occur in select individuals
-
Pre-pregnancy counseling is critical, maternal and fetal risks can exist and vary based on prior repair and anatomy
-
Pre-pregnancy coarctation imaging is essential to inform risk discussion
-
Genetic transmission should be discussed and fetal echocardiography is recommended
-
-



Right Ventricular Outflow Tract (RVOT) Obstruction/Pulmonic Stenosis (PS)
-
Valvular PS : Congenital PS most often occurs at valve level, whether bi or tricommissural. Varies significantly in severity and clinical presentation.
-
Noonan syndrome may be associated with myxomatous valvular PS (may also have associated LV hypertrophic cardiomyopathy)
-
Physical exam:
-
Systolic ejection murmur (intensity, time to peak and duration, vary with severity)
-
Presence of early systolic ejection sound; closer the ejection sound to S1, the more severe stenosis—of note the pulmonic valve ejection click is the only right heart finding which decreases in intensity with inspiration
-
Pulmonic closure intensity decreases and delay of P2 from A2 increases with severity of stenosis.
-
Jugular venous a waves and RVH are present in significant stenosis
-
Low pitched diastolic murmur of PR may coexist
-
-
Echocardiography: defines and quantifies PS anatomy and severity
-
CXR:
-
Prominent main and left pulmonary branch dilation (even if stenosis is not severe)
-
-
Management:
-
Surgically managed since the mid 1950s with excellent survival
-
Since early 1980s, transcatheter balloon dilation has supplanted surgery for a majority
-
Balloon valvotomy- ACC/AHA Class I recommendations [2]:
-
If asymptomatic with favorable valve anatomy: peak instantaneous Doppler gradient is 60 mmHg or greater, or mean Doppler gradient of 40 mmHg or greater
-
If symptomatic: peak instantaneous gradient of 50 mmHg and mean of 30 mmHg
-
Moderate or greater PR is a relative contraindication.
-
-
-
-
Supravalvular PS : (or Branch PS) is uncommon but noteworthy and occurs in Congenital Rubella syndrome, Williams syndrome and Takayasu arteritis. Balloon dilation is favored if the lesion in amenable. May occur iatrogenically in the branches from previous systemic to pulmonary palliative shunts, or at the main PA from prior pulmonary artery banding.
-
Subpulmonic stenosis : rare but does occur in patients with valvular PS, tetralogy of Fallot and some transposition patients.
-
Double chambered RV : Anomalous muscle bundles that divide the RV into a higher pressure proximal chamber and a lower pressure distal chamber. Associated lesions are VSD, valvular PS, subaortic membranes. In the elderly, double chambered RV may be complicated by ventricular tachyarrhythmia.
Complex Lesions
-
Tetralogy of Fallot (TOF):
-
General:
-
Most common cyanotic congenital heart lesion after infancy
-
Spectrum of morphology and severity, with pulmonary atresia and VSD the most severe form
-
-
Anatomy: RV outflow obstruction (valvular and subvalvular/infundibular with generally small pulmonary arteries), large VSD with an overriding aorta and RV hypertrophy (Fig. 21-7a). Right aortic arch is associated in 25 % of cases. Suspect TOF as a diagnosis in cyanotic patients with a right aortic arch.
FIGURE 21-7 

Tetralogy of Fallot. (a) Depiction of TOF. (b) Classical ECG with RBBB, right ventricular hypertrophy (patient status post PVR for severe PR). (c) Palliative shunts. (d) 2D echocardiogram of continuous wave Doppler profile across the RVOT consistent with severe pulmonic regurgitation. Note: steep deceleration of pulmonic regurgitant jet, correlates with short decrescendo diastolic murmur
-
∼ 5 % of TOF patients have aberrant course of the left anterior descending (LAD) or left main arising from the proximal right coronary artery (RCA) or right sinus of Valsalva, traversing the RVOT (coronary anatomy should be assessed pre-operatively)
-
Approximately 15 % patients have ascending aortic dilation, most notably those with AR, right aortic arch, and severe degrees of pulmonary stenosis, particularly pulmonary atresia
-
-
Clinical presentation in adults:
-
Patients present s/p remote palliative procedures (see below), but most present s/p remote complete repair. It is rare to present as an adult with no prior interventions, though teenagers in immigrant populations may present with native disease.
-
Post complete repair: asymptomatic or may have significant late complications including significant pulmonary insufficiency and RV dilation and dysfunction, and ventricular tachycardia (VT), sudden cardiac death.
-
-
Physical exam:
-
Evidence of residual RVOT obstruction with systolic murmur over the pulmonic area
-
Harsh holosystolic murmur of a residual VSD
-
Pulmonary incompetence: low-pitched diastolic decrescendo murmur; shorter murmurs generally more severe
-
-
ECG:
-
RBBB, RVH, RA enlargement (Fig. 21-7b)
-
T wave inversions over anterior precordium
-
PR prolongation and complete heart block rarely
-
SVT or VT
-
-
Palliative interventions (Fig. 21-7c and Table 21-1): do not correct the pulmonary stenosis or the right-to-left shunt
Table 21-1 Surgical palliation or corrective procedures -
Blalock-Taussig shunt is most common. Waterston and Potts are rarely used today.
