
Abstract

HIV Attachment. In this cross section, HIV is shown at the top and a target cell is shown at the bottom in blues. HIV envelope protein (A) has bound to the receptor CD4 (B) and then to coreceptor CCR5 (C), causing a change in conformation that inserts fusion peptides into the cellular membrane
Antiretroviral therapy changed the face of HIV/AIDS from that of soon and certain death to that of a chronic disease in the years following introduction of highly active antiretroviral therapy in 1995–1996 (initially termed HAART, but now most often abbreviated to ART since not all combinations of regimens are equally active). Since then, many new agents have been developed and introduced in response to problems of resistance, toxicity, and tolerability, and great advances have been achieved in accessibility of HIV drugs in resource-poor global regions. Potential challenges that providers of HIV therapy will face in the coming decade include continuing problems with resistance, especially where access to drugs is inconsistent, determining how best to combine new and existing agents, defining the role of preventive treatment (pre-exposure prophylaxis or PrEP), and evaluating the potential of strategies for cure in some populations.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Human Immunodeficiency Virus
- Human Immunodeficiency Virus Infection
- Virological Failure
- Human Immunodeficiency Virus Disease
- Human Immunodeficiency Virus Replication
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
The progress in chemotherapy of human immunodeficiency virus infection (HIV) ranks as one of the great success stories of infectious disease. Advances in treatment over the past 25 years have accompanied milestones in our understanding of the virology and immunopathogenesis of disease, reflect triumphs of rational drug design, and encompass a plethora of findings from careful and comprehensive clinical research. Where it is available, highly active antiretroviral therapy (ART) has dramatically lowered mortality not only from HIV disease, but from all causes, especially cardiovascular disease, as well. While the convenience, efficacy, and toxicity of antiviral therapy have improved remarkably from the era of early treatment, when lactic acidosis, lipodystrophy, and severe neuropathy were accepted as regrettable trade-offs of survival, acquired antiviral resistance persists, increasing primary HIV antiviral drug resistance has emerged. Furthermore, the development of resistance in areas where drug access is limited present a growing problem. In addition, the cross-resistance of many drugs within classes, adverse pharmacologic interactions between antiretroviral agents and other antiretrovirals as well as drugs commonly used for other medical conditions can still quickly make acceptable choices for regimens difficult.
This chapter aims to present a brief look at the current armamentarium, give some insight into current clinical problems and treatment strategies, and highlight areas where advances in activity and pharmacologic profile are needed.
2 The Medicine Cabinet—Current Antiretroviral Drugs
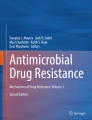
Background and Introduction: The number of pharmaceuticals approved for the treatment of AIDS and HIV infection in the United States grew from one (zidovudine, AZT) in 1987 to include thirty individual agents and eight fixed-dose combination tablets by 2014 (some no longer available, some additional combination agents are available abroad—see Fig. 1). Many approved medications were discovered via high-throughput screening efforts, while others were developed principally through rational drug design based on structural biology. The latter approach has proven particularly effective in developing second- and third-generation drugs in several different classes, which can be used against virus resistant to earlier, similar drugs.

Time line for approval of antivirals in the United States. Time from left to right from 1997 to 2014 (red bar). Combination tablets including single-tablet combination regimens are shown at the top, cyan background. NRTI, NNRTI, PI, entry inhibitors, and INSTIs are shown below the time line in alternating beige and cyan background. Vertical lines for each drug represent quarter of year of approval [data from 17, archival guidelines, and multiple other sources]
Approved antiretroviral drugs for HIV still target only four viral and one host protein (see Fig. 1): Nucleoside (zidovudine—AZT, didanosine—ddI, zalcitabine—ddC is no longer available, stavudine—D4T, lamivudine—3TC, and abacavir—ABC) and nucleotide (tenofovir, TDF) reverse transcriptase (RT) inhibitors act both as competitive inhibitors and chain terminators within the active site of the HIV viral RNA-dependent DNA polymerase, blocking efficient synthesis of proviral DNA. Non-nucleoside reverse transcriptase inhibitors (nevirapine—NVP, efavirenz—EFV, etravirine—ETV, rilpivirine—RPV) bind to site(s) outside the catalytic active site producing structural changes in the enzyme that render it incapable of normal function. Approved protease inhibitors (saquinavir—SQV, indinavir—IDV, nelfinavir—NFV, fosamprenavir—FPV, lopinavir—LPV, tipranavir—TPV, atazanavir—ATV, and darunavir—DRV) are all derivatives of structural analogs of the natural enzyme cleavage site and function as potent competitive inhibitors. Enfuvirtide (FuzeonTM, T20), an injectable peptide drug, binds to the transmembrane portion of the HIV envelope protein (TM, gp41), stabilizing the conformation, preventing infection by blocking a structural change needed for entry of virus into CD4+ cells. Integrase inhibitors (raltegravir—RAL, elvitegravir—ETG, and dolutegravir—DTG) block the strand transfer function of HIV-1 integrase, preventing integration of the reversed-transcribed provirus into host genomic DNA, resulting in abortive, if any, viral transcription. A drug targeting one of the two most common cell-surface coreceptor molecules used by HIV (CCR5), maraviroc (MVC), is also in clinical use.
Each class of antiretroviral drug is very briefly reviewed below, mechanism(s) of action explained in more detail, and some prominent pharmacokinetic characteristics and adverse effects are noted.
Currently Approved Reverse Transcriptase Inhibitors: These include seven nucleoside/nucleotide analogs (NRTIs) and five non-nucleoside inhibitors (NNRTIs) of HIV-1 RT (see Fig. 1 and following). Three agents in this class were introduced but are no longer available and/or recommended due to toxicity (ddC, zalcitabine, HividTM) and pharmacokinetics (delavirdine, DLV, RescriptorTM—no longer marketed by Agouron but revived by ViiV, and non-enteric coated ddI—Videx).
Nucleoside Reverse Transcriptase Inhibitors (NRTIs). Stemming from work in the 1960s and 1970s, modified dideoxynucleotides similar in structure to NRTIs were studied as DNA chain terminators for use in cancer therapy (Toji and Cohen 1969; Yatchoan and Broder 1987), including screening for antineoplastic activity. AZT, the first approved antiretroviral agent, is still in use and serves as an example. The structure of AZT differs from deoxythymidine in the presence of a 3′ azido rather than a 3′ hydroxy group. Activity requires intracellular phosphorylation at the 5′ position by thymidine kinase to form AZT-5′-monophosphate, phosphorylation to AZT-5′-diphosphate by thymidylate kinase, and conversion to AZT-5′-triphosphate (AZT-TP) by nucleoside diphosphate kinase. AZT-TP is a substrate for viral RT (and to a lesser degree host enzymes), but the azido group at the 3′ position of AZT does not allow further 5′–3′ phosphodiester linkages to form. AZT competes with thymidine for access to the active site of reverse transcriptase and prematurely terminates chain elongation once incorporated into the DNA strand (Yatchoan and Broder 1987; Furman et al. 1986; St Clair et al. 1987). While AZT and other NRTI agents have a greater affinity for reverse transcriptase than cellular DNA polymerases alpha, beta, or epsilon, mitochondrial DNA polymerase is susceptible to varying degrees, and incorporation of AZT into germ-line DNA and vertical transmission of modified DNA has been noted (see toxicity) (Yatchoan and Broder 1987; St Clair et al. 1987).
Each NRTI is an analog of a DNA nucleoside or nucleotide, including structural analogs of thymidine (zidovudine—AZT, stavudine—D4T), cytosine (lamivudine—3TC, emtricitabine—FTC), guanine (abacavir—ABC), and adenosine (didansosine—DDI, tenofovir—TDF). Tenofovir is the only currently approved nucleotide (monophosphate) NRTI.
The NRTI antiretrovirals have only few metabolic interactions of importance. Though abacavir is a substrate for both alcohol dehydrogenase and uracil transferase enzymes, no dosage adjustment is required. Lamivudine, emtricitabine, and tenofovir require dosage reduction in renal insufficiency. Tenofovir also reduces exposure to atazanavir by mechanism(s) that remain unelucidated, and tenofovir also has an important interaction with ledipasvir, a new hepatitis C NS5A inhibitor (Rockstroh 2015).
Non-nucleoside Reverse Transcriptase Inhibitors (NNRTIs). Approved NNRTI antiretrovirals in the United States include nevirapine (NVP), delavirdine (DLV), efavirenz (EFV), etravirine (ETV), and rilpivirine (RPV). Unlike NRTIs, non-nucleoside reverse transcriptase inhibitors (NNRTIs) are not structural homologues of DNA nucleotides, rather binding reverse transcriptase at an allosteric site ~10 Å distant from the catalytic site. Binding induces conformational changes, which alters substrate binding and affects translocation of double-stranded DNA. NNRTIs are non-competitive inhibitors of the reverse transcriptase enzyme (Mao et al. 2000; Crauwels et al. 2012; Kohlstaedt et al. 1992; Pollard et al. 1998; Smerdon et al. 1994). Currently, there are five NNRTIs available in the United States for the treatment of HIV infection (Fig. 1). Just as for the NRTI class of antiretroviral agents, the NNRTIs have also been associated with significant toxicity. As a class, all agents share the potential for causing cutaneous reactions, sometimes severe ones.
Metabolism of all NNRTI drugs processed largely through CYP3A4, and all but rilpivirine induces their own metabolism (Crauwels et al. 2012). Efavirenz and nevirapine are metabolized and induced by CYP2B6, and etravirine is metabolized and inhibited by CYP2C9 and CYP2C19 (see Table 1).
