
Abstract
Non-invasive imaging plays an important role in the management of cardiac diseases. While chest radiography forms a standard part of the diagnostic work-up and follow-up of many cardiac patients, evolving technology related to cardiac computed tomography (CT) and cardiovascular magnetic resonance (CMR) imaging have contributed substantially to the diagnosis and prognosis of various cardiac pathologies. This chapter describes chest radiography findings of cardiopulmonary abnormalities and diseases, including recognition of valvular prostheses as well as pericardial and aortic abnormalities. This is followed by a section on cardiac CT and CMR where scan modes and sequences, indications specific to cardiology and safety issues are addressed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Right Ventricular
- Cardiac Magnetic Resonance
- Cardiac Magnetic Resonance
- Late Gadolinium Enhancement
- Left Atrial
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Non-invasive imaging plays an important role in the management of cardiac diseases. While chest radiography forms a standard part of the diagnostic work-up and follow-up of many cardiac patients, evolving technology related to cardiac computed tomography (CT) and cardiovascular magnetic resonance (CMR) imaging have contributed substantially to the diagnosis and prognosis of various cardiac pathologies. This chapter describes chest radiography findings of cardiopulmonary abnormalities and diseases, including recognition of valvular prostheses as well as pericardial and aortic abnormalities. This is followed by a section on cardiac CT and CMR where scan modes and sequences, indications specific to cardiology and safety issues are addressed.
Chest Radiography
Advantages
Quick, portable, minimal radiation (0.02 millisieverts [mSv]), useful for serial follow-up
Normal Chest X-ray (CXR) Findings
-
Heart
-
Normal cardiothoracic ratio of the heart width to the chest width is <50 % on postero-anterior (PA) projection
-
-
Diaphragm
-
Normal chest expansion on CXR : 6 ± 1 anterior ribs or 9 ± 1 posterior ribs, right hemi-diaphragm higher than the left by up to 3 cm in 95 % of cases
-
-
Hila
-
Left hilum usually higher by approximately 1 cm than the right hilum, equal density
-
Abnormal CXR Findings
-
Dextroposition
-
In situs solitus, the position of the heart is on the right side secondary to a non-cardiac abnormality e.g. scoliosis, pneumonectomy, pulmonary agenesis, right pneumothorax, chronic volume loss or diaphragmatic hernia
-
-
Dextrocardia with situs inversus
-
Heart on the right side with inverted abdominal viscera and lung morphology (Fig. 2-1). Thoracic situs is determined by the anatomy of the trachea and lungs, not the position of aortic arch or cardiac apex
Figure 2-1 
Dextrocardia with situs inversus. Frontal CXR demonstrating both the cardiac apical silhouette and gastric air bubble are on the right side. Note the “L” marker on the upper right hand corner signifying left
-
-
Dextroversion
-
Counter-clockwise rotation of a normally developed heart in the right hemithorax. On CXR, the apex is not evident as it lies behind the sternum, the left heart border is formed by the left atrium, the right border is formed by the right ventricle and the right atrium is in a posterior position. The aortic knob is in the normal left-sided position.
-
-
“Boot-shaped” heart
-
Hallmark of Tetralogy of Fallot, due to right ventricular hypertrophy. The apical curvature of the left heart border is elevated “coeur en sabot” (Fig. 2-2a)
Figure 2-2 
Tetralogy of Fallot. (a) CXR showing elevation of the apical curvature of the left heart border known as “coeur en sabot”. (b) Cardiac CT showing an overriding aorta (Ao), ventricular septal defect patch (arrow), and right ventricular (RV) hypertrophy. The pulmonary stenosis is not shown on this CT slice. LV left ventricle
-
-
Mediastinal enlargement
-
Technical factors causing width of mediastinum to appear exaggerated: patient positioning, antero-posterior (AP) projection or incomplete inspiration
-
Pathological causes: aortic dissection, lymphadenopathy, thyroid, thymus, tumor
-
-
Enlarged cardiac silhouette
-
Pericardial effusion, left ventricular (LV) dilatation, LV aneurysm
-
-
Unequal hilar densities
-
Rotated film, lymph nodes, tumor
-
-
Hilar enlargement
-
Pulmonary hypertension, lymphadenopathy (tuberculosis, sarcoid, lymphoma)
-
-
Elevated hemidiaphragm
-
Loss of lung volume, phrenic nerve palsy (e.g. post coronary artery bypass graft [CABG] surgery), subpulmonic effusion, subphrenic abscess, diaphragmatic rupture (e.g. post trauma), hepatomegaly
-
-
Increased translucency in lung fields
-
Pneumothorax (absent vascular markings with visible lung border), pulmonary hypertension, pulmonary emboli, hyperinflation and bullous changes in chronic obstructive pulmonary disease
-


Cardiopulmonary Abnormalities/Diseases on CXR
-
Heart Failure
-
Cardiomegaly
-
Kerley A lines: long (2–6 cm), unbranching lines seen coursing diagonally towards the hila caused by distension of anastomotic channels between peripheral and central lymphatics of the lungs. Kerley A lines are not seen without Kerley B or C lines.
-
Kerley B lines: thickened interlobular septa visible as short linear opacities (1–2 cm) in the subpleural regions indicative of interstitial pulmonary edema
-
Kerley C lines: seen as fine reticular opacities which may represent anastomotic lymphatics or superimposition of many Kerley B lines. Kerley C lines do not reach the pleura and do not course radially away from the hila
-
Peribronchial cuffing due to edema of the bronchial walls and peribronchial connective tissues
-
Poor distinction of lower lobe pulmonary vessels
-
Greater caliber of upper lobe vessels to lower lung zones
-
Pulmonary hila become enlarged and hazy
-
Bilateral patchy alveolar infiltrates (bat’s wing appearance)
-
Pleural effusions
-
Chronic left atrial (LA) hypertension results in pulmonary hypertensive changes, right ventricular (RV) dilatation.