-
Blalock-Taussig shunt (subclavian artery to branch PA): allowed survival to complete repair; ligated at time of complete repair
-
Potts shunt (descending aorta to left PA window): may be complicated by pulmonary vascular obstruction of the left lung or left PA hypoplasia (challenging surgical revision)
-
Waterston shunt (ascending aorta to right PA window): complications include right PA stenosis and hypoplasia. Transcatheter right PA dilation may be helpful
-
-
Rastelli procedure: (See Table 21-1, Figure 21-18) used in patients who have degrees of transposition of the great arteries associated with their VSD and pulmonary stenosis where traditional complete TOF repair is not possible
-
Baffle from the LV to the ascending aorta (occasionally complicated by AV block) and valved conduit placement from the RV to the main PA
-
Late stenosis of the RV to PA conduit is common and requires with either percutaneous dilation or surgical replacement. Experience with percutaneous valve placement in the Rastelli conduit is growing at select institutions.
-
Stenosis occurs at the take off or touch down conduit site or at the level of the valve within the conduit (transcatheter techniques for pulmonary valve dilation or replacement are rapidly evolving)
-
-
Complete repair (VSD closure, RVOT augmentation): now mostly performed in infancy or early childhood
-
Late post repair complications:
-
PR may be progressive over several decades (Fig. 21-7d). ACC/AHA Class I recommendation: Pulmonic valve replacement is indicated for severe PR with any of the following: (1) symptoms of decreased exercise tolerance, (2) moderate to severe RV dysfunction or enlargement (3) sustained atrial or ventricular arrhythmias or (4) moderate to severe TR [2]
-
Significant residual VSD is increasingly less common as is significant residual PS.
-
SVT is increasingly common beyond the fifth decade
-
Ventricular tachycardia (VT) /fibrillation (sudden cardiac death):
-
High risk features: LV dysfunction, palliation for many years prior to complete repair/older age at time of repair, significant RV dilation and dysfunction, high RV mass to volume ratio, inducible VT on electrophysiology testing, and QRS duration >180ms
-
Aggressive antiarrhythmic management and assessment and implantable defibrillator should be considered in high risk patients. It is important to address repair of significant hemodynamic lesions in patients with an arrhythmia burden as well.
-
-
-
Pregnancy:
-
Well repaired stable TOF adults manage well through pregnancy and delivery, but always advisable to involve high risk obstetrics and congenital heart specialist
-
Risk of right heart failure and arrhythmia is increased with significant RV dysfunction
-
-
-
Ebstein Anomaly
-
General: approximately 1 % of all CHD, wide spectrum of severity of anatomic and functional abnormalities of the TV and RV
-
Anatomy: “Apical displacement” of the TV caused by failure of delamination of the tricuspid leaflets from the RV muscle, compromise in size of the portion of the RV below the TV and enlargement of the RA by portion of the RV above the TV (‘atrialized’ RV)
-
Major clinical issues:
-
Degree of tricuspid regurgitation
-
RV cardiomyopathy/ RV function
-
Presence of an associated interatrial communication (ASD or stretched patent foramen ovale [PFO])
-
Atrial arrhythmias
-
-
Clinical presentation is highly variable:
-
From asymptomatic with a nearly silent clinical exam to marked right heart failure, cyanosis, and early death
-
Wolff-Parkinson-White syndrome (WPW) is present in 25 % of patients and presents with palpitations or SVT. Ventricular arrhythmias may occur.
-
Progressive exercise intolerance and fatigue from TR and RV dysfunction may occur
-
Acute systemic desaturation from right-to-left shunt through an ASD or PFO is poorly tolerated. Paradoxical embolus can rarely occur.
-
-
Clinical exam
-
Tricuspid holosystolic murmur and multiple systolic clicks exist but can be subtle
-
Both first and second heart sounds are widely split
-
“Sail sound” of a loud systolic sound created by the large anterior leaflet may be heard
-
Rocking motion of the heart with an easily palpable RV in more severe disease
-
Right heart failure: elevated jugular venous pressure, hepatojugular reflux, lower extremity edema, hepatic congestion, cyanosis
-
-
ECG: wide and splintered QRS complex (right precordial leads), RA enlargement, first degree AV block and when present, Type B WPW pattern (Fig. 21-8a)
FIGURE 21-8 
Ebstein’s anomaly. (a) ECG with right axis deviation, first degree AV block and complete right bundle branch block with marked splintering of the R’ deflection. (b) CXR of marked cardiomegaly. (c) 2D echocardiogram, four chamber view demonstrating marked apical displacement of the septal leaflet of the tricuspid valve, large atrialized portion of the RV
-
CXR: varies with severity and shows RA enlargement, pulmonary vasculature usually normal unless marked cyanosis, and cardiac silhouette can be massive with enlargement progressing with age (Fig. 21-8b).