Entry (attachment and fusion) Inhibitors. The first entry and only approved fusion inhibitor is Fuzeon (Loutfy et al. 2007), approved in 2003 for use in the United States. A number of additional entry inhibitors have been evaluated in clinical and preclinical trials, including enhanced peptide-based fusion inhibitors (T-1249), and antagonists of envelope binding to the CXCR4 co-receptor (most are toxic), the CD4 receptor, and cell-surface galactosyl ceramide. Monoclonal antibodies that interfere with entry have also been explored. However, the only other entry inhibitor approved at the time of this writing is maraviroc®, a small molecule that targets the CCR5 coreceptor molecule. Maraviroc (MVC) (Dorr et al. 2005) is metabolized primarily by CYP3A4, is also a substrate for the P-glycoprotein efflux pump, and requires dosage adjustment with protease inhibitors and/or NNRTI drugs given in combination.
Protease Inhibitors: HIV protease is a virally encoded aspartyl protease that prefers phenylalanine–proline or tyrosine–proline containing substrates. Two 65-Kd pol precursor polyproteins must first interact to form an active dimer which then self-cleaves and acts to cleave other individual proteins (e.g., matrix and capsid proteins, reverse transcriptase and integrase proteins) from gag and pol polyprotein precursors. The mature protease has two identical 99 amino acid monomers arranged in a donut-like homodimer. Protease inhibitors are competitive inhibitors of catalyzed cleavage that have high affinity for the preferred peptide substrate cleavage site. Protease inhibitors (PIs) do not block infection by viral particles produced in the absence of PI, but in the presence of PI only non-infectious and immature (the core never condenses as the capsid protein is never cleaved) viral particles are produced (Merrett 1990).
The crystal structure of the HIV protease was first determined by X-ray diffraction in 1988 (Merrett 1990). Protease inhibitors are essential analogs of phenylalanine-proline that competitively inhibits the enzyme because of chemical affinity for the active site. Drug resistance is primarily mediated by mutations resulting in subsequent amino acid substitutions both near and distant (producing conformational changes) to the active site, which affects drug-binding affinity. In addition, compensatory mutations in the gag polyprotein which introduce more favored or altered cleavage may allow proteases otherwise impaired by changes needed to escape PI inhibition to function more effectively.
In vitro activity of early peptide analogs was documented as early as 1990, and by 1993 candidate drugs were entering human trials, and the first protease inhibitor, saquinavir (SQV, Invirase) was approved for use in the United States, in 1995, followed by ritonavir (RTV) and indinavir (IDV) in the next year, and by nelfinavir (NFV), amprenavir (APV), lopinavir/ritonavir combination (LPV/r) atazanavir (ATV), fosamprenavir (FPV), tipranavir (TPV), and darunavir (DRV) over the next decade (see Fig. 1).
Pharmacokinetics of Protease Inhibitors. Each agent is available exclusively in oral dosage form though absorption may be limited. One strategy included use of presolubilized soft gel capsules for absorption (RTV, APV, LPV/RTV, Fortovase soft gel capsules) and addition of agents such as vitamin E (APV). Many of these have been supplanted (LPV/RTV available in tablet and solution, RTV available in capsule and tablet, ATV, TPV, SQV, and IDV capsules) and/or withdrawn from the market (unmodified Amprenavir, Fortovase). Distribution throughout the body varies, but while CSF penetration tends to be low (CSF usually averages ~4 % of serum concentration), this is still within the active range. All share metabolism via the P-450 mixed function oxidase system, including primarily CYP3A (see Table 2). Various protease inhibitors also inhibit and/or induce cytochrome oxidases, conjugation, and membrane transport proteins, leading to many drug interactions with other medications. These can be troublesome, but are also sometimes useful pharmacokinetic interactions, as between ritonavir (and now cobicistat), which is co-administered to prolong the half-life and area under the curve (AUC—i.e., cumulative drug exposure, a product of concentration over time) of all currently used protease inhibitors except nelfinavir (see Table 2) (Fellay et al. 2002; Kim 2003).
Integrase Inhibitors: HIV-1 integrase is a multifunctional enzyme that catalyzes the insertion of reverse transcribed viral DNA into the host genome. Integrase removes the two terminal 3′ nucleotides from the 5′ U3 and 3′ U5 LTR ends of linear viral DNA (3′–5′ exonuclease), makes a 5 bp staggered cut in host double-stranded DNA (endonuclease), and mediates strand transfer between the processed viral and cleaved genomic DNA (ligase) (Craigie 2001). Theoretically, disruption of any step in the integration process should efficiently inhibit viral replication, but all currently approved medications in this class are integrase strand transfer inhibitors (INSTIs), including raltegravir (RAL), elvitegravir (EVG), and dolutegravir (DTG). While initially often used in patients resistant to other classes of antiretrovirals, INSTIs are increasingly being used in first-line regimens given their potency and favorable side-effect profiles. In addition, for reasons that remain incompletely understood, INSTIs suppress HIV replication in the blood more quickly than any other class of antiretrovirals.
3 Current Treatment—Who, What, When, Why, and How
Who to treat and why: Over the last twenty-five years, the goals of antiretroviral therapy have evolved from the desperate attempt to prolong the duration and quality of life in critically ill AIDS patients with limited tools (Fischl et al. 1987; Cooper et al. 1993). Currently, there are multiple objectives (Department of Health and Human Services 2014) influencing treatment of HIV-infected individuals: (1) To achieve durable suppression and immune reconstitution, avoiding “AIDS-related” infections and other complications, treating HIV as a chronic disease that must be controlled, not unlike diabetes or hypertension; (2) To reduce all-cause morbidity and mortality, most notably by reducing inflammation and thereby improving cardiovascular and neoplastic co-morbidity (Kuller et al. 2008; Sandler et al. 2011; Duprez et al. 2012; Borges et al. 2013; Smith 2010; Sabin et al. 2008; Bedimo et al. 2009; Shiels et al. 2011; Worm et al. 2013); (3) To prevent transmission of HIV, “test to treat” strategies (Nachega et al. 2014; Kretzschmar et al. 2013; Kulkarni et al. 2013; DeGruttola et al. 2010) can ultimately lower the prevalence of disease; (4) There is evidence that HIV treatment is helpful in reducing the otherwise accelerated progression of hepatitis C infection in co-infected individuals and also may aid HCV treatment; and finally (5) To effectively cure HIV infection, while not yet possible, early treatment can reduce viral set point and “total body burden,” which may be critical factors in the success of new modalities which emerge to produce potential eradication of infection (Department of Health and Human Services 2014).
These goals are reflected in the changes in the Department of Health and Human Services (DHHS) guidelines over the years (Table 3). From 1998 to 2003, treatment was largely recommended to prevent complications arising directly from HIV disease. Only in 2004 had sufficient evidence accumulated that treatment of individuals before critical immunological depletion (i.e., before CD4 of <350/mm3) with high viral loads (>100,000 copies/ml) was recommended for consideration for treatment. From 2007 to 2011, guidelines urged consideration of therapy in asymptomatic individuals with higher CD4 cells, but with delayed therapy acceptable in those with >350 or >500 T cells. Since 2012, antiretroviral therapy (ART) has been recommended in all individuals (see Table 3) (Department of Health and Human Services 2014).
With What & How—General Principals of Therapy: The DHHS guidelines on antiretroviral are properly based on validated clinical trial data and experience, but that does not obviate the potential usefulness of models that might predict superior activity and/or better combinations for clinical exploration beyond what can be deduced by pharmacokinetic data and in vitro antiviral activity studies. Historically, there have been interesting and at times contrasting theories and interpretations. For example, AZT was initially given every 4 h based on plasma levels, but studies of intracellular concentrations later showed this to be unnecessary, and it is now often given only twice daily (Fletcher et al. 1998). Similarly, in the early 1990s “convergent therapy” with three nucleotides targeting the reverse transcriptase was predicted on the basis of in vitro modeling to create a genetic barrier to which the virus would be unable to surmount with resistance mutations (Chow et al. 1993), then quickly derided and the paradigm that multiple enzymes would needed to be targeted when ABC+AZT+3TC (triple NRTI) failed in trials (Emini et al. 1993), and revised again to reflect two mechanisms of action (though perhaps on the same enzyme) when Atripla (NNRTI + two NRTI) became a successful mainstay of therapy.
From 1995 until the introduction of the integrase strand inhibitors, only protease inhibitors and non-nucleoside reverse transcriptase inhibitors were felt to be potent enough to form the backbone of successful antiretroviral regimens, but these two differed very widely in barrier to resistance, and the reason and nature of the greater potency remained unexplained, particularly as the in vitro IC50 values did not differentiate PIs and NNRTIs from NRTIs. From 2011 to 2014, a “critical subset” model, postulating that multiple copies of a drug target must remain active to allow replication to progress, was found to correlate with steeper dose-response curves for NNRTI and PI antiretrovirals (Shen et al. 2011; Jilek et al. 2012; Laskey and Siliciano 2014). While both NRTIs and INSTIs exhibit flatter curves, the integrase inhibitors, most potent of all the antiretrovirals, are not subject to this model (i.e., inhibition of even one site prevents replication), at least possibly explaining the lower effectiveness of NRTIs compared to these other drugs.
