
Abstract
Hypertension is the most common cardiovascular condition to be seen in primary care. It also represents the strongest single modifiable risk factor with regards to future morbidity and mortality. The incidence of hypertension is predicted to continue to increase, being contributed to by an ageing population.
The major consequence of this largely asymptomatic condition is the development of cardiovascular sequelae. The aim of early diagnosis is to provide an opportunity to intervene in order to prevent or delay the onset of overt vascular disease. The positive effects of treatment have been proven in numerous randomised placebo-controlled trials. However since hypertension is usually asymptomatic and treatment is aimed at prevention of complications, targeting patients at highest risk while avoiding ‘medicalisation’ and causing side effects in people at low risk is challenging. This is especially the case in young people for whom a diagnosis of hypertension entails life-long treatment, based upon studies performed in older people. Using a clinical example we will review some of those challenges and how to deal with them in this chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Hypertension
- Young adult
- Blood pressure
- Essential hypertension
- Primary hypertension
- Secondary hypertension
Case: The Tense Technician
A Caucasian patient in his early-30s attended his primary care physician for the fourth time in 6 months. John had initially presented with coryzal symptoms, which had since resolved but had left him feeling tired, with a non-specific headache that was affecting his concentration at work. He was anxious that this could represent something serious, but the only worrying feature so far was a slightly raised blood pressure.
Why is hypertension important?
Hypertension is the leading contributor to global mortality [1, 2]. The increase in worldwide childhood and adult obesity, along with an ageing and increasingly sedentary population means that the incidence and prevalence is likely to continue to grow (Figs. 11.1 and 11.2) [3–5].

NHS National Statistics (2010) data showing the increasing incidence of hypertension with age (Reproduced with permission from National Statistics [3]. Copyright © 2011, Re-used with the permission of the Health and Social Care Information Centre. All rights reserved)

Prevalence of hypertension by gender and age (Data adapted from the Canadian Hypertension Education Program 10-year population study [4])
It is also the most significant reversible cause for cardiovascular disease with numerous studies proving that the control of hypertension can lower the risk of cardiovascular events and mortality [6]. Screening and effective control of raised blood pressure has public health benefits and is cost-effective [7], and is therefore endorsed by the British National Institute for Health and Clinical Excellence (NICE) [8]. Both the guidelines and the data are limited to patients within certain age groups and it is unclear whether the benefits of treatment extend to the young [9], in whom prevalence is estimated to be between 5 and 20 % for those aged between 24 and 32 [10]. However, it is generally assumed that earlier treatment is associated with greater benefits in terms of longevity and life free from disease [2, 11].
Hypertension is often classed as “primary” or “secondary,” with the latter being due to some specific identifiable additional condition (see below). On the other hand the pathogenesis of primary hypertension is often multifactorial, although the diagnosis and complications are known to be associated with several risk factors such as race, family history, diabetes mellitus, obesity, inactive lifestyle, high sodium intake and excessive alcohol consumption [8, 12, 13]. Psychosocial factors and depressive illnesses may increase the risk of chronically raised blood pressure [14, 15]. Recent evidence also links severe vitamin D deficiency with the subsequent development of hypertension [16].
Although it is usually asymptomatic in its early stages, untreated chronic hypertension contributes to the early development of cardiovascular disease, renal impairment and disability, regardless of the aetiology. There is a 7 % incremental risk of mortality from ischaemic heart disease (and 10 % from stroke) for every 2 mmHg step in systolic blood pressure [17].Epidemiological studies suggest that a 10 mmHg lower systolic blood pressure (or 5 mmHg lower diastolic blood pressure) is associated with a 50 % reduction in the risk of death from coronary artery disease or stroke (Fig. 11.3) [17]. Hypertension therefore is an important condition to recognise and address even in young adults and both lifestyle modification and anti-hypertensive therapies to achieve blood pressure reduction are a priority to reduce risk. However, treatment goals should be individualised to take patient characteristics and co-morbidities into account. Recently, there has been limited evidence to suggest that excessive lowering of the diastolic blood pressure to below 70 mmHg in the high-risk elderly population with co-existing severe coronary artery disease or diabetes, may be associated with an increase in cardiovascular complications [6, 18–20].