-
Echocardiography is the diagnostic gold standard and defines anatomy and severity of TR, RV size and function, RA size, interatrial communication and associated LV abnormalities (Fig. 21-8c).
-
Management:
-
IV filters when ASD or PFO present
-
SVT and accessory pathway management can be challenging secondary to multiple bypass tracts, variation in atrialized RV and tricuspid annular anatomy, thickened atrialized RA tissue and thin RV walls.
-
Anticoagulation is recommended if history of paradoxical embolism or atrial fibrillation
-
-
Surgical timing: cannot be generalized and differs with each individual
-
Surgery is best performed in experienced centers
-
Options include TV repair vs. replacement, inter-atrial communication closure, simultaneous Maze procedure, and in some, cardiac transplant
-
Post operatively: management includes avoidance of right ventricular afterload and positive pressure, and arrhythmia and AV block surveillance.
-
-
Pregnancy: pre-pregnancy counseling is important; successful delivery is often accomplished without difficulty in uncomplicated patients; but with significant RV failure, TR, and cyanosis, pregnancy should be discouraged.
-
-
Transposition of the Great Arteries (TGA)
-
D-TGA:
-
Anatomy: great vessels arise from the incorrect ventricle (i.e., ventriculoarterial discordance: aorta arises from the morphologic RV and PA arises from the morphologic LV) resulting in parallel circulations (Fig. 21-9a)
FIGURE 21-9 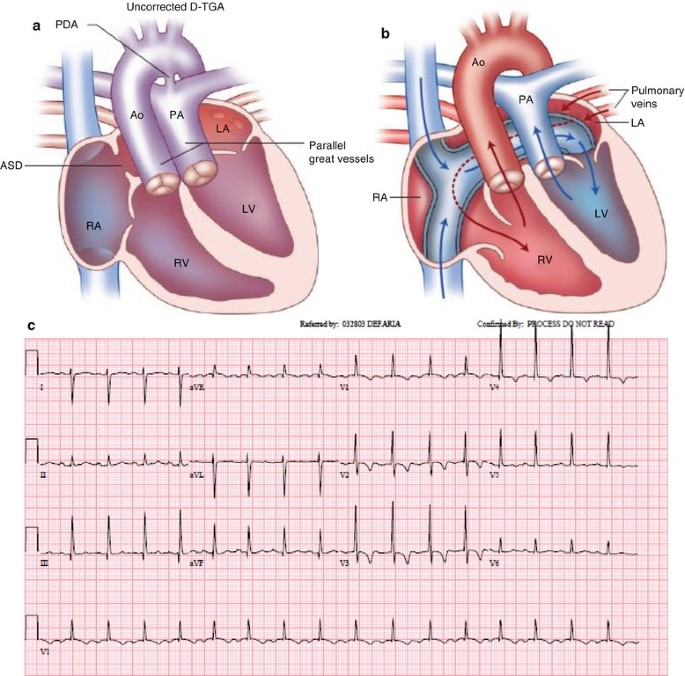

D Transposition of the Great Arteries. (a) Depiction of D TGA anatomy. (b) Schematic of Mustard anatomy with baffle directing SVC and IVC flow across the intraatrial septum to the morphologic right ventricle. (c) ECG of patient status post Mustard atrial switch with RVH and right axis deviation. (d) CTA and MRI of patient with D TGA demonstrating intraatrial baffle directing flow from the pulmonary veins to the LA across the tricuspid valve to hypertrophied systemic RV. (e) Schematic of Jatene arterial switch procedure
-
General: most common cause of cyanotic CHD in neonates
-
Surgery: adults with D-TGA have had some form of intervention in infancy including:
-
Rashkind balloon atrial septostomy to allow sufficient mixing of deoxygenated and oxygenated blood and enable survival for the early post delivery months
-
Blalock Hanlon surgical atrial septectomy
-
Atrial switch: Senning and Mustard procedures (until 1980s) – (Fig. 21-9b):
-
re-routes systemic venous return to the MV and LV and lungs, and allows pulmonary venous flow to the TV and RV and aorta.
-
Clinical exam:
-
RVH with loud (single sounding) second heart sound from the anteriorly placed aorta, often no murmur
-
outflow murmur if there is associated sub pulmonic stenosis
-
holosystolic murmur if there is (systemic) TV regurgitation
-
-
ECG: marked right axis deviation and RVH (Fig. 21-9c)
-
Echocardiography: defines the status of the atrial baffle (rule out baffle leak or obstruction), rule out AV valvular regurgitation, presence of subpulmonic obstruction, and evaluate biventricular dysfunction.