Some hard and soft “don’ts.” Some clinicians feel uncomfortable using an NNRTI regimen (especially rilpivirine) in those with very high viral loads (>100,000 copies/ml) or where concern for resistance is high. (Rimsky et al. 2012; Pozniak et al. 2010). The concomitant use of tenofovir and abacavir should be avoided, as the risk of virological failure is significant (Gilliam et al. 2007). Most clinicians would not add or change a single agent in a regimen with overt virological failure (HIV RNA rising and/or >5000 copies/ml), but addition of single agents as “consolidation therapy” for patients achieving a significant antiviral response falling short of complete suppression is not uncommon, but should be guided by resistance testing where feasible. Avoidance of agents with additive or synergistic toxicities (e.g., d4T and ddI), adverse intracellular interactions (e.g., AZT and d4T or 3TC and ddC), and adverse pharmacokinetics (e.g., saquinavir and efavirenz) is another general principal of therapy.
Treatment of antiretroviral-experienced individuals who have undergone failures of one or more regimens must be guided by genotypic and/or phenotypic resistance testing (see “Technologies for Monitoring and Guiding Treatment,” following) assessment of adherence (e.g., review of prescription refill data), careful consideration of absorption limiting drug-drug or drug/disease interactions, possibly approached by therapeutic drug monitoring, review of prior treatment (“archived” resistant variants may escape detection by conventional resistance testing), availability of agents of classes not previously included in the patient’s treatment history (e.g., INSTIs, NNRTIs, Fuzeon), and the patient’s potential for tolerating additional or different drugs (Montaner et al. 2001; Youle et al. 2002; Lalezari et al. 2003; Lazzarin et al. 2003).
Historical Notes. The manner in which we treat patients infected with HIV has undergone remarkable changes. Zidovudine monotherapy was the only option available from 1997 to 1991 (see Fig. 1). By the time didanosine was approved in 1991, many individuals who had experienced a transient response from zidovudine were simply switched to didanosine, and later to zalcitabine (1992) or stavudine (1994) as these new drugs became available. Sequential monotherapy was associated with greater survival than continued zidovudine or cessation of therapy (Graham et al. 1996), but HIV variants with multiple drug resistance mutations predictably accumulated (Iversen et al. 1996).
Combination therapy produced greater and more sustained response (Iversen et al. 1996; Meng et al. 1992; Collier et al. 1993; Schooley et al. 1996; Gulick et al. 1997; Johnson and Sax 2014) and has improved with the introduction of less toxic and better tolerated therapies. With the introduction of protease inhibitors saquinavir, ritonavir, and indinavir in combination with NRTIs in 1995 and 1996 (Gulick et al. 1997), highly active antiretroviral therapy (HAART) produced profound and durable suppression of HIV in the plasma, with marked reductions in mortality, becoming the standard of care by 1998 (Table 3). The subsequent introduction of additional abacavir and tenofovir, additional protease inhibitors and NNRTIs (NVP, EFV, ETV, RPV) have led to regimens with increased efficacy and reduced toxicity (Fig. 1). Subsequent second-generation PIs (TPV, DRV) and introduction of INSTIs (RAL, ELG, DTG) allowed formulation of regimens that were more potent, and both less toxic for initial therapy while also being active against many resistant strains (Johnson and Sax 2014).
Technologies for Monitoring and Guiding Treatment. Assays to quantify HIV replication (Ho et al. 1995; Saag et al. 1996) established the relationship between HIV RNA viral load and the risk of disease progression and death (Mellors et al. 1997). Elaboration of the kinetics of HIV replication (Perelson et al. 1996) facilitated more clinical trials by allowing rapid comparison of regimens using “surrogate” (i.e., non-clinical) endpoints, as well as expediting early identification of successful and failing therapy in clinical practice. Most recently droplet digital PCR (Strain et al. 2013) has provided the ability to quantify very low viral loads consistently, allowing an approach for a clinical definition of strategies for cure (see following).
HIV resistance testing (Tang and Shafer 2012) has also undergone considerable evolution in sophistication over the years. Routine use of genotyping using conventional capillary sequencing of the reverse transcriptase and protease in genomic HIV RNA present in plasma virions followed viral load monitoring by only a few years, allowing prediction of prevalent populations of virus bearing resistance mutations (Shafer 2002). Phenotyping has involved cloning portions or all of the pol genes derived by RT-PCR from plasma virus into a reference reporter clone expressing luciferase, transfecting recombinant virus and measuring virus infection in the presence of increasing concentrations of drug (Richman 2000), which is very analogous to conventional antimicrobial sensitivity testing. The availability of large databanks of virus for which both phenotypic and genotypic resistance data allowed the introduction of “virtual phenotyping,” to more accurately predict resistance from sequence data (Larder et al. 2000; Hertogs et al. 2000). A number of allele-specific PCR-based assays capable of detecting minor populations of resistant virus (esp. NNRTIs) have become available, and some have found their way into potential point of care devices (Paredes et al. 2007; Palmer et al. 2006; Hunt et al. 2014). Finally, next-generation sequencing of the entire polymerase or even the complete viral genome is beginning to be used to better predict the success of possible therapeutic regimens (Hunt et al. 2014; Garcia-Diaz et al. 2014; Simen et al. 2014). Clinical studies have indicated better short- and long-term outcomes in clinical settings when clinicians are provided with the results of testing (Cingolani et al. 2002; Clevenbergh et al. 2000; Baxter et al. 2000; Tural et al. 2002), especially when expert advice in interpretation is also provided (Baxter et al. 2000; Tural et al. 2002). Current guidelines suggest that resistance testing should be obtained in cases of virological failure, incomplete suppression, prior to initiation of antiretroviral therapy, and in acute HIV infection, due to increasing transmission of drug-resistant strains during primary infection (Little et al. 2002), which is especially relevant in resource-poor settings where monitoring and availability of antiretrovirals may be intermittent (Hamers et al. 2013).
Barriers to Treatment: Include identifying those with HIV infection, providing access to treatment, and maintaining patients in care on therapy, termed the continuum of HIV care, as well as problems of adherence, toxicity, and resistance.
Access and the Continuum of HIV care. Clearly access is an overriding while clearly surmountable hurdle for treatment. It is estimated that 1.3 million individuals in the United States are infected with HIV of whom only 400,000 are in care and only 200,000 are suppressed on treatment (CDC 2011). Worldwide, nearly 35 million individuals are estimated to be infected with HIV, with 2 million newly infected in 2013, while only 12.9 million have access to antiretrovirals, and a smaller number still are suppressed (World Health Organization 2014). Progress, however, has been made: Nearly 67 % of HIV+ pregnant women receive prophylactic treatment, and over 2 million people were started on antiretrovirals worldwide (World Health Organization 2014).
Adherence and Tolerability. As noted above, many earlier drugs were quite toxic, frequently producing “minor” issues of nausea, diarrhea, rash, and other symptoms. In addition, the pill burden of earlier antiretroviral regimens was staggering—a patient requiring amprenavir, didanosine, and lamivudine in the late nineties could look forward to eighteen tablets and capsules of antiretrovirals a day at staggered times four times daily. With the introduction of Epzicom (ABC+3TC) and Truvada (TDF+FTC) in 2004 and the routine use of boosted protease inhibitors such as ATV/r and later DRV/r, regimens containing 2–4 doses once daily became common. Finally, with the introduction of Atripla (EFV+TDF+FTC) in 2006, and subsequently Complera (RPV+TDF+FTC), Stribild (EGV+Cobi+TDF+FTC), and most recently Triumeq (DTG+ABC+3TC), a single-pill, highly potent, fixed-dose regimens have assumed the preferred position in recommended therapy and become goals of future drug development (see Fig. 1). New combination tablets that will likely be available by the time this review appears include atazanavir/cobicistat, darunavir/cobicistat, elvitegravir/cobicistat, and elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide (United States Food and Drug Administration 2014).
Adherence is also a critical factor in the success or failure of antiretroviral therapy with a direct relationship to pharmacokinetics of available drugs. Studies indicate that lower than 95 % adherence—one missed dose in a twice daily regimen once every ten days—may lower the success rate by up to 20 % (Paterson et al. 2000; Knobel et al. 1998). Promotion of adherence by reducing pill burden, decreasing frequency of administration, establishing a rapport with the patient, and involving the patient in treatment decisions, proper pharmacy instruction and monitoring, and provision of pill boxes or other organizers, electronic reminders, or phone calls have all been explored (Chesney 2003).
Toxicity and Metabolic Effects. The newer antiretroviral regimens avoid many but not all of these problems, but the legacy of prior use of more toxic antiretrovirals and combinations remains in the clinic today. Mitochondrial effects have been minimized by largely restricting NRTI use to tenofovir, abacavir, lamivudine, and emtricitabine. These are the least potent inhibitors of mitochondrial DNA-dependent DNA polymerase gamma. Prolonged treatment otherwise results in depletion of mitochondrial DNA and loss of mitochondria, leading in the extreme to lactic acidosis (Feng et al. 2001; Arenas-Pinto et al. 2003), pancreatitis, hepatitis, and muscle weakness (Boubaker et al. 2001; Coghlan et al. 2001). Individual “bad” NRTIs manifested different patterns of toxicity, AZT characteristically causing myopathy (Arnaudo et al. 1991), while ddI (particularly when used with d4T) was associated with pancreatitis (Moore et al. 2001; Scribner et al. 2000). The same “D” drugs (d4T, ddI) were strongly implicated in avascular necrosis of the femoral heads, of femur and tibia in the knee, and even of the shoulder girdle, although this may also be related to steroid exposure during treatment of pneumocystis pneumonia, alcoholism, smoking, and other risk factors (Brown and Crane 2001; Valencia et al. 2003) encountered more frequently in the HIV-infected population.