Association between mortality and systolic blood pressure separated by age (Data adapted with permission from a meta-analysis of individual data for one million adults. Adapted from Lewington et al. [17], Copyright 2002, with permission from Elsevier)
John’s general practitioner (GP) arranged for him to have a series of blood tests (full blood count, urea/electrolytes, glucose, thyroid function tests and estimated glomerular filtration rate), urinalysis and electrocardiogram. She also arranged for 24-h blood pressure monitoring in order to confirm the diagnosis.
How should a clinician proceed?
The use of ambulatory blood pressure monitoring (ABPM) is currently recommended by the NICE guidelines in order to confirm the diagnosis, when there are persistently elevated clinic blood pressure (BP) readings (between 140/90 and 180/110 mmHg) and an absence of end-organ damage (Fig. 11.4) [8]. Where ABPM is not available, home BP monitoring should be used since this shows a stronger correlation to daytime ABPM measurements than clinic BP readings [21, 22]. If clinic BP is the only available test, then this should be measured on at least three to six visits spanning a period of 3 months [23].

Blood pressure definitions. National Institute for Health and Clinical Excellence (2011) (Adapted from NICE guidance [8]. Available from http://guidance.nice.org.uk/CG127 Reproduced with permission)
The following ABPM cut-offs have been recommended by both the seventh Joint National Committee and the European Societies of Hypertension and Cardiology guidelines to diagnose hypertension [24, 25]:
-
24-h average above 135/85 mmHg
-
Daytime average above 140/90 mmHg
-
Night-time average above 125/75 mmHg
ABPM can also be used to monitor treatment response, and to clarify the diagnosis of [26]:
-
“White-coat” syndrome
-
Episodic hypertension (if suspecting a phaeochromocytoma)
-
Hypotensive symptoms with anti-hypertensive medications
-
Resistant hypertension
Systolic blood pressure readings over 180 or diastolic blood pressure readings over 110 mmHg suggest severe hypertension. In the presence of hypertensive ophthalmic changes such as retinal haemorrhage, papilloedema or exudates, or symptoms indicative of phaeochromocytoma, such as headaches, palpitations, sweating and labile blood pressure [27], this is termed “malignant” or accelerated hypertension and requires urgent treatment (within 24 h). On the other hand, in asymptomatic patients with no evidence of acute end-organ damage, the short-term risk of severe hypertension is low and there is no proven benefit of rapid in-patient blood pressure reduction [28, 29].
Based on the ABPM results (overall average blood pressure 138/87; daytime average 142/94), John was given a diagnosis of hypertension. Initial examination, blood tests and urinalysis were normal, suggesting no end-organ damage had yet occurred, but given John’s young age, his GP performed a more focussed cardiovascular examination and requested some further blood tests to identify whether this could be secondary hypertension (serum calcium, parathyroid hormone, serum lipid profile, aldosterone:renin ratio).
Determining the Cause: What to Look for and What Tests to Do
The main focus of examination is to assess for end-organ damage although a full examination also helps identify potential causes for the hypertension [30]. In most asymptomatic adults, essential hypertension remains the predominant cause for chronic high blood pressure even in the young, with secondary causes only found in less than 10 % of young adults (Fig. 11.5) [31–33]. Extensive testing in those with no risk factors or additional features is therefore not indicated or cost effective.