-
-
LA enlargement
-
Straightening of LA appendage segment between level of the main pulmonary artery and LV on the left heart border, double density to the right of the spine on PA CXR with increasing LA enlargement, splaying of carina >90°.
-
-
-
Pulmonary embolism
-
Oligemia
-
“Westermark sign” a dilatation of the pulmonary vessels proximal to an embolism along with collapse of distal vessels, sometimes with a sharp cutoff
-
Hampton hump, a triangular or rounded pleural-based infiltrate with the apex pointed toward the hilum, suggestive of pulmonary infarction
-
-
Pulmonary hypertension
-
Gradual taper of caliber between dilated central and hilar pulmonary arteries and smaller peripheral vessels (Fig. 2-3), if secondary to left-to-right shunting, the peripheral shunt vessels branch and extend towards the lung periphery
Figure 2-3 
Pulmonary hypertension. CXR showing prominence of the main pulmonary artery and dilated left and right pulmonary arteries (arrows) associated with pruning of the peripheral pulmonary vasculature
-
-
Reduced pulmonary blood flow
-
Small caliber central and hilar pulmonary arterial branches, reduced pulmonary vascular markings, seen in Tetralogy of Fallot, pulmonary atresia with ventricular septal defect, Ebstein’s anomaly, tricuspid atresia
-
-
Right ventricular hypertrophy
-
Right ventricle is a midline and anterior structure and thus does not form a cardiac border in the PA projection, however in RV hypertrophy the apex may be elevated from the diaphragm and the left lower cardiac contour may become more rounded
-
-
Scimitar syndrome
-
Partial or total anomalous pulmonary venous return of the right lung veins to the inferior vena cava just above or below the diaphragm, frequently associated with right lung and right pulmonary artery hypoplasia
-
PA CXR: decrease in the size of the right thorax, shift of mediastinal structures and heart to the right, presence of anomalous vein “scimitar” as a vertical structure coursing towards the right cardiophrenic angle closely in parallel with the right atrial border
-

Pericardial Abnormalities
-
Pericardial Effusion
-
An abrupt asymmetrical change in the dimension of the cardiac silhouette without a change in the cardiac chamber size, larger effusions result in the appearance of a ‘globular’ shaped heart, ‘fat pad’ sign on lateral CXR is positive when an anterior pericardial stripe (separation by pericardial fluid between the pericardial fat posteriorly from the mediastinal fat anteriorly) is thicker than 2 cm
-
Echocardiography most commonly used to confirm the diagnosis
-
-
Pericardial calcification
-
Irregular calcification along the heart border, coexisting cardiac enlargement if large pericardial effusion (Fig. 2-4)
Figure 2-4 
Pericardial calcification. (a) CXR and (b) CT image demonstrating calcification along the inferior cardiac border (arrow)
-
-
Pericardial cyst
-
Well demarcated, rounded mass more commonly near the right cardiophrenic border than the left cardiophrenic border, can have a pointed upper border, pericardial diverticulae changes contours and size during deep inspiration
-
-
Congenital absence of the pericardium
-
“Snoopy sign” with displacement of the LV and pulmonary artery towards the left side
-

Abnormalities of the Aorta
Calcification usually signifies degenerative intimal change, such as from atherosclerosis
-
Coarctation
-
“3” sign due to diminution of aortic arch segment with a concave notch in the proximal descending aorta and interruption of the descending aorta shadow distal to the coarctation, rib notching evident if retrograde collateral flow to the post-coarctation aorta by dilated intercostal arteries (Fig. 2-5a)
Figure 2-5 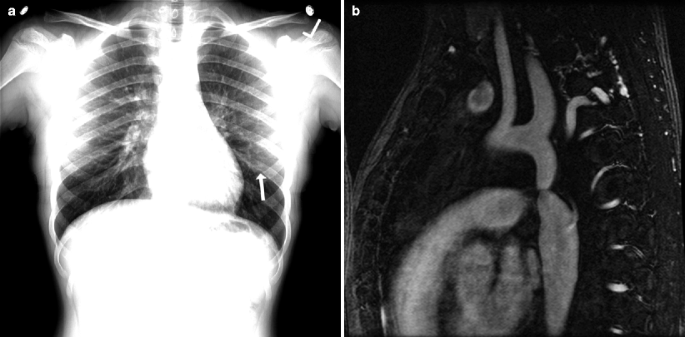
Aortic coarctation. (a) CXR showing left sided rib notching (arrow) due to retrograde collateral flow to the post-coarctation aorta by dilated intercostal arteries. (b) Cardiac Magnetic Resonance angiography demonstrating the aortic coarctation in the same patient
-
-
Thoracic aorta dilatation
-
Increased curvature of the mid right heart border on PA projection or anterior aortic border on lateral projection suggest ascending aortic enlargement
-
-
Aortic dissection
-
Prominent aortic arch from hypertension, atherosclerosis, connective tissue disorders, vasculitis, bicuspid aortic valve, blunt chest trauma or iatrogenic causes
-
Abnormal if diameter >4 cm, focal pathological dilatation especially with widening of the arch beyond the origin of the left subclavian artery (Fig. 2-6a)
Figure 2-6 
Aortic dissection. (a) CXR demonstrating a widened mediastinum (>4 cm, white arrows) in a patient with aortic dissection after blunt chest trauma. (b) Cardiac CT confirms a DeBakey Type 1 aortic dissection where the intimal tear/dissection flap (black arrows) originates in the ascending aorta and propagates to the aortic arch and descending aorta
-
Other CXR findings may include obliteration of the aortic knob, tracheal deviation, depression of the left main stem bronchus
-
Pleural effusions, usually left sided, are associated with descending aortic dissection
-
-
Right-sided aortic arch
-
The descending aorta typically runs parallel to the spine in continuity to the aortic arch on the left side on PA CXR, except in cases of a right sided aortic arch
-


Identification of Valvular Prostheses on CXR (Fig. 2-7)

(a) Frontal and (b) Lateral CXR demonstrating the anatomic relationship of a patient with prosthetic aortic (AV) and mitral valve (MV) replacements and tricuspid valve (TV) annuloplasty ring. The AV is situated higher and is smaller and more anterior to the mitral valve on the lateral CXR. The TV annuloplasty ring is aligned medial-laterally and is positioned to the right of and below the AV
-
Apart from homografts, prosthetic valves are radio-opaque
-
Caged valves and heterografts: direction of flow is from the base ring to the struts
-
Disc valves: the direction of flow is appreciated if the disc is seen in an open position
-
Aortic valve
-
The opening of the valve ring is directed more vertically, facing obliquely and to the right, aortic valve is usually higher, smaller and more anterior to the mitral valve on lateral CXR, perceived direction of blood flow is towards the ascending aorta
-
-
Mitral valve
-
Situated lower and more to the left than aortic valves, perceived direction of flow is towards the apex
-
-
Tricuspid valve
-
Aligned in a medial-lateral direction, to the right of mitral valve and below the aortic valve
-
Cardiac Computed Tomography (CT)
Most current multi-detector CT scanners (64-, 256- and 320-slice scanners) have similar spatial resolution, however the increased detector slices and larger detector width allow more coverage of the heart in each heartbeat. Dual source CT scanners consist of two X-ray tube sources leading to improved temporal resolution to 75 ms. Spatial resolution is how close two objects can be discernible from each other. Temporal resolution is how fast an image could be acquired such that motion does not create image blurring, similar to the shutter speed of a camera.