Glucose intolerance, hypertriglyceridemia, and hypercholesterolemia (Carr et al. 1881, 1998; Caron et al. 2001) can be induced by protease inhibitors, more so with first-generation PIs (e.g., indinavir) as well as the NRTIs 3TC and FTC (Dressman et al. 2003; Lenhard et al. 2000). These changes may be mediated by changes in nuclear localization of the sterol regulatory element-binding protein-1 (SREBP-1) and changes in expression of peroxisome proliferator-activated receptor gamma (PPAR-gamma) and the insulin receptor (Caron et al. 2001). A variety of studies have reported that lipodystrophy (fat redistribution) and accelerated atherosclerotic disease occurring in individuals treated with HAART have been associated with total time on HAART (Caron et al. 2001; Dressman et al. 2003; Lenhard et al. 2000; Carr 2000; Bozzette et al. 2003; Friiis-Mǿller et al. 2003; Bogner et al. 2001; Mallon et al. 2003; Blanco et al. 2003; Seminari et al. 2002; Joly et al. 2002; Worm et al. 2002).
In addition to the previously mentioned association between abacavir hypersensitivity and host genotype (Mallal et al. 2002), other associations between response to antivirals and genetic background have been noted, including significant variation in serum levels of efavirenz and nelfinavir obtained during therapy in individuals with polymorphisms in the multidrug resistance transporter 1 gene (MDR1), organic anion transporters (OAT), P-450 alleles, and uracil gUGT (Fellay et al. 2002). Different alleles of the MDR1/P-glycoprotein efflux system may also affect CNS levels of antiretroviral drugs (Kim 2003). Polymorphisms uncommon in the Caucasian and European populations but common in individuals of African descent strongly affect efavirenz metabolism, leading to increased toxicity in susceptible individuals.
Resistance. While the medicine cabinet seems replete with choices, a little resistance can go a long way in limiting effective therapy, often requiring more toxic and less tolerable combinations to be effective. Drug resistance can be either transmitted with a founding virus or acquired, as the result of treatment to prior regimens. As noted above, the latter was common during the introduction of HAART in the mid- and late 1990s, as a large proportion of the population had acquired NRTI resistance. This led to acquisition of resistance to early protease inhibitor regimens, and often to NNRTI resistance after introduction of first-generation NNRTIs. Often the only choice was to wait, to maintain patients on failing regimens, until the time that two or more agents with full activity became available. Later drugs in most antiretroviral classes were designed to both increase activity against viruses resistant to earlier members and increase the genetic barrier to resistance (see Fig. 2—genetic barrier to resistance). Among NRTIs, tenofovir appears less susceptible, likely because of decreased replication fitness in mutants harboring the K65R mutation. Similarly, among NNRTIs, etravirine provides some rescue of K103N positive strains resistant to nevirapine and efavirenz (though Y181C, frequent in recipients of nevirapine, remains significant). To some extent tipranavir, and to a greater extent darunavir, are examples of protease inhibitors developed to be active against strains resistant to many or all other PIs. While INSTIs were only introduced in 2007 and generally require several mutations to completely abolish antiviral activity, the newest, dolutegravir, also retain activity against some raltegravir-resistant strains (Tang and Shafer 2012; Shafer 2002; Richman 2000; Larder et al. 2000; Hertogs et al. 2000; Wensing et al. 2014; Castagna et al. 2014).

Genotypic barrier to resistance in antiretroviral drugs. Vertically, INSTI, NRTI, NNRTI, and PI classes are shown from top to bottom in alternating light gray and light blue backgrounds (see text for drug abbreviations:. Horizontal grouping of drugs by number of mutations needed to render the antiretroviral ineffective are very approximate, as mutations at single positions that have higher replication cost (K65R, multi-NTRI substitution mutations) can still inactivate some drugs (e.g., tenofovir, loprinavir, and darunavir) shown further to the right in the figure. Data extrapolated from multiple sources (Emini et al. 1993; Tang and Shafer 2012; Shafer 2002; Richman 2000; Larder et al. 2000; Hertogs et al. 2000; Paredes et al. 1955; Palmer et al. 2006; Hunt et al. 2014; Garcia-Diaz et al. 2014; Simen et al. 2014; Wensing et al. 2014)
Drug–Drug interactions. Some antiretrovirals should never be used together due to metabolic antagonism (e.g., zidovudine and stavudine), and many cannot be used together with other antiretrovirals or with other medications a patient may be taking due to non-HIV-related medical conditions. Some antivirals require acid conditions for absorption (e.g., ATV, RPV) and should not be used with caution or avoided in patients on proton pump inhibitors or H2 antihistamines for acid-peptic disease. Others require dosage adjustment in patients with reduced renal function (e.g., 3TC, FTC, and TDF). Analysis of the patterns of efflux pumps (MDRs, MRDPs, OATs, others), elimination (e.g., UGT1A1 glucuronidation), metabolism, inhibition, and induction (principally microsomal enzymes) sometimes predict favorable and unfavorable interactions (see Table 1, “Metabolic pathways important to drug-drug interactions”), but may also fail to predict significant interactions (e.g., tenofovir reduction of atazanavir concentrations) and may suggest avoidance of combinations where only minimal changes occur (e.g., nevirapine and azole antifungals) when drug levels are measured. There appears to be no substitute for empiric determination.
4 Toward a Cure, (dys)Functional, or Otherwise
The philosophy of “treat early, treat hard” as a strategy for cure must be understood only in light of estimates that ranged as low as 4 years for the virus to disappear in the body of infected individuals. As data accumulated on rate of decay of proviral HIV DNA in resting memory T cells (Ho et al. 1995; Saag et al. 1996; Mellors et al. 1997; Perelson et al. 1996; Strain et al. 2013; Chun et al. 1995), the best estimates for the half-lives of viral reservoirs increased to the point that it was uncertain that any decay was taking place at all. Current data suggest that complete suppression of virus for a lifetime might not achieve cure (Strain et al. 2003) by antiviral treatment alone.
However anecdotal and some systematic study data suggest that cure of HIV may be possible, at least in some certain situations. A great deal of popular media coverage has been devoted to “The Berlin Patient” who received an hematopoietic stem cell transplant (HSCT) for acute myelogenous leukemia from a non-related donor homozygous for the CCR5Δ32 mutation (Hutter et al. 2009), conferring resistance to R5 tropic HIV-1 [note this same description has been used for an earlier elite controller (Jessen et al. 2014)]. This patient has remained free of replicating virus (but not completely free of fragments of proviral RNA as detectable by droplet digital PCR) (Yukl et al. 2013). Two additional patients who were heterozygous for CCR5Δ32 underwent HSCT using matched donors who were wild-type CCR5+ (“The Boston Patients”) in 2010 (Henrich et al. 2013). While viral DNA disappeared in transplanted subjects while on therapy, both experienced viral rebound 12–32 weeks after stopping ART (Henrich et al. 2014).
Other examples have stirred hope that cure of HIV-1 infection might be effected by treated very early with potent therapy, after which ART could be withdrawn, with persistent suppression of viral replication. The so-called Mississippi Baby, who was treated beginning 30 h after birth with ART for 18 months, which was then withdrawn, with undetectable viremia for years (Persaud et al. 2013). The “Mississippi Baby’s” mother was a long-term non-progressor, suggesting potential genetic factors. However, this infant relapsed with the mother’s virus after two years off of therapy (Rainwater-Lovett et al. 2015).
A longer, more heterogeneous, and less well-controlled literature has reported long-term control after early treatment followed by treatment cessation, most recently exemplified by 14 individuals treated within 2 months of acquiring HIV infection in the ANRS VISCONTI trial (Sáez-Cirión et al. 2013) who have had extended periods of low-level viremia off ART for 48–115 months. Importantly, the majority of these individuals do have detectable viremia and cannot be considered “cured” in a virological sense. Whether this simply reflects a tiny minority with outlying delayed stochastic reactivation, compared to prompt reactivation of replication in 3–8 weeks in most who stop ART (Deeks et al. 2005), or reflects some as yet undescribed genetic or functional advantage is unclear.
Regardless of inspiration, there has been a growing emphasis on the attempted eradication of HIV by activating HIV replication in the face of ongoing ART, a strategy termed “kick and kill.” Initial efforts to do this with agents such as anti-CD3 and interleukin-2 (Prins et al. 1999) showed substantial toxicity. The most clinically advanced current studies have employed better tolerated histone deacetylase inhibitors (HDACs) such as vorinostat (Archin et al. 2012, 2014) and romidepsin (Wei et al. 2014) while continuing ART. These and other attempted interventions have not as yet shown much of an effect on overall HIV viral burden (Rasmussen et al. 2013), but other agents and/or more complicated or esoteric strategies (e.g., autologous stem transplantation with engineered CRISPR/Cas-9 CCR5 knockout or other perturbations, additional pharmacologic agents) are actively being explored (Rasmussen et al. 2013).
5 Preventative Treatment
While there have been some discrepant results in the use of both topical and oral tenofovir for the prevention of HIV infection [e.g., the FemPrEP (Van Damme et al. 2012) and VOICE trials (Peterson et al. 2007)], most studies have found that taken consistently, tenofovir, or especially tenofovir + emtricitabine (Truvada) can effectively reduce acquisition of HIV by up to 90 % in a variety of populations, including men who have sex with men (Grant et al. 2010; Grohskopf et al. 2013), heterosexuals (Baeten et al. 2012; Thigpen et al. 2012), and IV drug users (Choopanya et al. 2013). The studies that failed to show protective effects generally were plagued by low adherence as ascertained by report and/or pill count (FemPrEP) or with low levels of detectable drug despite good reported adherence (VOICE trial, 80 %+ by report or pill count but with only 30 % detectable drug on pharmacologic monitoring). Aside from these failures, results seem remarkably consistent across widely varying populations and geographic regions: (1) The PrEx trial showed 46 % reduction in MSM overall with 92 % in those with levels of TDF/FTC detectable in the blood (based in South America (Peterson et al. 2007), and in the US MSM trial none of 6 participants who seroconverted had yet received drug, (2) In the PartnersPrep Trial, overall estimates of efficacy were 67 % for tenofovir alone and 75 % for Truvada (Grohskopf et al. 2013), and the TDF2 trial showed an overall efficacy of 62 % in reduction of infection (Baeten et al. 2012). (3) In IVDU in Bangkok, Thailand, an overall reduction of infection of 48 % was achieved, increasing to 74 % in those displaying detectable tenofovir in their blood upon testing (Choopanya et al. 2013).