Essential Tests
In the majority of patients without symptoms suggestive of secondary causes, only a limited evaluation is routinely required:
-
Confirm near-equal blood pressure in left and right arms (difference of >20 mmHg in systolic blood pressure is significant)
-
Fundoscopy to assess for any hypertensive retinal changes
-
Blood tests: full blood counts, urea/electrolytes, glucose, thyroid function tests, parathyroid hormone, serum calcium level, serum lipid profile, estimated glomerular filtration rate
-
Urinalysis
-
Electrocardiogram (Fig. 11.6)
Fig. 11.6 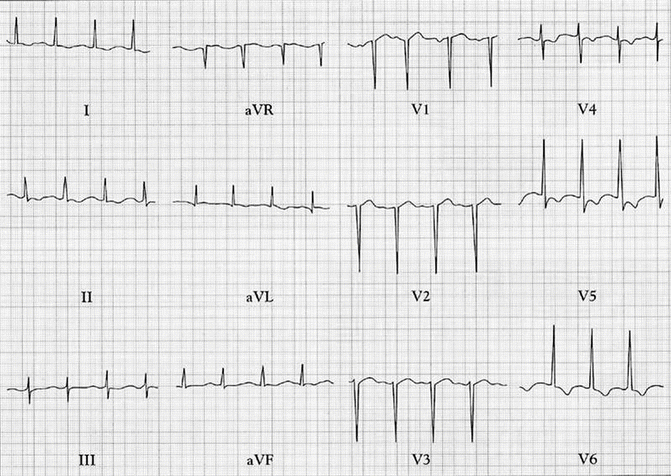
Electrocardiogram showing left ventricular hypertrophy with strain pattern (lateral ST depression)

The presence of any of the following general features would justify a work-up for secondary causes of hypertension (Table 11.1 and Fig. 11.7):

Diagnostic algorithm for the evaluation of primary and secondary hypertension. National Institute for Health and Clinical Excellence (2011) (Adapted from ‘CG 127 [8]. Available from http://guidance.nice.org.uk/CG127 Reproduced with permission)
-
Rapid onset of severe or malignant hypertension (diastolic BP >120 mmHg +/− acute end organ damage)
-
Persistently raised blood pressures (diastolic >90 mmHg) despite treatment with three or more antihypertensive agents (inclusive of diuretic use)
-
Age of onset before puberty
-
Confirmed hypertension at an age less than 30 years with no risk factors (i.e., non-black, no family history, normal BMI, normal plasma cholesterol levels) [34]
No abnormalities were discovered with further testing and a diagnosis of essential hypertension was made. John’s GP explained this diagnosis and the potential consequences to John. She then proceeded to discuss risk factors, along with reassurance that dietary and life-style modifications can be sufficient to treat mild hypertension. They also discussed the influence his stressful job may be having on his blood pressure, although the doctor reassured him that work is often indirectly related via lifestyle issues. This led on to a discussion about the adverse effects of smoking, obesity and a sedentary routine. John had recently read a newspaper article about a cure for hypertension called renal denervation and wondered if he might be eligible for this.
What are the principles with regards to treatment?
The initial treatment approach in mild to moderate uncomplicated essential hypertension is lifestyle modification [8, 35]. The key features of this are increasing daily physical activity levels, with the aim of achieving and maintaining a BMI <25. Weight loss lowers systolic blood pressure by 5–20 mmHg per 10 kg lost [36]. Dietary changes with particular attention given to increasing proportionate consumption of fruits, vegetable and low-fat dairy products, and reducing dietary sodium intake to less than 100 mmol/day, can also lead to a 10 mmHg reduction in the systolic blood pressure [37, 38]. Limiting daily alcohol consumption is also an important intervention to ensure good blood pressure control [13]. Vitamin D supplementation could be considered in those with severely reduced 25-hydroxyvitamin D levels, especially patients of South Asian origin who are especially susceptible to vitamin D deficiency [16]. This has been shown to reverse the renin-angiotensin activation that is associated with low vitamin D levels, and can thus improve blood pressure control [39].
At this early point, counselling is essential to ensure long term compliance with lifestyle and medical therapy. It is important to explain that lifestyle modifications are important even if the BP remains elevated. Equally, patients are often reassured to find that if medical therapy is required, a combination of two treatments is not a marker of “difficult hypertension” or “failed” treatments but rather a way to achieve optimal results with fewer side effects.
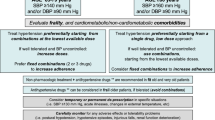
Lifestyle changes alone can be adequate to treat mild hypertension and lower overall cardiovascular risk but persistently raised blood pressures or evidence of any end-organ damage warrants pharmacological therapy (Fig. 11.8). The reduction in cardiovascular risk is directly related to the magnitude of blood pressure reduction regardless of the agent used, with the goal being to reduce the daytime blood pressure to below 140/90 mmHg (with lower targets in those with concurrent diabetes) (Fig. 11.9) [8, 40].