-
CT/MRI: useful in diagnosing baffle leak or obstruction, and assessing ventricular volumes and function (Fig. 21-9d)
-
Long term complications:
-
Sinus node dysfunction, sudden death, atrial arrhythmias, ventricular arrhythmias
-
Atrial baffle leak allowing an atrial level shunt
-
Atrial baffle obstruction resulting in inhibition of systemic or pulmonary venous return
-
Systemic atrioventricular valve regurgitation and systemic RV dysfunction
-
-
Management:
-
Medications/ablation for atrial arrhythmias, pacemaker for significant sinus node dysfunction
-
Percutaneous intervention for both baffle leaks and obstruction
-
Systemic right ventricle failure with progressive TR should be managed with aggressive systemic afterload reduction but may require cardiac transplantation
-
-
-
Arterial switch: Jatene Procedure (Fig. 21-9e)
-
Has largely supplanted the atrial switch procedure since the 1980s
-
Normal exam (healed incision) and generally normal ECG
-
Potential complications:
-
Aortic dilation and AR
-
Supra- aortic and supra- pulmonic anastomotic site stenosis
-
Coronary ostial obstruction (rare)
-
-
-
-
-
Congenitally corrected Transposition of the Great Arteries (CC-TGA, L-TGA, ventricular inversion):
-
Anatomy: systemic venous flow (vena cavae) enter the RA, traverse a MV to a subpulmonary LV and exit the PA to the lungs. The pulmonary veins enter the LA and traverse the TV to the RV to the aorta (making the TV the “systemic” ventricle).
-
Associated anomalies include VSD, pulmonic stenosis, or systemic AV valve (tricuspid) insufficiency (occasionally Ebstein-like valve) and complete heart block.
-
Clinical exam:
-
Consider L-TGA in any young adult with unexplained heart block
-
Loud second heart sound (from the anteriorly placed aorta)
-
Systemic AV valve insufficiency murmur (if tricuspid valve is abnormal or RV annulus is dilated)
-
If VSD and PS are present, there may be cyanosis and clubbing
-
-
ECG: (Fig. 21-10a)
-
Classic ECG is diagnostic: Q wave in right precordial leads (septal depolarization direction is altered) with varying degrees of heart block
-
-
CXR: (Fig. 21-10b)
-
Flat or convex upper left-sided cardiac silhouette, reflecting the abnormal ascending aorta position and take off
-
-
Echocardiogram: (Fig. 21-10c)
-
Gold standard for diagnosis and detection of associated lesions.
-
Apically placed TV which enters the RV receives LA inflow and communicates with the aorta. Apical 4 chamber best demonstrates the “inverted ventricles”.
-
-
Outcomes:
-
May survive well into older age with essentially normal lifestyle including pregnancy and delivery.
-
Complete heart block may require pacemaker placement (active fixation leads may be needed for the smooth LV septal surface).
-
Can present with progressive systemic (tricuspid) AV valve regurgitation and progressive systemic RV dilation, dysfunction and failure
-
-
Management:
-
Afterload reduction and maintaining lower blood pressure is helpful
-
Pacemakers for complete heart block, small studies reveal cardiac resynchronization may have a role in some patients with systemic RV failure.
-
TV replacement (less often repair) for significant TR if systemic ventricular function is not severely compromised may help preserve systemic ventricular function.
-
Clinical management of L-TGA patients can be challenging and expert ACHD input is strongly recommended.
-
Cardiac transplantation may be needed for medically refractory heart failure
-
-
-
-
Univentricular Heart and Fontan revision (Fig. 21-10)
FIGURE 21-10 
L Transposition of the Great Arteries. (a) ECG with first degree AV block, Q waves in II, III, F, absence of septal Q waves in V5-V6 due to inversion of the right and left bundle branches causing septal activation to occur from right to left axis deviation and PVC not necessarily seen in L-TGA. (b) CXR of patient with L- TGA and dual chamber pacer. (c) 4-chamber view demonstrating apical displacement of the systemic AV valve indicating this is a tricuspid valve and systemic right ventricle, pacer lead also noted in the morphologic (subpulmonary) LV
(Tricuspid or Mitral atresia, hypoplastic left or right heart syndrome)
-
Early Interventions include:
-
Pulmonary artery banding: protect the lungs from overcirculation for patients with no natural pulmonary flow obstruction
-
Modified Blalock-Taussig shunt (subclavian artery to PA prosthetic conduit): often used for infants with severe pulmonic stenosis or pulmonary atresia and cyanosis, and staged prior to the Fontan procedure
-
Glenn procedure: direct connection of SVC to right PA (may cause late right pulmonary arteriovenous malformations - secondary to absence of inferior venous cava flow to the right lung which may carry “liver factors” which prevent pulmonary arteriovenous malformation)
-
-
Fontan procedure: allows systemic venous flow to be directed to the lungs without the aid of a ventricular pump (Fig. 21-11).