While trials are still ongoing including investigation of alternative strategies other than daily, continuous drug treatment, the evidence is sufficiently compelling that the CDC has issued guidelines for PrEP in high-risk individuals, including suggesting monitoring practices (US Public Health Service 2014). Resistance, while infrequent, has been described to result from preventative treatment (Peterson et al. 2007; Grant et al. 2010; Grohskopf et al. 2013) and remains a concern to clinicians and for public health as PrEP treatment becomes more widespread.
6 Concluding Remarks
Optimal drug treatment of HIV infection is a rapidly moving, continuously improving target (Department of Health and Human Services 2014). There are considerable incentives to develop new agents with entirely different mechanisms of action as well as improved generations of current drugs that display more favorable pharmacokinetics, lower toxicity profiles, and have activity against strains resistant to currently available agents. Exploration of strategies to possibly permanent (or at least durable) cure of some patient populations is in progress. New technologies, including drug monitoring, genetic testing, and improved resistance testing, may also expedite achievement of therapeutic goals. The expansion of HIV treatment to new populations presents unique challenges, and the use of antiretrovirals for preventative treatment, while it may save millions of lives, may also risk making resistance to the most commonly used agents more widespread.
Abbreviations
- HAART:
-
Highly active antiretroviral therapy
- ART:
-
Antiretroviral therapy
- HIV, HIV-1:
-
Human immunodeficiency virus, human immunodeficiency virus type 1
- AIDS:
-
Acquired immune deficiency syndrome
- PrEP:
-
Pre-exposure prophylaxis
- AZT:
-
Zidovudine
- ddI:
-
Didanosine
- ddC:
-
Zalcitidine
- d4T:
-
Stavudine
- 3TC:
-
Lamivudine
- FTC:
-
Emtricitabine
- ABC:
-
Abacavir
- TDF:
-
Tenofovir disoproxil fumarate
- RT:
-
Reverse transcriptase
- DNA:
-
Deoxyribonucleic acid
- RNA:
-
Ribonucleic acid
- NVP:
-
Nevirapine
- EFV:
-
Efavirenz
- ETV:
-
Etravirine
- DLV:
-
Delavirdine
- RPV:
-
Rilpivirine
- SQV:
-
Saquinavir
- IDV:
-
Indinavir
- NFV:
-
Nelfinavir
- FPV:
-
Fosamprenavir
- LPV:
-
Lopinavir
- RTV/r:
-
Ritonavir
- TPV:
-
Tipranavir
- ATV:
-
Atazanavir
- DRV:
-
Darunavir
- T20:
-
Enfurvirtide
- RAL:
-
Raltegravir
- ETG:
-
Elvitegravir
- DTG:
-
Dolutegravir
- MVC:
-
Maraviroc
- NRTI:
-
Nucleoside reverse transcriptase inhibitor
- NNRTI:
-
Non-nucleoside reverse transcriptase inhibitor
- TP:
-
Triphosphate
- NS5A:
-
Non-structural protein 5A of hepatitis C virus
- Kd:
-
Kilodalton
- PI:
-
Protease inhibitor
- INSTI:
-
Integrase strand transfer inhibitor
- CSF:
-
Cerebrospinal fluid
- CYP3A:
-
Cytochrome P450 isoform protein 3A
- HBV:
-
Hepatitis B virus
- HCV:
-
Hepatitis C virus
- DHHS:
-
Department of health and human services
- IC50:
-
Inhibitory concentration 50 %
- PCR:
-
Polymerase chain reaction
- SREBP-1:
-
Sterol regulator element-binding protein 1
- PPAR-gamma:
-
Peroxisome proliferator-activated receptor gamma
- OAT, OATP:
-
Organic anion transporter
- gUGT:
-
Glucuronosyltransferase
- CNS:
-
Central nervous system
- MDR1:
-
Multidrug resistance transporter 1
- HSCT:
-
Hematopoetic stem cell transplant
- CCR5:
-
CC Chemokine receptor 5 gene
- ANRS:
-
Agence Nationale de Recherche sur le Sida
- VISCONTI:
-
Virological and immunological studies in controllers after treatment interruption
- CD3:
-
Cluster of differentiation surface marker 3
- CD4:
-
Cluster of differentiation surface marker 4
- HDAC:
-
Histodeacytelase inhibitor
- CRISPR:
-
Clustered regularly interspaced short palindromic repeat protein
- Cas-9:
-
CRISPR-associated protein 9
- Fem-PrEP:
-
Women’s preventative treatment study
- VOICE:
-
Vaginal and oral interventions to control the epidemic
- MSM:
-
Men who have sex with men
- US:
-
United States
- IVDU:
-
Intravenous drug users
- CDC:
-
Centers for Disease Control
- NIH:
-
National Institutes of Health
- DAIDS:
-
Division of AIDS
- NIAID:
-
National Institute of Allergy and Infectious Disease
- NIMH:
-
National Institute of Mental Health
- NIDA:
-
National Institute of Drug Abuse
- NICHD:
-
National Institute of Child Health and Human Development
- NHLBI:
-
National Heart Lung and Blood Institute
- NIGMS:
-
National Institute of General Medical Sciences
- NIDDK:
-
National Institute of Diabetes and Digestive and Kidney Diseases
- NIA:
-
National Institute on Aging
- PPI:
-
Proton pump inhibitor
- ADH:
-
Alcohol dehydrogenase
- OCT2:
-
Organic cation transporter 2
- MATE1:
-
Multidrug and toxin extrusion protein 1
- UGT1A:
-
Uracil diphosphate glucuronosyltransferase 1 protein family
- CYPnLn, nLn:
-
Cytochrome protein isoforms of P-450, e.g., CYP1A2 or 1A2, CYP1A6, or 1A6.
References
Archin NM, Liberty AL, Kashuba AD, Choudhary SK, Kuruc JD, Crooks AM, Parker DC, Anderson EM, Kearney MF, Strain MC, Richman DD, Hudgens MG, Bosch RJ, Coffin JM, Eron JJ, Hazuda DJ, Margolis DM (2012) Administration of vorinostat disrupts HIV-1 latency in patients on antiretroviral therapy. Nature 487(7408):482–485 (PMCID: PMC3704185)
Archin NM, Bateson R, Tripathy MK, Crooks AM, Yang KH, Dahl NP, Kearney MF, Anderson EM, Coffin JM, Strain MC, Richman DD, Robertson KR, Kashuba AD, Bosch RJ, Hazuda DJ, Kuruc JD, Eron JJ, Margolis DM (2014) HIV-1 expression within resting CD4+ T cells after multiple doses of vorinostat. J Infect Dis 210(5):728–735. doi:10.1093/infdis/jiu155 (Epub 2014 Mar 11. PMC4148603)
Arenas-Pinto A, Grant AD, Edwards S, Weller IVD (2003) Lactic acidosis in HIV infected patients: a systematic review of published cases. Sex Transm Infect 79:340–344
Arnaudo E, Dalakas M, Shanske S, Moraes CT, DiMauro S, Schon EA (1991) Depletion of muscle mitochondrial DNA in AIDS patients with zidovudine-induced myopathy. Lancet 337(8740):508–510
Baeten JM, Donnell D, Ndase P et al (2012) Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med 367(5):399–410
Baxter JD, Mayers DL, Wentworth DN, Neaton JD, Hoover ML, Winters MA, Mannheimer SB, Thompson MA, Abrams DI, Brizz BJ, Ioannidis JP, Merigan TC (2000) A randomized study of antiretroviral management based on plasma genotypic antiretroviral resistance testing in patients failing therapy. AIDS 14(9):F83–F93 (The CPCRA 046 study team for the terry beirn community programs for clinical research on AIDS)
Bedimo RJ, McGinnis KA, Dunlap M, Rodriguez-Barradas MC, Justice AC (2009) Incidence of non-AIDS-defining malignancies in HIV-infected versus noninfected patients in the HAART era: impact of immunosuppression. J Acquir Immune Defic Syndr 52:203
Blanco F, Garcia-Benayas T, Jose de la Cruz J, Gonzalez-Lahoz J, Soriano V (2003) First-line therapy and mitochondrial damage: different nucleosides, different findings. HIV Clin Trials 4(1):11–19
Bogner JR, Vielhauer V, Beckmann RA, Michl G, Wille L, Salzberger B, Goebel FD (2001) Stavudine versus zidovudine and the development of lipodystrophy. J Acquir Immune Defic Syndr 27(3):237–244
Borges AH, Silverberg MJ, Wentworth D et al (2013) Predicting risk of cancer during HIV infection: the role of inflammatory and coagulation biomarkers. AIDS 27(9):1433–1441
Boubaker K, Flepp M, Sudre P, Furrer H, Haensel A, Hirschel B et al (2001) Hyperlactatemia and antiretroviral therapy: the Swiss HIV cohort study. Clin Infect Dis 33:1931–1937
Bozzette SA, Ake CF, Tam HK et al (2003) Cardiovascular and cerebrovascular events in patients treatedfor human immunodeficiency virus infection. N Engl J Med 348(8):702
Brown P, Crane L (2001) Avascular necrosis of bone in patients with human immunodeficiency virus infection: report of 6 cases and review of the literature. Clin Infect Dis 32(8):1221–1226