Updated algorithm for the diagnosis of primary hypertension. ABPM, ambulatory blood pressure monitoring; HBPM, home blood pressure monitoring. National Institute for Health and Clinical Excellence (2011) (Adapted from NICE guidelines [8]. Available from http://guidance.nice.org.uk/CG127 Reproduced with permission)

Updated algorithm for the management of primary hypertension. Adapted from [8]. National Institute for Health and Clinical Excellence (2011) (Adapted from ‘CG 127 [8]. Available from http://guidance.nice.org.uk/CG127 Reproduced with permission)
Three months later, John attended for a review with Dr Byrom. He had successfully stopped smoking, had lost several kilograms of weight and was now exercising regularly. She re-examined him for any signs of end-organ damage (fundoscopy and urinalysis) and also repeated the ABPM. The results of this showed that John had been successful in controlling his blood pressure, and his 24-h average blood pressure was 130/82. John now attends every year for a blood pressure review with the practice nurse, and is delighted to have avoided long-term pharmacological therapy.
Specialist Insight
What is the strategy for resistant cases?
Failure of the blood pressure to respond to treatment despite the use of three or more anti-hypertensive agents (inclusive of a diuretic) is known as resistant hypertension (as defined by the American Heart Association 2008 guidelines) [41]. Resistant hypertension is commonly due to:
-
Suboptimal therapy
-
Extracellular volume expansion (due to chronic kidney disease or a high-sodium diet) [42]
-
Poor compliance with medical or dietary therapy
-
“White coat” hypertension [43]
-
Ingestion of substances that can elevate the blood pressure (see below)
Patients with resistant hypertension are more likely to have an underlying cause for their hypertension, and are also at a much higher risk of developing cardiovascular complications and end-organ damage [44]. The strategy with such patients should include the following:
-
Re-evaluation for potential secondary causes of hypertension
-
Assessing for and treating end-organ damage: premature cardiovascular disease, hypertensive retinopathy, left ventricular hypertrophy, heart failure (either with normal or reduced ejection fraction), chronic kidney disease, transient ischaemic attack or stroke [45, 46].
-
Consider stopping any medications or agents that are known to increase the blood pressure such as: non-steroidal anti-inflammatory agents, selective COX-2 inhibitors, decongestants, oral contraceptives (especially oestrogen), herbal remedies (such as ginseng, ephedra), amphetamines, prednisolone, sympathomimetic diet pills, psychiatric medications (including antidepressants), liquorice, cocaine, alcohol [49].
-
ABPM (see above) to rule out co-existent ‘white coat’ hypertension.
-
Referral to a hypertension specialist service if the blood pressure remains elevated for over 6 months despite the above measures and three or more anti-hypertensive agents.
What is renal denervation?
Renal denervation is a novel therapy that may be an option for resistant hypertension. It is a percutaneous procedure that involves trans-luminal radiofrequency sympathetic denervation of the renal artery. Early case series and a randomised controlled trial demonstrated safe and significant blood pressure reductions of around 25/11 mmHg [47, 48]. However, the recent and only randomised, blinded placebo controlled study of renal denervation for hypertension (Symplicity HTN-3) failed to show any significant additional blood pressure lowering at 6 months [49]. This trial has fortunately tempered the previously unfettered enthusiasm for this intervention.
Blood pressure control is merely a surrogate for morbidity or mortality. New treatments, for hypertension, especially irreversible device-based therapies, must not just demonstrate better blood pressure control but also improved efficacy in lowering stroke or heart attack rates over current treatments before being accepted as routine. At present renal denervation is not routinely commissioned by the National Health Service (NHS) in England, ands trials with hard endpoints are currently ongoing [50, 51].
References
Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ, Comparative Risk Assessment Collaborating Group. Selected major risk factors and global and regional burden of death. Lancet. 2002;360(9343):1347–60.
Taylor BC, Wilt TJ, Welch HG. Impact of diastolic and systolic blood pressure on mortality: implications for the definition of “normal”. J Gen Intern Med. 2011;26:685.