Advantages and Disadvantages of Cardiac CT (Table 2-1)
CT Scan Acquisition Modes (Table 2-2)
Appropriate CT Indications
Appropriate CT indications: 2010 Appropriate use criteria for cardiac computed tomography [1].
-
A.
Indications for non-contrast coronary calcium score (CCS)
-
Risk assessment in asymptomatic patients without known coronary artery disease (CAD):
-
At intermediate risk of CAD (correlates with 10-year absolute coronary heart disease [CHD] risk between 10 and 20 %)
-
At low risk of CAD (correlates with 10-year absolute CHD risk <10 %) with a family history of premature CAD
-
Patients with an Agatston score of >400 have a tenfold increased risk of cardiac events compared to a score of 0 [2]
-
The absence of calcium does not imply no significant coronary stenosis as 8–10 % of stenoses can be caused by non-calcified plaque.
-
-
-
-
B.
Indications for CT angiography (CTA)
-
Detection of CAD in symptomatic patients without known CAD who present with:
-
Non acute symptoms (stable chest pain) possibly representing an ischemic equivalent with
-
intermediate pretest probability of CAD, or
-
low pretest probability of CAD with uninterpretable electrocardiogram (ECG) or unable to exercise
-
-
Acute symptoms with suspicion of acute coronary syndrome, low to intermediate pretest probability of CAD without high risk ECG changes or elevated cardiac biomarkers (Fig. 2-8)
Figure 2-8 
Severe stenosis in the left anterior descending artery (LAD) due to non-calcified plaque (arrow). Curved multi-planar reformat cardiac CTA image in a patient presenting with acute chest pain and low-intermediate pre-test probability of acute coronary syndrome without elevated cardiac biomarkers or ischemic ECG changes
-
-
Detection of CAD in other clinical scenarios
-
Newly diagnosed clinical heart failure with no prior CAD and reduced LV ejection fraction (low to intermediate pretest probability of CAD)
-
Pre-operative coronary assessment prior to non-coronary cardiac surgery (intermediate pretest probability of CAD)
-
-
CTA in the setting of prior test results
-
Prior normal ECG exercise testing with continued symptoms, prior Duke Treadmill score with intermediate risk findings
-
Discordant ECG exercise and imaging results, prior equivocal stress imaging procedure
-
Evaluation of new or worsening symptoms in the setting of past normal stress imaging study
-
Meta-analysis shows good diagnostic accuracy for detection of obstructive CAD (≥50 % stenosis) with sensitivity 98 % and specificity 88 % [3].
-
Due to high negative predictive values of 95–100 %, coronary CTA has been used to “rule out” obstructive CAD in chest pain patients with low to intermediate risk of CAD.
-
CT delayed enhancement: myocardial scar detectable on non-contrast delayed enhancement scans, good concordance regarding the presence of delayed enhancement in CT and cardiac magnetic resonance imaging (CMR) on a per-segment basis, though less accurate than CMR, and not clinical routine.