Caron M, Auclair M, Vigouroux C, Glorian M, Forest C, Capeau J (2001) The HIV protease inhibitor indinavir impairs sterol regulatory element-binding protein-1 intranuclear localization, inhibits preadipocyte differentiation, and induces insulin resistance. Diabetes 50:1378–1388
Carr A (2000) HIV protease inhibitor-related lipodystrophy syndrome. Clin Infect Dis 30(Suppl 2):S135–S142
Carr A, Samaras K, Chisolm DJ, Cooper DA (1881) Pathogenesis of HIV-1 protease inhibitor-associated peripheral lipodystrophy, hyperlipidaemia, and insulin resistance. Lancet 1998:351
Carr A, Samaras K, Burton S et al (1998) A syndrome of peripheral lipodystrophy (LD) hyperlipidemia and insulin resistance in patients receiving HIV protease inhibitors. AIDS 12:F51
Castagna A, Maggiolo F, Penco G, Wright D, Mills A, Grossberg R, Molina JM, Chas J, Durant J, Moreno S, Doroana M, Ait-Khaled M, Huang J, Min S, Song I, Vavro C, Nichols G, Yeo JM (2014) Dolutegravir in antiretroviral-experienced patients with raltegravir- and/or elvitegravir-resistant HIV-1: 24-week results of the phase III VIKING-3 study. J Infect Dis 210(3):354–362. doi:10.1093/infdis/jiu051 (Epub 2014 Jan 19. PubMed PMID: 24446523; PubMed Central) (VIKING-3 study group)
CDC (2011) Vital signs: HIV diagnosis, care, and treatment among persons living with HIV—United States. MMWR 63(47):1113–1117
Chesney M (2003) Adherence to HAART regimens. AIDS Patient Care STDS 17(4):169–177
Choopanya K, Martin M, Suntharasamai P et al (2013) Antiretroviral prophylaxis for HIV infection among people who inject drugs in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet 381(9883):2083–2090
Chow YK, Hirsch MS, Merrill DP, Bechtel LJ, Eron JJ, Kaplan JC, D’Aquila RT (1993) Use of evolutionary limitations of HIV-1 multidrug resistance to optimize therapy. Nature 361(6413):650–654 (Erratum in: Nature. 1993 Aug 19; 364(6439):679. PubMed PMID: 7679778)
Chun T-W, Finzi D, Margolick J, Chadwich K, Schwartz D, Siliciano RF (1995) Fate of HIV-1-infected T cells in vivo: rates of transition to stable latency. Nat Med 1:1284–1290
Cingolani A, Antinori A, Rizzo MG, Murri R, Ammassari A, Baldini F, Di Giambenedetto S, Cauda R, De Luca A (2002) Usefulness of monitoring HIV drug resistance and adherence in individuals failing highly active antiretroviral therapy: a randomized study (ARGENTA). AIDS 16(3):369–379
Clevenbergh P, Durant J, Halfon P, Giudice P, Mondain. V, Montagne N, Schapiro JM, Boucher CA, Dellamonica P (2000) Persisting long-term benefit of genotype-guided treatment for HIV-infected patients failing HAART. The viradapt study: week 48 follow-up. Antivir Ther 5(1):65–70
Coghlan ME, Sommadossi JP, Jhala NC, Many WJ, Saag MS, Johnson VA (2001) Symptomatic lactic acidosis in hospitalized antiretroviral-treated patients with human immunodeficiency virus infection: a report of 12 cases. Clin Infect Dis 33:1914–1921
Collier AC, Coombs RW, Fischl MA, Skolnik PR, Northfelt D, Boutin P, Hooper CJ, Kaplan LD, Volberding PA, Davis LG et al (1993) Combination therapy with zidovudine and didanosine compared with zidovudine alone in HIV-1 infection. Ann Intern Med 119:786–793
Cooper DA, Gatell JM, Kroon S, Clumeck N, Millard J, Goebel FD, Bruun JN, Stingl G, Melville RL, Gonzalez-Lahoz J et al (1993) Zidovudine in persons with asymptomatic HIV infection and CD4+ cell counts greater than 400 per cubic millimeter. The European-Australian Collaborative Group. N Engl J Med 329:297–303
Craigie R (2001) HIV integrase, a brief overview from chemistry to therapeutics. J Biol Chem 276(26):23213–23216
Crauwels H, Vingerhoets J, Ryan R et al (2012) Pharmacokinetic parameters of once-daily rilpivirine following administration of efavirenz in healthy subjects. Antivir Ther 17(3):439–446
Deeks SG, Hoh R, Neilands TB, Liegler T, Aweeka F, Petropoulos CJ, Grant RM, Martin JN (2005) Interruption of treatment with individual therapeutic drug classes in adults with multidrug-resistant HIV-1 infection. J Infect Dis 192(9):1537–1544 Epub 2005 Sep 20
DeGruttola V, Smith DM, Little SJ, Miller V (2010) Developing and evaluating comprehensive HIV infection control strategies: issues and challenges. Clin Infect Dis 15(50 Suppl 3):S102–S107. doi:10.1086/651480 (Review. PubMed PMID: 20397937; PubMed Central PMCID: PMC2913596)
Department of Health and Human Services (2014) DHHS adult and adolescent guidelines—panel on antiretroviral guidelines for adults and adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf. Section accessed 13 Nov 2014
Dorr P, Westby M, Dobbs S, Griffin P, Irvine B, Macartney M, Mori J, Rickett G, Smith-Burchnell C, Napier C, Webster R, Armour D, Price D, Stammen B, Wood A, Perros M (2005) Maraviroc (UK-427,857), a potent, orally bioavailable, and selective small-molecule inhibitor of chemokine receptor CCR5 with broad-spectrum anti-human immunodeficiency virus type 1 activity. Antimicrob Agents Chemother 49(11):4721–4732 (PMCID: PMC1280117)
Dressman J, Kincer J, Matveev SV, Guo L, Greenberg RN, Guerin T, Meade D, Li XA, Zhu W, Uittenbogaard A, Wilson ME, Smart EJ (2003) HIV protease inhibitors promote atherosclerotic lesion formation independent of dyslipidemia by increasing CD36-dependent cholesteryl ester accumulation in macrophages. J Clin Invest 111:389–397
Duprez DA, Neuhaus J, Kuller LH et al (2012) Inflammation, coagulation and cardiovascular disease in HIV-infected individuals. PLoS One 7(9):e44454
Emini EA, Graham DJ, Gotlib L, Condra JH, Byrnes VW, Schleif WA (1993) HIV and multidrug resistance. Nature 364(6439):679
Fellay J, Marzolini C, Meaden ER, Back DJ, Buclin T, Chave JP, Decosterd LA, Furrer H, Opravil M, Pantaleo G, Retelska D, Ruiz L, Schinkel AH, Vernazza P, Eap CB, Telenti A, Swiss HIV (2002) Cohort Study. Response to antiretroviral treatment in HIV-1-infected individuals with allelic variants of the multidrug resistance transporter 1: a pharmacogenetics study. Lancet 359(9300):30–306
Feng JY, Johnson AA, Johnson KA, Anderson KS (2001) Insights into the molecular mechanism of mitochondrial toxicity by AIDS drugs. J Biol Chem 276:23832–23837
Fischl MA, Richman DD, Grieco MH, Gottlieb MS, Volberding PA, Laskin OL, Leedom JM, Groopman JE, Mildvan D, Schooley RT et al (1987) The efficacy of azidothymidine (AZT) in the treatment of patients with AIDS and AIDS-related complex. A double-blind, placebo-controlled trial. N Engl J Med 317:185–191
Fletcher CV, Acosta EP, Henry K et al (1998) Concentration-controlled zidovudine therapy. Clin Pharmacol Ther 64:331–338
Friiis-Mǿller N,Weber R, D’Armininio Monforte A et al (2003) Exposure to HAART is associated with an increased risk of myocardial infarction: the D:A:D study. In: Presented at: 10th conference on retroviruses and opportunistic, Abstract No. 130, Boston, Mass, 10–14 Feb 2003
Furman PA, Fyfe JA, St.Clair MH, Weinhold K, Rideout JL, Freeman GA et al (1986) Phosphorylation of 3′-azido-3′-deoxythymidine and selective interaction of the 5′-triphosphate with human immunodeficiency virus reverse transcriptase. Proc Natl Acad Sci 85:8333–8337
Garcia-Diaz A, McCormick A, Booth C, Gonzalez D, Sayada C, Haque T, Johnson M, Webster D (2014) Analysis of transmitted HIV-1 drug resistance using 454 ultra-deep-sequencing and the DeepChek(®)-HIV system. J Int AIDS Soc 17(4 Suppl 3):19752 (PMCID: PMC4225408)
Gilliam BL, Sajadi MM, Amoroso A, Davis CE, Cleghorn FR, Redfield RR (2007) Tenofovir and abacavir combination therapy: lessons learned from an urban clinic population. AIDS Patient Care STDS 21(4):240–246
Graham NM, Hoover DR, Park LP, Stein DS, Phair JP, Mellors JW, Detels R, Saah AJ (1996) Survival in HIV-infected patients who have received zidovudine: comparison of combination therapy with sequential monotherapy and continued zidovudine monotherapy. Multicenter AIDS cohort study group. Ann Intern Med 124:1031–1038
