
Abstract
Calcification of the mitral valve and the mitral subvalvular apparatus can potentially complicate the MitraClip procedure by affecting leaflet grasp and increasing the risk of chordal or papillary muscle rupture. This case example shows a successful MitraClip procedure in a patient with extensive calcification of the mitral apparatus.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Clinical History
We report on an 86-year-old man who was repeatedly admitted to a local hospital because of congestive heart failure, stage NYHA IV, due to severe mitral regurgitation (MR). In 2006, he underwent coronary artery bypass grafting. Furthermore, he suffered from pulmonary hypertension, chronic renal failure, and peripheral vascular disease (EuroSCORE II: 12.72 %; log. EuroSCORE I: 35.17 %). Conventional surgery was denied because of very advanced age, previous bypass surgery with patent grafts, and comorbidities. Finally, the patient was referred to our center for evaluating the suitability for percutaneous mitral valve repair with MitraClip.
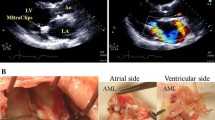
Pre-procedural transesophageal echocardiography revealed extensive calcification of the posterior mitral annulus, the posterior leaflet, and the chordae tendineae (possibly with chordal fusions) (Fig. 33.1a, b). The calcification of the chordae led to an asymmetric restriction of the leaflet motion (Fig. 33.2a, b) in both systole and diastole. In addition, there was a small P2 prolapse in this patient resulting in severe eccentric mitral regurgitation along the anteroseptal wall of the left atrium (Carpentier II and IIIa [1]) (Fig. 33.3a–d). The heavy calcifications of the leaflets and the subvalvular apparatus were felt to make MitraClip implantation more risky, including the possibility of chordal or papillary rupture. However, the patient was accepted for the procedure due to severe symptoms with recurrent cardiac decompensation and the lack of other treatment options.
Figures 33.4, 33.5, and 33.6 demonstrate the MitraClip implantation procedure. A first clip was placed directly into the PISA zone of the MR jet (Fig. 33.4a, b) creating a double orifice (Fig. 33.4c) with significant reduction of regurgitation grade (Fig. 33.4d). However, because of significant residual MR, a second clip was placed lateral to the first one (Fig. 33.5a). The mean gradient after implantation of the second clip was acceptable (5 mmHg), with reduction of regurgitation grade to mild MR (Fig. 33.6a, b). The patient was discharged 4 days after the procedure, with no periprocedural complications.
At 1-year follow-up, the patient reported a good quality of life and denied any symptoms of congestive heart failure. The 6-min walk test had increased from 240 m pre-procedural to 300 m at follow-up. TTE demonstrated only mild mitral regurgitation (Fig. 33.7).
Summary
Excessive calcification of the mitral valve apparatus may potentially complicate the MitraClip procedure and increase the risk of chordal or papillary rupture due to brittle tissue. However, with appropriate planning and meticulous technique, the procedure may be safely performed.


Transesophageal three-chamber views in diastole (a) and systole (b) demonstrating extensive calcification of the posterior mitral annulus, the posterior leaflet, the chordae tendineae (possibly with chordal fusions), and the heads of the papillary muscles


3D images of the mitral valve in diastole (a) and systole (b). Focal leaflet calcification is visible. The chordal calcifications provoke an asymmetric restriction of leaflet motion leading to poor leaflet coaptation in systole and a small P2 prolapse (b)




Transesophageal four-chamber views (a, b) and three-chamber views (c, d) with (b, d) and without (a, c) color Doppler show severe eccentric mitral regurgitation along the anteroseptal wall of the left atrium




Placement of a first MitraClip directly into the PISA zone of the MR jet (a, b) creating a double orifice (c) with visible MR reduction (d)


Placement of a second clip lateral from the first one (a) with a post-procedural mean gradient of 5 mmHg (b)


Color Doppler images demonstrate only mild residual MR (a: three-chamber view; b: four-chamber view)


TTE (four-chamber view) at 12-months follow-up confirms the presence of only mild MR
Reference
Carpentier A. Cardiac valve surgery—the “French correction”. J Thorac Cardiovasc Surg. 1983;86:323–37.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag London
About this chapter
Cite this chapter
Puls, M., Hünlich, M., Schillinger, W. (2013). MitraClip Implantation in Chronic Degenerative Mitral Regurgitation with Extensive Calcification. In: Feldman, T., Franzen, O., Low, R., Rogers, J., Yeo, K.K. (eds) Atlas of Percutaneous Edge-to-Edge Mitral Valve Repair. Springer, London. https://doi.org/10.1007/978-1-4471-4294-2_33
Download citation
DOI: https://doi.org/10.1007/978-1-4471-4294-2_33
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-4293-5
Online ISBN: 978-1-4471-4294-2
eBook Packages: MedicineMedicine (R0)