FIGURE 21-11 
Fontan circulation
-
Complications:
-
RA to PA Fontan: RA enlargement, thrombus formation, atrial arrhythmias, hepatic congestion and eventual cirrhosis
-
Lateral tunnel Fontan: Atrial arrhythmias, hepatic congestion
-
Extracardiac conduit: Hepatic congestion may still occur
-
Fistulous communications from the systemic to the pulmonary circulation may present as new onset progressive desaturation, often amenable to transcatheter occlusion
-
-
-
Univentricular dysfunction as well as AV incompetence may be progressive in adult life, hence early and continued management with afterload reduction and avoidance of systemic hypertension is an essential feature for these patients.
-
When Fontan patients require intubation avoidance of positive pressure is essential
-
-
Pregnancy: can be very challenging, contraindicated in severe cyanosis, may not do well with depressed single ventricle ejection fraction
-
-
Eisenmenger Syndrome
-
General: seen in patients with large left-to-right shunt lesions who were not appropriately intervened upon in childhood (generally because of limited access to health care); defined as progressive increase in PVR which leads to reversal of shunting (right-to-left) and ultimately subpulmonary ventricular failure and death; overall, increasingly uncommon
-
Clinical Exam:
-
Cyanosis, clubbing, jugular venous a wave
-
Prominent RV heave, loud P2
-
Often no murmur, but occasionally the holosystolic murmur of TR or diastolic murmur of functional PR from elevated PVR
-
Hepatosplenomegaly from chronic congestion
-
-
CXR: Large main PA and central PA with oligemic periphery (pruning) (Fig. 21-12a, b)
FIGURE 21-12 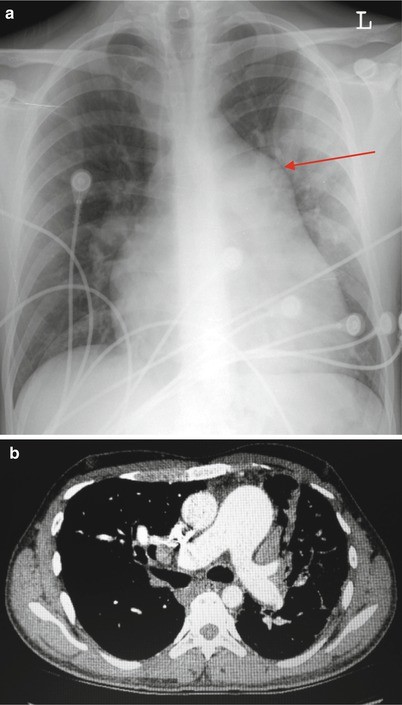
Eisenmenger physiology. (a) CXR of patient with Eisenmenger with markedly enlarged pulmonary artery (arrow). (b) Chest CT angiography demonstrating PA is significantly larger than aorta, PA branches are dilated
-
Complications:
-
Systemic emboli or abscess from right-to-left shunting
-
Erythrocytosis as a response to chronic hypoxemia, thrombocytopenia from splenic sequestration; neurologic events may occur due to hyperviscosity syndrome
-
Hemoptysis may occur
-
Arrhythmia and sudden cardiac death
Management: Medical therapy with pulmonary arterial vasodilators is an option and may prolong survival [4] and the only surgical option is heart-lung transplant. ACC/AHA Class I recommendations:
-
Avoidance of dehydration, moderate to severe strenuous activity, isometric exercise, excessive heat, chronic high altitude exposure and iron deficiency [2]
-
Annual monitoring of hemoglobin, platelet count, iron stores, creatinine, and uric acid annually; assess oximetry with and without oxygen annually [2]
-
Right-to-left shunt precautions are essential with all IVs [2]
Other recommendations: Endocarditis prophylaxis, phlebotomy when appropriate (neurologic symptoms from hyperviscocity), anticoagulation may be considered, avoidance of unessential surgery or anesthesia is important. With appropriate and experienced clinically guided care, Eisenmenger patients can survive to midlife and on occasion beyond
-
-
Pregnancy: strictly contraindicated
-
-
Dextrocardia and cardiac malposition
-
Mirror Image Dextrocardia: (Fig. 21-13a)
FIGURE 21-13 
Dextrocardia. (a) CXR of patient with mirror image dextrocardia (stomach bubble is on the patient’s right). (b) ECG with normal ECG lead placement and mirror image dextrocardia demonstrating inverted precordial R wave progression with negative P wave and right axis deviation in lead 1. Differential diagnosis for negative p wave in lead 1 includes: right/left arm reversal or mirror image dextrocardia
-
Total situs inversus: heart chambers and body viscera are all in mirror image position
-
Many have no associated congenital cardiac anomaly
-
ECG, Echo, CXR: when present, can trigger identification (Fig. 21-13b)
-
-
Kartagener’s syndrome:
-
Bronchiectasis, sinusitis, ciliary dysmotility, infertility
-
Limited to those with mirror image dextrocardia and not seen in dextroversion (heart is dextrorotated but visceral abdominal organs are in normal position)
-
-
-
Congenital Coronary anomalies
-
ALCAPA: anomalous left coronary artery origin from the PA (rare)
-
In the absence of surgical intervention, most infants die in early infancy. Rare natural survivors may have acute myocardial infarction (MI), MR and LV failure and survive to childhood.