Grant RM, Lama JR, Anderson PL et al (2010) Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med 363(27):2587–2599. doi:10.1056/NEJMoa1011205
Grohskopf LA, Chillag KL, Gvetadze R et al (2013) Randomized trial of clinical safety of daily oral tenofovir disoproxil fumarate among HIV-uninfected men who have sex with men in the United States. J Acquired Immune Defic Syndr 64(1):79–86
Gulick RM, Mellors JW, Havlir D, Eron JJ, Gonzalez C, McMahon D, Richman DD, Valentine FT, Jonas L, Meibohm A, Emini EA, Chodakewitz JA (1997) Treatment with indinavir, zidovudine, and lamivudine in adults with human immunodeficiency virus infection and prior antiretroviral therapy. N Engl J Med 337(11):734–739
Hamers RL, Sigaloff KC, Kityo C, Mugyenyi P, de Wit TF (2013) Emerging HIV-1 drug resistance after roll-out of antiretroviral therapy in sub-Saharan Africa. Curr Opin HIV AIDS 8(1):19–26
Henrich TJ, Hu Z, Li JZ, Sciaranghella G, Busch MP, Keating SM et al (2013) Long-term reduction in peripheral blood HIV type 1 reservoirs following reduced-intensity conditioning allogeneic stem cell transplantation. J Infect Dis 207(11):1694–1702
Henrich TJ, Hanhauser E, Marty FM, Sirignano MN, Keating S, Lee TH, Robles YP, Davis BT, Li JZ, Heisey A, Hill AL, Busch MP, Armand P, Soiffer RJ, Altfeld M, Kuritzkes DR (2014) Antiretroviral-free HIV-1 remission and viral rebound after allogeneic stem cell transplantation: report of 2 cases. Ann Intern Med 161(5):319–327. doi:10.7326/M14-1027 (PubMed PMID: 25047577; PubMed Central PMCID: PMC4236912)
Hertogs K, Bloor S, Kemp SD, Van den Eynde C, Alcorn TM, Pauwels R, Van Houtte M, Staszewski S, Miller V, Larder BA (2000) Phenotypic and genotypic analysis of clinical HIV-1 isolates reveals extensive protease inhibitor cross-resistance: a survey of over 6000 samples. AIDS 14(9):1203–1210
Ho DD, Neumann AU, Perelson AS, Chen W, Leonard JM, Markowitz M (1995) Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 infection. Nature 373:123–126
Hunt GM, Morris L, Moorthy A, Coovadia A, Abrams EJ, Strehlau R, Kuhn L, Persaud D (2014) Concordance between allele-specific PCR and ultra-deep pyrosequencing for the detection of HIV-1 non-nucleoside reverse transcriptase inhibitor resistance mutations. J Virol Methods 207:182–187 (PMC4150030)
Hutter G, Nowak D, Mossner M, Ganepola S, Mussig A, Allers K et al (2009) Long-term control of HIV by CCR5 Delta32/Delta32 stem-cell transplantation. N Engl J Med 360(7):692–698
Iversen AK, Shafer RW, Wehrly K, Winters MA, Mullins JI, Chesebro B, Merigan TC (1996) Multidrug-resistant human immunodeficiency virus type 1 strains resulting from combination antiretroviral therapy. J Virol 70:1086–1090
Jessen H, Allen TM, STreek H (2014) How a single patient influenced HIV research—15-year follow-up. N Engl J Med 370:682–683. doi:10.1056/NEJMc1308413
Jilek BL, Zarr M, Sampah ME, Rabi SA, Bullen CK, Lai J, Shen L, Siliciano RF (2012) A quantitative basis for antiretroviral therapy for HIV-1 infection. Nat Med 18(3):446–451. doi:10.1038/nm.2649 (PubMed PMID: 22344296; PubMed Central PMCID: PMC3296892)
Johnson JA, Sax PE (2014) Beginning antiretroviral therapy for patients with HIV. Infect Dis Clin North Am 28(3):421–438
Joly V, Flandre P, Meiffredy V, Leturque N, Harel M, Aboulker JP, Yeni P (2002) Increased risk of lipoatrophy under stavudine in HIV-1-infected patients: results of a substudy from a comparative trial. AIDS 16(18):2447–2454
Kim RB (2003) Drug transporters in HIV Therapy. Top HIV Med 11(4):136–139
Knobel H, Carmona A, Grau S, Pedro-Botet J, Diez A (1998) Adherence and effectiveness of highly active antiretroviral therapy. Arch Intern Med 158(17):1953
Kohlstaedt LA, Wang J, Friedman JM, Rice PA, Steitz RA (1992) Crystal structure at 3.5 a resolution of HIV-1 reverse transcriptase complexed with an inhibitor. Science 256:1783–1790
Kretzschmar ME, Schim van der Loeff MF, Birrell PJ, De Angelis D, Coutinho RA (2013) Prospects of elimination of HIV with test-and-treat strategy. Proc Natl Acad Sci USA 110(39):15538–15543. doi:10.1073/pnas.1301801110 (Epub 2013 Sep PubMed PMID: 24009342; PubMed Central PMCID: PMC3785722)
Kulkarni SP, Shah KR, Sarma KV, Mahajan AP (2013) Clinical uncertainties, health service challenges, and ethical complexities of HIV “test-and-treat”: a systematic review. Am J Public Health. 103(6):e14–e23. doi:10.2105/AJPH.2013.301273 (Epub 2013 Apr 18. Review. PubMed PMID: 23597344)
Kuller LH, Tracy R, Belloso W et al (2008) Inflammatory and coagulation biomarkers and mortality in patients with HIV infection. PLoS Med 5(10):e203
Lalezari JP, Henry KO, Hearn M et al (2003) Enfuvirtide, an HIV-1 fusion inhibitor, for drug-resistant HIV infection in North and South America. N Engl J Med 348(22):2175–2185
Larder BA, Kemp SD, Hertogs K (2000) Quantitative prediction of HIV-1 phenotypic drug resistance from genotypes: the virtual phenotype (VirtualPhenotype). Antiviral Ther 5(suppl 3):49
Laskey SB, Siliciano RF (2014) A mechanistic theory to explain the efficacy of antiretroviral therapy. Nat Rev Microbiol 12(11):772–780. doi:10.1038/nrmicro3351 (Epub 2014 Sep 29)
Lazzarin A, Clotet B, Cooper D et al (2003) Efficacy of enfuvirtide in patients infected with drug-resistant HIV-1 in Europe and Australia. N Engl J Med 348(22):2186–2195
Lenhard JM, Furfine ES, Jain RG, Ittoop O, Orband-Miller LA, Blanchard SG, Paulik MA, Weiel JE (2000) HIV protease inhibitors block adipogenesis and increase lipolysis in vitro. Antiviral Res 47:121–129
Little SJ, Holte S, Routy JP, Daar ES, Markowitz M, Collier AC, Koup RA, Mellors JW, Connick E, Conway B, Kilby M, Wang L, Whitcomb JM, Hellmann NS, Richman DD (2002) Antiretroviral-drug resistance among patients recently infected with HIV. N Engl J Med 347(6):385–394
Loutfy MR, Antoniou T, Shen S, Diong C, Vlaicu M, Halpenny R, Kovacs C, Fletcher D, Raboud JM (2007) Virologic and immunologic impact and durability of enfuvirtide-based antiretroviral therapy in HIV-infected treatment-experienced patients in a clinical setting. HIV Clin Trials 8(1):36–44 (PMID: 17434847)
Mallal S, Nolan D, Witt C, Masel G, Martin AM, Moore C, Sayer D, Castley A, Mamotte C, Maxwell D, James I, Christiansen FT (2002) Association between presence of HLA-B*5701, HLA-DR7, and HLA-DQ3 and hypersensitivity to HIV-1 reverse-transcriptase inhibitor abacavir. Lancet 359:727–732
Mallon PW, Miller J, Cooper DA, Carr A (2003) Prospective evaluation of the effects of antiretroviral therapy on body composition in HIV-1-infected men starting therapy. AIDS 17(7):971–979
Mao C, Sudbeck EA, Venkatachalam TK, Uckun FM (2000) Structure-based drug design of non-nucleoside inhibitors for wild-type and drug resistant HIV reverse transcriptase. Biochem Pharmacol 60:1251–1265
Mathias AA, German P, Murray BP, Jain A, West S, Warren D, Hui J, Kearney BP (2010) Pharmacokinetics and pharmacodynamics of GS-9530: a novel pharmacokinetic enhancer without anti-HIV activity. Clin Pharmaco Ther 87:322–329
Mellors JW, Munoz A, Giorgi JV, Margolick JB, Tassoni CJ, Gupta P, Kingsley LA, Todd JA, Saah AJ, Detels R, Phair JP, Rinaldo CR Jr (1997) Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med 126(12):946–954
Meng TC, Fischl MA, Boota AM, Spector SA, Bennett D, Bassiakos Y, Lai SH, Wright B, Richman DD (1992) Combination therapy with zidovudine and dideoxycytidine in patients with advanced human immunodeficiency virus infection. A phase I/II study. Ann Intern Med 116:13–20
Roberts NA, Martin JA, Kinchington D, Broadhurst AV, Craig JC, Duncan IB, Galpin SA, Handa BK, Kay J, Kröhn A, Lambert RW, Merrett, MJS, Parkes KEB, Redshaw S, Ritchie AJ, Taylor DL, Thomas GJ, Machin PJ (1990) Rational design of peptide-based HIV proteinase inhibitors. Science 248:358
Montaner JS, Harrigan PR, Jahnke N et al (2001) Multiple drug rescue therapy for HIV-infected individuals with prior virologic failure to multiple regimens. AIDS 15(1):61–69