-
-
-
Post revascularization (coronary artery bypass graft surgery (CABG) or percutaneous coronary intervention)
-
Evaluation of graft patency after CABG in symptomatic patients
-
CT ideal for graft assessment as high sensitivity (96 %), specificity (92 %) [4]
-
Native coronary vessels are typically heavily calcified in this setting, limiting the diagnostic accuracy for stenosis evaluation
-
-
Localization of coronary bypass grafts and other retrosternal anatomy prior to reoperative chest or cardiac surgery
-
Evaluation of left main coronary stent (diameter ≥3 mm) in asymptomatic patients
-
-
Assessment of adult congenital heart disease
-
Coronary anomalies (Fig. 2-9)
Figure 2-9 
Anomalous right coronary artery with inter-arterial course. Cardiac CTA image demonstrating an anomalous right coronary artery (arrow) arising from the left coronary cusp (LCC) with an inter-arterial course between the aorta and pulmonary artery (PA). LA left atrium, LSPV left superior pulmonary vein, NCC non-coronary cusp, RA right atrium, RCC right coronary cusp, RVOT right ventricular outflow tract
-
Anomalies of thoracic arteriovenous or aortic vessels (aorto-venous fistulas, aortic coarctation)
-
Adult congenital heart disease (Figs. 2-2b and 2-10)
Figure 2-10 
Patent ductus arteriosus (PDA). Cardiac CTA images (a, maximal intensity project; b, volume rendered image) demonstrating a PDA (arrow) with contrast traversing from the aorta to pulmonary artery (PA)
-
-
Assessment of ventricular morphology and function
-
If inadequate imaging from other noninvasive methods not requiring radiation (such as echocardiography or CMR):
-
Evaluation of LV function following acute myocardial infarction or in heart failure patients Quantitative evaluation of RV size and function, assessment of RV morphology (focal aneurysm), in suspected arrhythmogenic RV dysplasia
-
-
Pre-procedural planning for electrophysiology procedures
-
Evaluation of pulmonary vein and LA anatomy (Fig. 2-11)
Figure 2-11 
Pulmonary venous anatomy by CT prior to atrial fibrillation ablation. Volume rendered contrast-enhanced CT image showing the left atrium and pulmonary venous anatomy. This CT dataset is used to co-register with 3-dimensional electroanatomic map in the electrophysiology laboratory for atrial fibrillation ablation
-
Co-registration with electroanatomic mapping prior to pulmonary vein ablation
-
Assessment for LA appendage thrombus (Fig. 2-12), but confirmation with transesophageal echocardiography still required
Figure 2-12 
Left atrial appendage (LAA) thrombus. Contrast-enhanced cardiac CT shows a hypoattenuation filling defect in the LAA on arterial phase imaging, which may represent LAA thrombus or slow flow. A non-contrast delay scan (figure not shown) was subsequently performed within 1 min with persistence of the filling defect, suggesting a LAA thrombus. Transesophageal echocardiography is required for definitive confirmation of LAA thrombus. Ao aorta, PA pulmonary artery
-
-
Evaluation of coronary vein anatomy such as prior to biventricular pacemaker implantation (Fig. 2-13)
Figure 2-13 
Coronary venous anatomy by contrast-enhanced cardiac CT. Volume rendered CT image showing the coronary venous system. CT venography may be used pre-procedurally to facilitate cardiac resynchronization therapy implantation. CS coronary sinus, MCV middle cardiac vein, PVLV1 first posterior vein to the left ventricle
-
-
Evaluation of intra and extra cardiac structures
-
If other imaging techniques are inadequate, CT can be used for characterization of native and prosthetic cardiac valves, cardiac masses (tumors, thrombus)
-
CT is less sensitive for diagnosing valvular vegetations but useful for identifying paravalvular abscesses
-
-
Evaluation of pericardial anatomy
-
Pericardial effusions, thickening, fat, calcification (Fig. 2-4b), tumors, cysts
-
CMR and echocardiography for constrictive physiology assessment
-
-
Diagnosis of other non-cardiac pathologies
-
Thoracic aorta assessment: aortic aneurysm, dissection (Fig. 2-6b), thoracic trauma, tears, intramural hematoma, mediastinal hematomas
-
Incidental findings: lung (pulmonary emboli (Fig. 2-14), pneumonia, nodules, effusion, atelectasis), liver (hemangiomas, cysts, tumor), bone (fractures, lytic lesions, degenerative disc disease), gastro-intestinal (hiatus hernia, esophageal thickening), mediastinal lymphadenopathy
Figure 2-14 
Pulmonary emboli (PE). Cardiac CTA images demonstrating the presence of PE (arrows) found incidentally in a patient presenting with acute chest pain
-
-
-







Medications in CT
-
Beta-blockers
-
Given to reduce heart rate (HR), HR variability and ectopy to minimize motion artifact and allow accurate ECG-triggering (if HR >60–65 bpm)
-
-
Calcium channel blockers
-
Given if beta-blockers are contraindicated (in limited centers)
-
-
Sublingual nitroglycerin
-
If not contraindicated, it is administered for vasodilatory effects immediately prior to coronary CTA. Diagnostic accuracy is reduced if nitroglycerin is not given
-
-
Medications to avoid
-
Metformin due to small potential risk of lactic acidosis from acute kidney failure related to contrast dye administration. Hold for 48 hours following scan
-
CT Safety
-
Ionizing radiation
-
Adhere to the ALARA (As Low As Reasonably Achievable) principle regarding radiation with dose saving algorithms, minimization of repeated scans
-
Stochastic effects
-
These effects occur by chance and are not dependent on the radiation dose received. An example is development of cancer in the future. There is also no lower threshold of radiation dose where it is certain that an adverse effect cannot occur.
-
-
Non-stochastic or deterministic effects
-
These effects are directly related to the radiation dose received. For example, a large radiation dose may result in skin burns, hair loss, cataracts, sterility, gastrointestinal syndrome (e.g. ulcers), or hematopoietic syndrome (e.g. bone marrow suppression). There is a clear relationship between radiation dose and effect.
-
-
-
Side-effects related to iodinated contrast
-
Tissue extravasation
-
Watch for compartment syndrome and infection
-
-
Allergy
-
Resulting in skin reactions (itch, rash) or anaphylaxis – prior history of mild contrast reaction (hives or less) requires premedication with steroid and anti-histamine prior to contrast administration
-
-
Contrast Induced Nephropathy
-
Occurs when there is a temporal relationship between deterioration of renal function and the administration of intravenous contrast, in the absence of any other etiology
-
It can be defined as either a >25 % increase of serum creatinine or an absolute increase in serum creatinine of 0.5 mg/dL after a radiographic examination using a contrast agent
-
This condition occurs in <2 % of patients, is very unlikely in patients with normal renal function (estimate Glomerular Filtration Rate >60 mL/min/1.73 m2), typically occurs 48 hours post contrast, persists for 2–5 days and resolves by 7–10 days [5]
-
-
Cardiac Magnetic Resonance (CMR) Imaging
-
CMR imaging uses magnetic and radiofrequency fields to generate signals from hydrogen
-
The typical magnetic field strength used for clinical CMR are 1.0, 1.5 and 3.0 Tesla
Advantages and Disadvantages of CMR (Table 2-3)
CMR Scan Sequences
-
Dark Blood Imaging
-
Flowing blood appears dark while slow moving structures such as myocardium is bright. T2 weighted images are sensitive to water content and will be represented as high signal in areas of acute injury such as myocarditis and infarction.