-
Management in Infancy involves:
-
Creation of a tunnel in the posterior PA to redirect the anomalously arising left coronary artery blood flow to a neo left coronary ostium and the left coronary artery.
-
Long term results of this procedures are still evolving but are encouraging with near normal LV function.
-
Even in patients who had significant LV damage with their presentation as infants, LV recovery often seems very favorable.
-
Exercise treadmill testing with imaging, arrhythmic monitoring and in many beta blockade or angiotensin converting enzyme (ACE) inhibition for less than normal LV function is likely prudent.
-
-
Adult presentation:
-
Infants can grow to adulthood with minimal complications and no significant heart failure post repair
-
Approximately 5 % of ALCAPA patients are unrepaired and survive by natural intercoronary collateral flow and may present in adult life with a palpable left ventricular aneurysm, MR, ventricular tachyarrhythmia and a continuous flow bruit over the anterior wall from the right to the left coronary circulation
-
ECG: may demonstrate LV aneurysm or remote anterior myocardial infarction pattern (Q waves and ST changes with loss of R waves in the anterior precordial leads).
-
-
-
Ectopic origin of the coronary artery:
-
Either the left or right coronary artery may arise from the contralateral sinus of Valsalva and pass anteriorly to the aorta and posterior to the RV outflow tract. Other coronary anomalies include a single coronary orifice, an aberrant LAD (in TOF arising from the RCA) or aberrant left circumflex (usually from the right, retroaortic, and therefore benign) (Fig. 21-14a, b)
FIGURE 21-14 
Ectopic coronary arteries. (a) Anomalous left anterior descending arising from the right coronary cusp traversing between the aorta and the RVOT. (b) Anomalous right coronary artery arising from the left coronary cusp (arrow) with anterior course, note all coronaries originate off the left coronary cusp. (c) Angiography of congenital coronary AV fistula from left main to pulmonary artery, often times small and tortuous and rarely need intervention
-
Presentation of anomalous coronary from contralateral cusp:
-
Incidental finding during scan for alternate indication
-
Sudden cardiac death
-
Ventricular arrhythmia
-
Exertional chest symptoms or syncope
-
-
Diagnosis:
-
Targeted ultrasound of coronary artery origins can be diagnostic (parasternal short axis above the level of the aortic valve)
-
MRI and CTA can be confirmatory (define the course of the vessel, assess for dominance of the artery and caliber of the proximal lumen and of the ostium. CT can assess for atherosclerosis which can change a previously benign clinical presentation)
-
-
High risk features:
-
Age at presentation < 50 years
-
Proximal hypoplasia and stenosis of the ectopic artery, or proximal oblique (or ‘slit-like’) orifice
-
Interarterial course: anterior to the aorta and posterior to the RVOT alone may not be the strongest risk factor, however the presence of a dominant ectopic vessel with proximal anatomic or functional obstruction suggests high risk and surgical intervention should be considered. Individuals with an interarterial course alone and age >50 years have anecdotally survived well with no intervention.
-
Presentation with ventricular arrhythmia in adolescence or young adulthood especially with exertion.
-
Presence of detectable ischemia on stress testing in the distribution perfused by the ectopic artery
-
-
Management:
-
Without high risk features: beta blockade (data are limited) and lifestyle modification
-
With high risk features: beta blockade and consider surgical revascularization
-
Anomalous coronary artery assessment and management can be challenging and expert ACHD consultation (with multidisciplinary evaluation) is often prudent.
-
ACC/AHA Class I recommendations (Level of Evidence B): surgical revascularization if:
-
anomalous left main courses between the aorta and PA/RVOT
-
documented ischemia due to coronary compression
-
anomalous origin of the right coronary between the aorta and PA/RVOT with evidence of ischemia [2]
-
-
-
-
Congenital coronary AV fistula:
-
Clinical exam: (in larger congenital coronary AV fistula)
-
Precordial continuous murmur (see differential above under PDA, physical exam)
-
-
Presentation:
-
Subclinical, incidental findings by ultrasound or at the time of coronary angiography (particularly small left main to PA congenital coronary AV fistula – Fig. 21-14c)
-
Heart failure, cardiomegaly (when large, usually from RCA or left circumflex, entering right heart)
-
Thrombosis
-
Ischemia secondary to steal phenomenon, where the fistula redirects flow away from the coronary distal to the fistula takeoff
-
-
Management:
-
Observation for small fistulas
-
If amenable, transcatheter coils are the treatment of choice
-
Surgical approach is also an option in select cases, and preferable with large aneurysms.
-
-
-










Review Questions
-
1.
A 31 year old man with a history of testicular cancer, received a chest, abdomen, and pelvic CT which revealed right ventricular and pulmonary arterial enlargement. An echocardiogram was recommended, but was read as only right heart enlargement. Images are below (Fig. 21-15). What anomaly can be seen in association with this diagnosis?