National Statistics. Health Service for England 2010—trend tables. NHS Information Centre. 2011. Available at http://www.ic.nhs.uk/statistics-and-data-collections/health-and-lifestyles-related-surveys/health-survey-for-england/health-survey-for-england-2010-trend-tables. Accessed 1 Dec 2013.
Tu K, Chen Z, Lipscombe LL, for the Canadian Hypertension Education Program Outcomes Research Taskforce. Prevalence and incidence of hypertension from 1995 to 2005: a population-based study. CMAJ. 2008;178(11):1429–35.
Kotchen TA. Obesity-related hypertension: epidemiology, pathophysiology, and clinical management. Am J Hypertens. 2010;23(11):1170–8.
Williams B. Hypertension and “J-curve”. J Am Coll Cardiol. 2009;54:1835–6.
Krause T, Lovibond K, Caulfield M, McCormack T, Williams B. Management of hypertension: summary of NICE guidance. BMJ. 2011;343:d4891.
National Clinical Guideline Centre (NCGC). Hypertension: the clinical management of primary hypertension in adults., Clinical guideline 127. Methods, evidence and recommendations. Commissioned by the National Institute for Health and Clinical Excellence. London: NCGC; 2011.
Tirosh A, Afek A, Rudich A, Percik R, Gordon B, Ayalon N, et al. Progression of normotensive adolescents to hypertensive adults: a study of 26,980 teenagers. Hypertension. 2010;56:203–9.
Nguyen QC, Tabor JW, Entzel PP, Lau Y, Suchindran C, Hussey J, et al. Discordance in national estimates of hypertension among young adults. Epidemiology. 2011;22(4):532–41.
Gaziano TA, Bitton A, Anand S, Weinstein MC, International Society of Hypertension. The global cost of nonoptimal blood pressure. J Hypertens. 2009;27:1472–7.
Greenland P, Knoll MD, Stamler J, Naeton JD, Dyer AR, Garsdie DB, et al. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events. JAMA. 2003;290:891.
Xin X, He J, Frontini MG, Ogden LG, Motsamai OI, Whelton PK. Effects of alcohol reduction on blood pressure: a meta-analysis of randomized controlled trials. Hypertension. 2001;38:1112.
Meng L, Chen D, Yang Y, Zheng Y, Hui R. Depression increases the risk of hypertension incidence: a meta-analysis of prospective cohort studies. J Hypertens. 2012;30:842.
Yan LL, Liu K, Matthews KA, Daviglus ML, Freeman T, Kiefe C. Psychosocial factors and risk of hypertension: the Coronary Artery Risk Development in Young Adults (CARDIA) study. JAMA. 2003;290:2138.
Burgaz A, Orsini N, Larsson SC, Wolk A. Blood 25-hydroxyvitamin D concentration and hypertension: a meta-analysis. J Hypertens. 2011;29:636.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(1903):1913. Erratum in Lancet 2003 Mar 22;361(9362):1060.
Chrysant SG. Current status of aggressive blood pressure control. World J Cardiol. 2011;3(3):65–71.
Cushman WC, Evans GW, Byington RP, Goff Jr DC, Grimm Jr RH, Cutler JA, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362:1575–85.
Moreno G, Mangione CM. Management of cardiovascular disease risk factors in older adults with type 2 diabetes mellitus: 2002–2012 literature review. J Am Geriatr Soc. 2013;61(11):2027–37.
Uhlig K, Patel K, Ip S, Kitsios GD, Balk EM. Self-measured blood pressure monitoring in the management of hypertension: a systematic review and meta-analysis. Ann Intern Med. 2013;159:185.
Parati G, Stergiou GS, Asmar R, Bilo G, de Leeuw P, Imai Y, et al. European Society of Hypertension practice guidelines for home blood pressure monitoring. J Hum Hypertens. 2010;24:779.
O’Brien E, Asmar R, Beilin L, Imai Y, Mancia G, Mengden T, et al. Practice guidelines of the European Society of Hypertension for clinic, ambulatory and self blood pressure measurement. J Hypertens. 2005;23:697.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560.
Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, et al. ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7):1281–357.
de la Sierra A, Segura J, Banegas JR, Gorostidi M, de la Cruz JJ, Armario P, et al. Clinical features of 8295 patients with resistant hypertension classified on the basis of ambulatory blood pressure monitoring. Hypertension. 2011;57:898.