-
-
Bright blood Imaging
-
Allows acquisition of cine images for assessment of cardiac function. Steady state free precession technique is commonly used for this purpose
-
-
Phase-contrast
-
Allows measurement of velocity and quantification of blood flow
-
-
Perfusion
-
Contrast agents such as gadolinium (Gd), which shortens T1 relaxation time, can be imaged as it transits through cardiac structures
-
-
MR angiography
-
Allows 3-dimensional examination of complex cardiac and vascular structures
-
-
Late gadolinium enhancement
-
Delayed hyperenhancement of Gd (∼10 min after administration) is seen in areas of myocardial necrosis and fibrosis
-
CMR Indications [6]
-
Ischemic Heart disease
-
Vasodilator perfusion or dobutamine stress function CMR in symptomatic patients with intermediate pre-test probability of CAD with uninterpretable ECG or cannot exercise
-
Stress perfusion to detect CAD can be performed with first-pass Gd perfusion imaging
-
Meta-analysis of 1,516 patients demonstrated perfusion imaging with CMR has a sensitivity 91 %, specificity 83 % in detecting CAD (≥50 % stenosis) [7]
-
CMR parameters (LV ejection fraction, aortic flow, delayed enhancement) is incremental to perfusion data for predicting adverse outcomes [8]
-
-
Viability
-
Cardiomyopathy
-
CMR can provide accurate measurements of biventricular function, volume, and tissue characterization for diagnosis, management, and prognosis
-
It is appropriate to quantify LV function with CMR if echocardiographic imaging is technically limited or discordant with prior tests
-
Ischemic cardiomyopathy: The pattern of late Gd enhancement is subendocardial and may be transmural with its location in a specific coronary artery distribution (Table 2-4)
Table 2-4 Distribution of late Gd enhancement of various cardiomyopathies and prognostic value
-
-
Myocarditis
-
The presence of two CMR criteria for myocarditis has a sensitivity of 67 % and specificity of 91 % for the diagnosis of myocarditis [11]
-
Late Gd enhancement is typically subepicardial (focal or widespread)
-
Increased T2 signal suggesting myocardial edema (regional or global, Fig. 2-15)
Figure 2-15 
CMR T2 assessment for myocarditis. Offline measurement for increased global T2 myocardial enhancement corrected for skeletal muscle, which is one parameter for assessment of myocarditis
-
Early global relative Gd enhancement indicating myocardial hyperemia and capillary leakage (Fig. 2-16)
Figure 2-16 
CMR early global relative gadolinium (Gd) assessment for myocarditis. Offline measurement comparing the pre- and post-Gd images. The ratios of pre-Gd myocardial: skeletal muscle (a/b) are compared to the post-Gd myocardial: skeletal muscle (c/d) signal intensities
-
-
-
Sarcoidosis
-
Presence of late Gd enhancement can be in any distribution (Fig. 2-17) and is associated with subsequent adverse cardiac events [12]
Figure 2-17 
Cardiac sarcoidosis. CMR delayed enhancement of the left ventricular short-axis at the mid-ventricular level showing patchy, myocardial scarring in the inferior septum (arrow) in a patient with known systemic sarcoidosis
-
CMR has a sensitivity of 100 % (78–100 %) and specificity of 78 % (64–89 %) with an overall accuracy of ∼80 % in diagnosing cardiac sarcoidosis [13]
-
-
Amyloidosis
-
Hypertrophic cardiomyopathy
-
CMR able to identify increased regional wall thickness not appreciated on other imaging techniques as well as accurate quantification of LV mass
-
Various patterns of late Gd enhancement are identified in patients with hypertrophic cardiomyopathy (Fig. 2-18) and are shown to be associated with adverse prognosis [15]
Figure 2-18 
Hypertrophic cardiomyopathy with midwall delay gadolinium enhancement of the left ventricle (LV) which is associated with increased risk for sudden cardiac death. Note the thick myocardial wall. RV right ventricle
-
-
Hemochromatosis
-
T2* measurement of myocardium on CMR can be used to identify subjects with cardiac involvement in hemochromatosis, with a T2* of less than 20 ms is associated with LV systolic dysfunction [16]
-
-
Arrhythmogenic Right Ventricular Dysplasia
-
Quantitative evaluation of RV size and function, assessment of RV morphology (focal aneurysm) in suspected arrhythmogenic RV dysplasia
-
Fatty deposition and fibrosis in the RV by CMR are not part of the modified Task Force criteria [17]
-
-
Non-compaction cardiomyopathy
-
A diastolic ratio of non compacted to compacted myocardium of greater than 2.3 has a sensitivity of 86 % and specificity of 99 % for diagnosing non compaction cardiomyopathy [18]
-
-
Congenital Heart Disease
-
Quantification of LV and RV mass, volume and ejection fraction
-
Quantification of valvular disease
-
Assessment of great vessels, coronary anomalies, flow through surgical conduits
-
Specific indications for CMR in congenital heart disease
-
Shunt size (Qp/Qs) calculation with phase contrast imaging
-
Assessing anomalous pulmonary and systemic venous return
-
Aortic abnormalities such as coarctation (Fig. 2-5b), aortic aneurysm
-
Pulmonary artery abnormalities i.e. pulmonary atresia, stenosis
-
Systemic to pulmonary collaterals
-
Complex congenital disease assessment and follow-up post surgery i.e. post atrial/arterial switch operation for transposition of great arteries, Fontan operations and post-Tetralogy of Fallot repair
-
-
-
Cardiac Tumors
-
CMR is an excellent imaging modality for visualization and characterization of cardiac masses
-
The main advantage of CMR includes better contrast resolution, multiplanar capability, ability to assess functional impact of the tumor, tissue characterization and detection of vascularity of the tumor with first pass perfusion imaging
-
Differentiating intracardiac thrombus from tumor and benign from malignant cardiac masses is an important strength of CMR
-
-
Pericardial disease [19]
-
Assessment of pericardial disease such as pericardial mass and pericardial constriction
-
Features of pericardial constriction on CMR (thickened pericardium ≥4 mm, paradoxical motion of the interventricular septum, lack of normal breaking of tag lines on tagging sequence during cardiac contraction due to shear motion between visceral and parietal pericardium (Fig. 2-19), calcified pericardium)
Figure 2-19 
Pericardial constriction. Tagging CMR sequences showing unbroken taglines over the pericardium during ventricular diastole and bending of taglines over the pericardium during systole suggesting pericardial adhesions
-
-
Valvular heart disease
-
If other forms of imaging such as echocardiography is technically limited, CMR can assess valvular function
-
Qualitative assessment of regurgitant and stenotic jets can be seen on cine CMR
-
Quantitative assessment of stenosis can be measured by planimetry or using phase contrast sequences to determine peak velocity across the valve
-
Regurgitant volume and fraction can be assessed by phase contrast sequences (determining the forward and reverse flow) or by assessing the differences in RV and LV stroke volume.