FIGURE 21-15 
Question 1 (Echo and CT)
-
(a)
tetralogy of Fallot
-
(b)
ciliary dysmotility syndrome
-
(c)
partial anomalous pulmonary venous connection
-
(d)
absent radius
-
(a)
-
2.
A 26 year old woman presents with hypertension and lower extremity claudication. Echocardiogram and CT (Fig. 21-16a, b). Which of the following statements are true?
FIGURE 21-16 
Question 2 (Echo)
-
(a)
This lesion is associated with bicuspid aortic valve in 60 % of cases
-
(b)
There is a high risk for mother and fetus if a gradient >30 mmHg is present
-
(c)
She should be offered a brain MRI or CT to evaluate for Berry aneurysm
-
(d)
Surgical and percutaneous approach have both been validated in this lesion
-
(e)
All of the above
-
(a)
-
3.
A young man from Cape Verde with right aortic arch, infundibular and valvar pulmonic stenosis presented for surgical correction. Post operatively, after infundibular resection and PVR, he developed florid heart failure. Which of the following was the most likely etiology?
-
(a)
peri-operative myocardial infarction
-
(b)
sudden pulmonary embolism
-
(c)
left to right shunt through an associated VSD once RV pressure declined
-
(d)
over-aggressive fluid resuscitation intra-operatively
-
(a)
-
4.
A 21 year old woman presents to you to establish primary care. She states she has a history of D transposition of the great vessels and had a surgical procedure when she was a young child. She currently denies any symptoms. Her exam is notable for normal vital signs, a median sternotomy scar, jugular venous pressure of 5cmH20, normal S1 with prominent A2 and no murmurs or heaves, liver is normal in size without pulsatility and she has no peripheral edema. Her ECG is below (Fig. 21-17). Which of the following below statements are true.
FIGURE 21-17 
Question 4
FIGURE 21-18 
Depiction of Rastelli procedure (RV to PA conduit)
-
(a)
Her systemic ventricle is her morphologic right ventricle
-
(b)
She is at high risk for atrial arrhythmias
-
(c)
A potential complication of her surgery is ostial coronary stenosis and aortic regurgitation
-
(d)
Her PA diameter should be intermittently monitored with serial echos to screen for dilation
-
(e)
She may have significant tricuspid regurgitation that cannot be heard on exam due to abnormal cardiac anatomy
-
(a)




Answers
-
1.
(c) Sinus venosus septal defect, pictured above, is commonly seen in association with anomalous pulmonary venous return. In cases of right heart enlargement where a secundum ASD is not readily visualized, TEE and MRI can be used to assess for sinus venosus or coronary sinus septal defects, as well as anomalous pulmonary venous return. Remember that while atrial level shunts cause right heart enlargement, large VSDs are more likely to cause left heart enlargement with some effect on the RV size, and PDA will create only left heart enlargement. Surgical correction of SV septal defect with PAPVR can be performed with a patch repair or a Warden procedure, where the SVC is transected cranial to the anomalous vein entrance and reattached to the RA appendage, while the SVC stump serves as a reservoir for the pulmonary vein which is directed into the left atrium via the sinus venosus defect. Superior sinus venosus with right upper pulmonary vein anomaly is more common than inferior sinus venosus defects or return of pulmonary venous drainage to the IVC (known as Scimitar Syndrome when accompanied by additional findings).
-
2.
(e) Coarctation of the aorta should always be in the differential diagnosis of hypertension in the young individual. Symptoms may include headaches from hypertension, claudication, fatigue. The diagnosis may also be incidental in the setting of evaluation for a BAV click or murmur. On physical exam, with a significant coarctation, there will be a radial-femoral (or brachial femoral) pulse delay which is palpable. Intervention is recommended at a peak to peak gradient of 20 mmHg. At 30 mmHg for any LV outflow lesion, the risk in pregnancy rises significantly. Patients should be informed of the risks of long term hypertension even with excellent and lasting repair, premature coronary artery disease, presence of an intracerebral aneurysm, and risk of recoarctation or aortic dilation. Intervention can be surgical (most commonly end to end anastomosis; however some individuals may have had a left subclavian flap repair, and therefore will have a poor pulse and blood pressure in that arm). Guidelines recommend imaging of the aorta with CT/MRI once every 5 years.
-
3.
(c) The presence of RVOT obstruction and right arch should raise suspicion for TOF, as 25 % of TOF patients will have right aortic arch. TOF consists of overriding aorta, VSD, RVH, and RVOT obstruction. The VSD, both in TOF and as an isolated lesion, can be unrecognized due to overlying tricuspid apparatus which can effectively “close” the defect. In this case, with relief of RVOT obstruction and placement of a pulmonic valve prosthesis, the RV pressure dropped and acute left to right shunting across the VSD ensued as the LV to RV pressure differential overpowered the thin septal leaflet which was covering the VSD. This acute shunt development can result in clinical heart failure.