Zuber SM, Kantorovich V, Pacak K. Hypertension in pheochromocytoma: characteristics and treatment. Endocrinol Metab Clin North Am. 2011;40(2):295–311.
Ahmed ME, Walker JM, Beevers DG, Beevers M. Lack of difference between malignant and accelerated hypertension. Br Med J (Clin Res Ed). 1986;292:235.
Shantsila A, Shantsila E, Lip GY. Malignant hypertension: a rare problem or is it underdiagnosed? Curr Vasc Pharmacol. 2010;8(6):775–9.
Severe symptomless hypertension. Lancet. 1989;9(2):1369–70.
Yoon EY, Cohn L, Freed G, Rocchini A, Kershaw D, Ascione F, et al. Use of antihypertensive medications and diagnostic tests among privately insured adolescents and young adults with primary versus secondary hypertension. J Adolesc Health. 2014; pii:S1054-139X(13)00800-8.
Rimoldi SF, Scherrer U, Messerli FH. Secondary arterial hypertension: when, who, and how to screen? Eur Heart J. 2013. doi:10.1093/eurheartj/eht534.
Omura M, Saito J, Yamaguchi K, Kakuta Y, Nishikawa T. Prospective study on the prevalence of secondary hypertension among hypertensive patients visiting a general outpatient clinic in Japan. Hypertens Res. 2004;27(3):193–202.
Lurbe E, Torro I, Alvarez V, Nawrot T, Paya R, Redon J, et al. Prevalence, persistence, and clinical significance of masked hypertension in youth. Hypertension. 2005;45:493.
Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293–300.
Mosso L, Carvajal C, Gonzalez A, Barraza A, Avila F, Montero J, et al. Primary aldosteronism and hypertensive disease. Hypertension. 2003;42(2):161–5.
Novick AC, Zaki S, Goldfarb D, Hodge EE. Epidemiologic and clinical comparison of renal artery stenosis in black patients and white patients. J Vasc Surg. 1994;20:1.
Garovic VD, Textor SC. Renovascular hypertension and ischemic nephropathy. Circulation. 2005;112:1362–74.
Textor SC, Lerman L. Renovascular hypertension and ischemic nephropathy. Am J Hypertens. 2010;23:1159.
Betensky BP, Jaeger JR, Woo EY. Unequal blood pressures: a manifestation of subclavian steal. Am J Med. 2011;124:e1.
Streeten DH, Anderson Jr GH, Howland T, Chiang R, Smulyan H. Effects of thyroid function on blood pressure. Recognition of hypothyroid hypertension. Hypertension. 1988;11:78.
Kanbay M, Isik B, Akcay A, Ozkara A, Karakurt F, Turgut F, et al. Relation between serum calcium, phosphate, parathyroid hormone and ‘nondipper’ circadian blood pressure variability profile in patients with normal renal function. Am J Nephrol. 2007;27:516.
Eisenhofer G, Lenders JW, Goldstein DS, Mannelli M, Csako G, Walther MM, et al. Pheochromocytoma catecholamine phenotypes and prediction of tumor size and location by use of plasma free metanephrines. Clin Chem. 2005;51:735–44.
Somers VK, White DP, Amin R, Abraham WT, Costa F, Culebras A, et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. J Am Coll Cardiol. 2008;52:686.
Saruta T, Suzuki H, Handa M, Igarashi Y, Kondo K, Senba S. Multiple factors contribute to the pathogenesis of hypertension in Cushing’s syndrome. J Clin Endocrinol Metab. 1986;62:275.
Mancini T, Kola B, Mantero F, Boscaro M, Arnaldi G. High cardiovascular risk in patients with Cushing’s syndrome according to 1999 WHO/ISH guidelines. Clin Endocrinol (Oxf). 2004;61:768.
Elmer PJ, Obarzanek E, Vollmer WM, Simons-Morton D, Stevens VJ, Young DR, et al. Effects of comprehensive lifestyle modification on diet, weight, physical fitness, and blood pressure control: 18-month results of a randomized trial. Ann Intern Med. 2006;144:485.