-
-
Evaluation of pulmonary vein and left atrial (LA) anatomy
-
Co-registration with electroanatomic mapping prior to pulmonary vein ablation
-





CMR Safety
-
The use of Gd in end-stage renal patients is associated with a rare but serious complication of nephrogenic systemic fibrosis, which results in fibrosis of skin overlying the extremities and truck and deeper structures including muscle, lung and heart
-
Ferromagnetic implants may lead to complications with CMR and should be screened prior to CMR [20]
-
It is generally recommended a waiting period of about 6 weeks post implantation of weakly ferromagnetic devices such as cardiac valves and stents before CMR
-
CMR in patients with pacemakers and implantable cardioverter-defibrillators can potentially lead to heating of the tip of the lead, inhibiting pacing output, activating tachyarrhythmia therapy or damage to the device
-
CMR-compatible pacemaker systems have recently become available, although their use is currently limited
Review Questions
-
1.
According to the 2010 appropriate use criteria for cardiac computed tomography; which of the following is false?
-
(a)
It is appropriate to perform a CT calcium score in an asymptomatic patient with intermediate pretest probability of coronary artery disease
-
(b)
It is appropriate to perform CT angiography in an asymptomatic patient with intermediate pretest probability of coronary artery disease
-
(c)
It is appropriate to perform CT angiography in a patient with acute chest pain and intermediate pretest probability of coronary artery disease with normal ECG and cardiac biomarkers
-
(d)
It is appropriate to perform CT angiography for risk assessment in an asymptomatic patient with prior 3.5 mm left main stent
-
(e)
It is appropriate to perform CT angiography in a symptomatic patient with intermediate pretest probability of coronary artery disease with interpretable ECG and able to exercise
-
(a)
-
2.
What artificial valve is shown in this CXR (Fig. 2-20)?

Figure 2-20
-
(a)
Mechanical mitral valve
-
(b)
Mechanic aortic valve
-
(c)
Bioprosthetic aortic valve
-
(d)
Mechanical tricuspid valve
-
(e)
Bioprosthetic mitral valve
-
(a)
-
3.
A 59 year old man who presented with symptoms of heart failure after mediastinal irradiation for Hodgkin lymphoma undergoes CMR. Which of the following feature is NOT consistent with pericardial constriction on CMR?
-
(a)
Pericardial thickness ≥ 4 mm
-
(b)
Left ventricular myocardial trabeculation ratio >2.3
-
(c)
Lack of normal breaking of tag lines during cardiac contraction
-
(d)
Pericardial calcification
-
(e)
Septal flattening on early diastolic filling
-
(a)
-
4.
Which of the following complications does not occur with CT angiography?
-
(a)
Nephrogenic systemic fibrosis
-
(b)
Anaphylaxis
-
(c)
Compartment syndrome of the arm
-
(d)
Contrast induced nephropathy
-
(e)
Bradycardia
-
(a)
-
5.
Which of the following is a stochastic effect from ionizing radiation?
-
(a)
Radiation burns
-
(b)
Cancer
-
(c)
Permanent sterility
-
(d)
Radiation sickness
-
(e)
Cataracts
-
(a)
-
6.
A 52 year old woman with hypertension and dyslipidemia presents to the emergency department with worsening chest discomfort on minimal exertion. Her ECG was non-diagnostic and two sets of troponin were negative. She underwent coronary CTA. This image (Fig. 2-21) demonstrates:

Figure 2-21
-
(a)
Anomalous left coronary artery arising from the right Sinus of Valsalva with an interarterial course
-
(b)
Severe aortic regurgitation due to aortic dissection
-
(c)
Severe stenosis in the mid right coronary artery
-
(d)
Sinus venosus atrial septal defect
-
(e)
Unroofed coronary sinus
-
(a)
-
7.
A 60 year old man with Type II diabetes on metformin and hypertension presents with dyspnea and impaired left ventricular systolic function on echocardiography. Based on the delayed gadolinium enhancement on CMR (Fig. 2-22), what is the most likely cause of the systolic dysfunction?