-
4.
(c) D TGA occurs with atrioventricular concordance (blood flows from RA through TV to RV) and ventriculoarterial discordance (RV to aorta), similarly LA through MV to LV to the PA. Options for correction in infants and children include atrial switch procedures (Mustard or Senning) where systemic venous flow is baffled through the intra-atrial septum to the morphologic LV out the PA. Complications of atrial switch procedures include atrial arrhythmias, baffle leaks, and systemic RV dysfunction. The arterial switch operation (or Jatene procedure) requires aortic and PA root excision and reimplantation to the appropriate ventricular chamber, and coronary buttons are reimplanted to the neo aortic root. Patients who have undergone arterial switch operations have nearly normal exam and ECG, and potential long term complications include aortic regurgitation or issues with ostial coronary stenosis (Table 21-2).
Table 21-2 Syndromes associated with congenital heart disease
Abbreviations
- ACE:
-
Angiotensin converting enzyme
- ADHD:
-
Adult Congenital Heart Disease
- ALCAPA:
-
Anomalous left coronary artery origin from the PA
- AR:
-
Aortic regurgitation
- AS:
-
Aortic stenosis
- ASD:
-
Atrial septal defect
- AV:
-
Atrioventricular
- BAV:
-
Bicuspid Aortic Valve
- BP:
-
Blood pressure
- CC-TGA:
-
Congenitally corrected Transposition of the Great Arteries
- CHD:
-
Congenital heart disease
- CTA:
-
CT angiography
- CXR:
-
Chest X Ray
- EF:
-
Ejection fraction
- ICD:
-
Implantable cardioverter defibrillator
- LA:
-
Left atrium
- LAD:
-
Left anterior descending
- LBBB:
-
Left bundle branch block
- LV:
-
Left ventricular
- LVOT:
-
Left ventricular outflow tract
- MI:
-
Myocardial infarction
- MR:
-
Mitral regurgitation
- MV:
-
Mitral valve
- NO:
-
Nitric oxide
- PA:
-
Pulmonary artery
- PDA:
-
Patent ductus arteriosus
- PFO:
-
Patent foramen ovale
- PR:
-
Pulmonic regurgitation
- PS:
-
Pulmonic stenosis
- PVR:
-
Pulmonary vascular resistance
- RA:
-
Right atrium
- RBBB:
-
Right bundle branch block
- RCA:
-
Right coronary artery
- RV:
-
Right ventricle
- RVH:
-
Right ventricular hypertertrophy
- RVOT:
-
Right ventricular outflow tract
- SVC:
-
Superior vena cava
- SVT:
-
Supraventricular tachycardia
- TEE:
-
Transesophageal echocardiogram
- TGA:
-
Transposition of the Great Arteries
- TOF:
-
Tetralogy of Fallot
- TR:
-
Tricuspid regurgitation
- TV:
-
Tricuspid valve
- VSD:
-
Ventricular septal defect
- VT:
-
Ventricular tachycardia
- WPW:
-
Wolff-Parkinson-White syndrome
References
Liberthson RR. Congenital heart disease: diagnosis and management in children and adults. Boston: Little, Brown; 1989.
Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM, Dearani JA, et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease. Circulation. 2008;118:e714–833.
Du ZD, Hijazi ZM, Kleinman CS, Silverman NH, Larntz K. Comparison between transcatheter and surgical closure of secundum atrial septal defect in children and adults: results of a multicenter nonrandomized trial. J Am Coll Cardiol. 2002;39:1836–44.
Dimopoulos K, Inuzuka R, Goletto S, Giannakoulas G, Swan L, Wort SJ, et al. Improved survival among patients with Eisenmenger syndrome receiving advanced therapy for pulmonary arterial hypertension. Circulation. 2010;121(1):20.
Suggested Readings
Rhodes JF, Hijazi ZM, Sommer RJ. Obstructive lesions pathophysiology of congenital heart disease in the adult. Part II: simple. Circulation. 2008;117:1228–37.
Sommer RJ, Hijazi ZM, Rhodes Jr JF. Pathophysiology of congenital heart disease in the adult: part I: shunt lesions. Circulation. 2008a;117:1090–9.
Sommer RJ, Hijazi ZM, Rhodes JF. Pathophysiology of congenital heart disease in the adult: part III: complex. Circulation. 2008b;117:1228–37.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
Yeh, D.D., Liberthson, R.R., Liberthson, R.R., Bhatt, A.B., Bhatt, A.B. (2014). Adult Congenital Heart Disease (ACHD). In: Gaggin, H., Januzzi, Jr., J. (eds) MGH Cardiology Board Review. Springer, London. https://doi.org/10.1007/978-1-4471-4483-0_21
Download citation
DOI: https://doi.org/10.1007/978-1-4471-4483-0_21
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-4482-3
Online ISBN: 978-1-4471-4483-0
eBook Packages: MedicineMedicine (R0)