Carnethon MR, Evans NS, Church TS, Lewis CE, Schreiner PJ, Jacobs Jr DR. Joint associations of physical activity and aerobic fitness on the development of incident hypertension: coronary artery risk development in young adults. Hypertension. 2010;56:49.
Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, et al.; DASH-Sodium Collaborative Research Group. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med. 2001;344(1):3–10.
Forman JP, Stampfer MJ, Curhan GC. Diet and lifestyle risk factors associated with incident hypertension in women. JAMA. 2009;302:401.
Schroten NF, Ruifrok WP, Kleijn L, Dokter MM, Silljé HH, Lambers Heerspink HJ, et al. Short-term vitamin D3 supplementation lowers plasma renin activity in patients with stable chronic heart failure: an open-label, blinded end point, randomized prospective trial (VitD-CHF trial). Am Heart J. 2013;166(2):357–64.
Blood Pressure Lowering Treatment Trialists’ Collaboration, Turnbull F, Neal B, Ninomiya T, Algert C, Arima H, et al. Effects of different regimens to lower blood pressure on major cardiovascular events in older and younger adults: meta-analysis of randomised trials. BMJ. 2008;336:112.
Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation. 2008;117:e510.
Pimenta E, Gaddam KK, Oparil S, Aban I, Husain S, Dell’Italia LJ, et al. Effects of dietary sodium restriction on blood pressure in subjects with resistant hypertension: results from a randomized trial. Hypertension. 2009;54:444–6.
Verdecchia P, Reboldi GP, Angeli F, Schillaci G, Schwartz JE, Pickering TG, et al. Short- and long-term incidence of stroke in white-coat hypertension. Hypertension. 2005;45:203.
Faselis C, Doumas M, Papademetriou V. Common secondary causes of resistant hypertension and rational for treatment. Int J Hypertens. 2011;2011:236239.
Sipahi I, Tuzcu EM, Schoenhagen P, Wolski KE, Nicholls SJ, Balog C, et al. Effects of normal, pre-hypertensive, and hypertensive blood pressure levels on progression of coronary atherosclerosis. J Am Coll Cardiol. 2006;48:833.
Asayama K, Ohkubo T, Kikuya M, Metoki H, Hoshi H, Hashimoto J, et al. Prediction of stroke by self-measurement of blood pressure at home versus casual screening blood pressure measurement in relation to the Joint National Committee 7 classification: the Ohasama study. Stroke. 2004;35:2356.
Symplicity HTN-1 Investigators. Catheter-based renal sympathetic denervation for resistant hypertension: durability of blood pressure reduction out to 24 months. Hypertension. 2011;57(5):911–7.
Symplicity HTN-2 Investigators. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010;376:1903–9.
Medtronic announces US renal denervation pivotal trial fails to meet primary efficacy endpoint while meeting primary safety end point [press release]. 9 Jan 2014.
Sapoval M; Assistance Publique – Hôpitaux de Paris. Renal Denervation in Hypertension (DENER-HTN). In: ClinicalTrials.gov[Internet]. Bethesda: National Library of Medicine (US). 2000-[cited 22 Feb 2014]. Available from: http://clinicaltrials.gov/show/NCT01570777; NLM Identifier NCT01570777.
Schlaich M, Baker IDI Heart and Diabetes Institute. Renal Denervation for Resistant Hypertension (RDNP-2012-01). In: ClinicalTrials.gov[Internet]. Bethesda: National Library of Medicine (US). 2000-[cited 10 Mar 2014]. Available from: http://clinicaltrials.gov/show/NCT01865240; NLM Identifier NCT01865240
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag London
About this chapter
Cite this chapter
Witte, K.K., Jamil, H.A. (2015). Hypertension in the Young Adult. In: Ajjan, R., Orme, S. (eds) Endocrinology and Diabetes. Springer, London. https://doi.org/10.1007/978-1-4471-2789-5_11
Download citation
DOI: https://doi.org/10.1007/978-1-4471-2789-5_11
Publisher Name: Springer, London
Print ISBN: 978-1-4471-2788-8
Online ISBN: 978-1-4471-2789-5
eBook Packages: MedicineMedicine (R0)