Figure 2-22
Figure 2-23 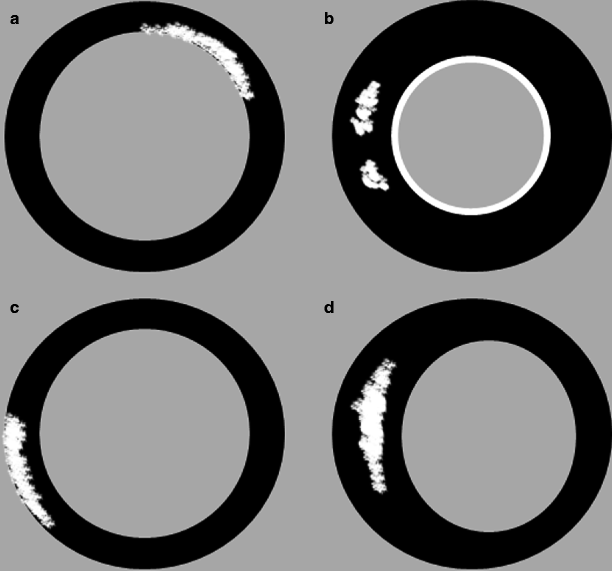
Distribution of late gadolinium enhancement in various cardiac conditions. (a) Ischemic (subendocardial enhancement), (b) Amyloid (global subendocardial enhancement), (c) Myocarditis (subepicardial enhancement), (d) Hypertrophic cardiomyopathy (mid wall enhancement)
-
(a)
Myocarditits
-
(b)
Amyloid
-
(c)
Previous left anterior descending artery territory myocardial infarction
-
(d)
Previous right coronary artery territory myocardial infarction
-
(e)
Constrictive pericarditis
-
(a)
-
8.
A 35 year old man with back pain has the above finding on CT (Fig. 2-24), which of the following is false?

Figure 2-24
-
(a)
He may have an autosomal dominant genetic disorder
-
(b)
He may have a diastolic and systolic murmur on examination
-
(c)
He requires urgent surgical consultation
-
(d)
He has non-compaction of the left ventricle
-
(e)
He may have a mutation of the transforming growth factor beta receptor 1
-
(a)
-
9.
A 47 year old man presents for CTA to investigate first presentation of intermittent chest discomfort. He is a current smoker and has a past history of Type II diabetes on Metformin, dyslipidemia on Atorvastatin, erectile dysfunction on vardenafil and benign prostatic hypertrophy. On examination his heart rate is 79 bpm, he has a harsh ejection systolic murmur which becomes louder with the Valsalva maneuver and clear lung fields. Which of the following is not advised when performing CTA for this patient?
-
(a)
Withhold Metformin for 48 hours post CTA
-
(b)
Administration of metoprolol to achieve heart rate of 60–65 bpm
-
(c)
Administration of iodinated contrast for the coronary CTA
-
(d)
Administration of sublingual nitrates for coronary vasodilation to improve CTA accuracy
-
(e)
All the above can be advised or given
-
(a)





Answers
-
1.
(b) Non-contrast calcium score is used for risk assessment in asymptomatic patients without known coronary artery disease (CAD). It is inappropriate for coronary CT angiography to be performed for risk assessment in asymptomatic patients with no previous coronary artery disease with low to intermediate pretest probability of CAD.
-
2.
(e) The CXR demonstrates a bioprosthetic mitral valve with the perceived direction of flow is towards the apex.
-
3.
(b) The ratio of noncompacted to compacted left ventricular (LV) myocardium of >2.3 is consistent with LV noncompaction, which is not a feature of pericardial constriction.
-
4.
(a) Nephrogenic system fibrosis is a potential complication of gadolinium administration when undergoing CMR. Anaphylaxis and contrast induced nephropathy are potential complications of iodinated contrast administration used in cardiac CT, severe tissue extravasation of iodinated contrast may result in compartment syndrome of the arm and beta-blockers administered prior to coronary CTA can result in bradycardia.
-
5.
(b) Stochastic effects occur by chance and are not dependent on the radiation dose received e.g. cancer. There is also no lower threshold of radiation dose where it is certain that an adverse effect cannot occur. The other options are examples of non-stochastic effects, which are effects that are directly related to the radiation dose received; there is a clear relationship between radiation dose and non-stochastic effect.
-
6.
(c) This CT image demonstrates severe stenosis in the mid right coronary artery due to non-calcified plaque.
-
7.
(c) The subendocardial distribution of late gadolinium enhancement in the anterior wall on CMR is consistent with previous anterior myocardial infarction. The typical late gadolinium enhancement seen in myocarditis is subepicardial. Cardiac amyloid typically has global subendocardial delayed enhancement, rather than localized to a particular coronary distribution. The following diagram (Fig. 2-23) illustrates the distribution of late gadolinium enhancement in various cardiac conditions.
-
(a)
Ischemic (subendocardial enhancement)
-
(b)
Amyloid (global subendocardial enhancement)
-
(c)
Myocarditis (subepicardial enhancement)
-
(d)
Hypertrophic cardiomyopathy (mid wall enhancement)
-
(a)
-
8.
(d) This gentleman has a dilated aortic root and left ventricle. He may have Marfan’s syndrome which is an autosomal dominant genetic disorder, however patients with Loeys-Dietz syndrome may also have aortic aneurysms due to a mutation of the gene encoding transforming growth factor beta receptor one. Urgent surgical intervention is required in patients with an aortic diameter of 5 cm, however in patients with Marfan’s or Loeys-Dietz syndrome, earlier intervention is recommended at 4 cm. On CMR, the ratio of noncompacted to compacted myocardium of 2.3 has good accuracy for the diagnosis of non compaction cardiomyopathy. It is suggested a similar ratio could be applied to cardiac CT. However, the patient in this scenario does not have non-compaction.
-
9.
(d) The administration of nitroglycerin (400–800 μg of a sublingual tablet or sublingual spray) is performed immediately prior to coronary CTA to improve diagnostic accuracy by causing vasodilation of the coronary arteries. The patient in this scenario has clinical signs which may be due to hypertrophic obstructive cardiomyopathy and is taking vardenafil, which is a phosphodiesterase type 5 (PDE-5) inhibitor. Nitroglycerin should be avoided in patients with hypertrophic cardiomyopathy with outflow tract obstruction or severe aortic stenosis as nitrates many reduce preload, exacerbate obstruction and result in hypotension, syncope or worsening heart failure. Nitroglycerin should also be avoided in patients on PDE-5 inhibitors.
Abbreviations
- ALARA:
-
As Low As Reasonably Achievable
- AP:
-
Antero-posterior
- bpm:
-
Beats per minute
- CABG:
-
Coronary artery bypass graft
- CAD:
-
Coronary artery disease
- CCS:
-
Coronary calcium score
- CHD:
-
Coronary heart disease
- CMR:
-
Cardiac magnetic resonance
- CT:
-
Computed tomography
- CTA:
-
Computed tomography angiography
- CXR:
-
Chest X-ray
- ECG:
-
Electrocardiogram
- Gd:
-
Gadolinium
- HR:
-
Heart rate
- LA:
-
Left atrial
- LV:
-
Left ventricular
- mSv:
-
Millisievert
- PA:
-
Postero-anterior
- RV:
-
Right ventricular
References
Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O’Gara P, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol. 2010;56(22):1864–94.
Pletcher MJ, Tice JA, Pignone M. Use of coronary calcification scores to predict coronary heart disease. JAMA. 2004;291(2):1831. author reply 2–3.
Stein PD, Yaekoub AY, Matta F, Sostman HD. 64-slice CT for diagnosis of coronary artery disease: a systematic review. Am J Med. 2008;121(8):715–25.
de Graaf FR, van Velzen JE, Witkowska AJ, Schuijf JD, van der Bijl N, Kroft LJ, et al. Diagnostic performance of 320-slice multidetector computed tomography coronary angiography in patients after coronary artery bypass grafting. Eur Radiol. 2011;21(11):2285–96.
Rao QA, Newhouse JH. Risk of nephropathy after intravenous administration of contrast material: a critical literature analysis. Radiology. 2006;239(2):392–7.
Hendel RC, Patel MR, Kramer CM, Poon M, Carr JC, Gerstad NA, et al. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006;48(7):1475–97.
Nandalur KR, Dwamena BA, Choudhri AF, Nandalur MR, Carlos RC. Diagnostic performance of stress cardiac magnetic resonance imaging in the detection of coronary artery disease: a meta-analysis. J Am Coll Cardiol. 2007;50(14):1343–53.
Bingham SE, Hachamovitch R. Incremental prognostic significance of combined cardiac magnetic resonance imaging, adenosine stress perfusion, delayed enhancement, and left ventricular function over preimaging information for the prediction of adverse events. Circulation. 2011;123(14):1509–18.
Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, et al. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999;100(19):1992–2002.
Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343(20):1445–53.
Friedrich MG, Sechtem U, Schulz-Menger J, Holmvang G, Alakija P, Cooper LT, et al. Cardiovascular magnetic resonance in myocarditis: a JACC White Paper. J Am Coll Cardiol. 2009;53(17):1475–87.
Patel MR, Cawley PJ, Heitner JF, Klem I, Parker MA, Jaroudi WA, et al. Detection of myocardial damage in patients with sarcoidosis. Circulation. 2009;120(20):1969–77.
Smedema JP, Snoep G, van Kroonenburgh MP, van Geuns RJ, Dassen WR, Gorgels AP, et al. Evaluation of the accuracy of gadolinium-enhanced cardiovascular magnetic resonance in the diagnosis of cardiac sarcoidosis. J Am Coll Cardiol. 2005;45(10):1683–90.
Maceira AM, Joshi J, Prasad SK, Moon JC, Perugini E, Harding I, et al. Cardiovascular magnetic resonance in cardiac amyloidosis. Circulation. 2005;111(2):186–93.
Moon JC, McKenna WJ, McCrohon JA, Elliott PM, Smith GC, Pennell DJ. Toward clinical risk assessment in hypertrophic cardiomyopathy with gadolinium cardiovascular magnetic resonance. J Am Coll Cardiol. 2003;41(9):1561–7.
Anderson LJ, Holden S, Davis B, Prescott E, Charrier CC, Bunce NH, et al. Cardiovascular T2-star (T2*) magnetic resonance for the early diagnosis of myocardial iron overload. Eur Heart J. 2001;22(23):2171–9.
Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, Bluemke DA, et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the task force criteria. Circulation. 2010;121(13):1533–41.
Petersen SE, Selvanayagam JB, Wiesmann F, Robson MD, Francis JM, Anderson RH, et al. Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging. J Am Coll Cardiol. 2005;46(1):101–5.
Bogaert J, Francone M. Cardiovascular magnetic resonance in pericardial diseases. J Cardiovasc Magn Reson. 2009;11:14.
Levine GN, Gomes AS, Arai AE, Bluemke DA, Flamm SD, Kanal E, et al. Safety of magnetic resonance imaging in patients with cardiovascular devices: an American Heart Association scientific statement from the Committee on Diagnostic and Interventional Cardiac Catheterization, Council on Clinical Cardiology, and the Council on Cardiovascular Radiology and Intervention: endorsed by the American College of Cardiology Foundation, the North American Society for Cardiac Imaging, and the Society for Cardiovascular Magnetic Resonance. Circulation. 2007;116(24):2878–91.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
Thai, We., Wai, B., Truong, Q.A. (2014). Cardiac Noninvasive Imaging: Chest Radiography, Cardiovascular Magnetic Resonance and Computed Tomography of the Heart. In: Gaggin, H., Januzzi, Jr., J. (eds) MGH Cardiology Board Review. Springer, London. https://doi.org/10.1007/978-1-4471-4483-0_2
Download citation
DOI: https://doi.org/10.1007/978-1-4471-4483-0_2
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-4482-3
Online ISBN: 978-1-4471-4483-0
eBook Packages: MedicineMedicine (R0)