Moore RD, Keruly JC, Chaisson RE (2001) Incidence of pancreatitis in HIV-infected patients receiving nucleoside reverse transcriptase inhibitor drugs. AIDS 15:617–620
Nachega JB, Uthman OA, del Rio C, Mugavero MJ, Rees H, Mills EJ (2014) Addressing the Achilles’ heel in the HIV care continuum for the success of a test-and-treat strategy to achieve an AIDS-free generation. Clin Infect Dis 59(Suppl 1):S21–S27. doi:10.1093/cid/ciu299 PubMed PMID: 24926028; PubMed Central PMCID:PMC4141496
Palmer S, Boltz V, Martinson N, Maldarelli F, Gray G, McIntyre J, Mellors J, Morris L, Coffin J (2006) Persistence of nevirapine-resistant HIV-1 in women after single-dose nevirapine therapy for prevention of maternal-to-fetal HIV-1 transmission. Proc Natl Acad Sci USA 103(18):7094–7099 (PMCID: PMC1459023)
Paredes R, Marconi VC, Campbell TB, Kuritzkes DR (2007) Systematic evaluation of allele-specific real-time PCR for the detection of minor HIV-1 variants with pol and env resistance mutations. J Virol Methods 146(1–2):136–46 (PMCID: PMC4195598)
Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier C, Wagener MM, Singh N (2000) Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med 133(1):21–30
Perelson AS, Neumann AU, Markowitz M, Leonard JM, Ho DD (1996) HIV-1 dynamics in vivo: virion clearance rate, infected cell life-span, and viral generation time. Science 271:1582–1586
Persaud D, Gay H, Ziemniak C et al (2013) Absence of detectable HIV-1 viremia after treatment cessation in an infant. N Engl J Med 369:1828–1835
Peterson L, Taylor D, Roddy R et al (2007) Tenofovir disoproxil fumarate for prevention of HIV infection in women: a phase 2, double-blind, randomized, placebo-controlled trial. PLoS Clin Trials 2(5):e27
Pollard RB, Robinson P, Dransfield K (1998) Safety profile of nevirapine, a nonnucleoside reverse transcriptase inhibitor for the treatment of human immunodeficiency virus infection. Clin Ther 20:1071–1089
Pozniak AL, Morales-Ramirez J, Katabira E et al (2010) TMC278-C204 study group. Efficacy and safety of TMC278 in antiretroviral-naive HIV-1 patients: week 96 results of a phase IIb randomized trial. AIDS 24(1):55–565
Prins JM, Jurriaans S, van Praag RM, Blaak H, van Rij R, Schellekens PT, ten Berge IJ, Yong SL, Fox CH, Roos MT, de Wolf F, Goudsmit J, Schuitemaker H, Lange JM (1999) Immuno-activation with anti-CD3 and recombinant human IL-2 in HIV-1-infected patients on potent antiretroviral therapy. AIDS 13(17):2405–2410
Rainwater-Lovett K, Luzuriaga K, Persaud D (2015) Very early combination antiretroviral therapy in infants: prospects for cure. Curr Opin HIV AIDS 10(1):4–11. doi:10.1097/COH.0000000000000127
Rasmussen TA, Tolstrup M, Winckelmann A, Østergaard L, Søgaard OS (2013) Eliminating the latent HIV reservoir by reactivation strategies: advancing to clinical trials. Hum Vaccin Immunother 9(4):790–799. doi:10.4161/hv.23202 (Epub 2013 Apr 1. Review. PMCID: PMC3903897)
Richman D (2000) Principles of HIV resistance testing and overview of assay performance characteristics. Antivir Ther 5:27–31
Rimsky L, Vingerhoets J, Van Eygen V et al (2012) Genotypic and phenotypic characterization of HIV-1 isolates obtained from patients on rilpivirine therapy experiencing virologic failure in the phase 3 ECHO and THRIVE studies: 48-week analysis. J Acquir Immune Defic Syndr. 59(1):39–346
Rockstroh JK (2015) Optimal therapy of HIV/HCV co-infected patients with direct acting antivirals. Liver Int 35(Suppl 1):51–555. doi:10.1111/liv.12721
Saag MS, Holodniy M, Kuritzkes DR, O’Brien WA, Coombs R, Poscher ME, Jacobsen DM, Shaw GM, Richman DD, Volberding PA (1996) HIV viral load markers in clinical practice. Nat Med 2(6):625–629
Sabin CA, Worm SW, Weber R et al (2008) Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A: D study: a multi-cohort collaboration. Lancet 371(9622):1417–1426
Sáez-Cirión A, Bacchus C, Hocqueloux L, Avettand-Fenoel V, Girault I, Lecuroux C, Potard V, Versmisse P, Melard A, Prazuck T, Descours B, Guergnon J, Viard JP, Boufassa F, Lambotte O, Goujard C, Meyer L, Costagliola D, Venet A, Pancino G, Autran B, Rouzioux C (2013) Post-treatment HIV-1 controllers with a long-term virological remission after the interruption of early initiated antiretroviral therapy ANRS VISCONTI study. PLoS Pathog 9(3):e1003211 (PMC3597518 ANRS) (VISCONTI study group)
Sandler NG, Wand H, Roque A et al (2011) Plasma levels of soluble CD14 independently predict mortality in HIV infection. JInfect Dis 203(6):780–790
Schooley RT, Ramirez-Ronda C, Lange JM, Cooper DA, Lavelle J, Lefkowitz L, Moore M, Larder BA, St Clair M, Mulder JW, McKinnis R, Pennington KN, Harrigan PR, Kinghorn I, Steel H, Rooney JF (1996) Virologic and immunologic benefits of initial combination therapy with zidovudine and zalcitabine or didanosine compared with zidovudine monotherapy. Wellcome Resistance Study Collaborative Group. J Infect Dis 173:1354–1366
Scribner AN, Troia-Cancio PV, Cox BA, Marcantonio D, Hamid F, Keiser P, Levi M, Allen B, Murphy K, Jones RE, Skiest DJ (2000) Osteonecrosis in HIV: a case-control study. J Acquir Immune Defic Syndr 25(1):19–25
Seminari E, Tinelli C, Minoli L, Sacchi P, Filice G, Zocchetti C, Meneghetti G, Bruno R, Maserati R (2002) Evaluation of the risk factors associated with lipodystrophy development in a cohort of HIV-positive patients. Antivir Ther 7(3):175–180
Shafer RW (2002) Genotypic testing for human immunodeficiency virus type 1 drug resistance. Clin Microbiol Rev 15:247–277
Shen L, Rabi SA, Sedaghat AR, Shan L, Lai J, Xing S, Siliciano RF (2011) A critical subset model provides a conceptual basis for the high antiviral activity of major HIV drugs. Sci Trans Med 3(91):91ra63. doi:10.1126/scitranslmed.3002304 (PubMed PMID: 21753122; PubMed Central PMCID: PMC3488347)
Shiels MS, Pfeiffer RM, Gail MH et al (2011) Cancer burden in the HIV-infected population in the United States. J Natl Cancer Inst 103(9):753–762
Simen BB, Braverman MS, Abbate I, Aerssens J, Bidet Y, Bouchez O, Gabriel C, Izopet J, Kessler HH, Stelzl E, Di Giallonardo F, Schlapbach R, Radonic A, Paredes R, Recordon-Pinson P, Sakwa J, St John EP, Schmitz-Agheguian GG, Metzner KJ, Däumer MP (2014) 454 HIV Alphastudy Group. An international multicenter study on HIV-1 drug resistance testing by 454 ultra-deep pyrosequencing. J Virol Methods 204:31–37 (PMID: 24731928)
Smerdon SJ, Jager J, Wang J, Kohlstaedt LA, Chirino AJ, Friedman JM et al (1994) Structure of the binding site for nonnucleoside inhibitors of the reverse transcriptase of human immunodeficiency virus type 1. Proc Natl Acad Sci 91:3911–3915
Smith C (2010) Factors associated with specific causes of death amongst HIV-positive individuals in the D:A: D study. AIDS 24(10):1537–1548
St Clair MH, Richards CA, Spector T, Weinhold KJ, Miller WH, Langlois AJ et al (1987) 3′-Azido-3′-deoxythymidine triphosphate as an inhibitor and substrate of purified human immunodeficiency virus reverse transcriptase. Antimicrob Agents Chemother 31:1972–1977
Strain MC, Gunthard HF, Havlir DV, Ignacio CC, Smith DM, Leigh-Brown AJ, Macaranas TR, Lam RY, Daly OA, Fischer M, Opravil M, Levine H, Bacheler L, Spina CA, Richman DD, Wong JK (2003) Heterogeneous clearance rates of long-lived lymphocytes infected with HIV: intrinsic stability predicts lifelong persistence. Proc Natl Acad Sci USA 100(8):4819–4824
Strain MC, Lada SM, Luong T, Rought SE, Gianella S, Terry VH, Spina CA, Woelk CH, Richman DD (2013) Highly precise measurement of HIV DNA by droplet digital PCR. PLoS One 8(4):e55943 (PMCID: PMC3616050)
Tang MW, Shafer RW (2012) HIV-1 antiretroviral resistance: scientific principles and clinical applications. Drugs. 72(9):e1–e25 (PMCID: PMC3689909)
Thigpen MC, Kebaabetswe PM, Paxton LA et al (2012) Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med 367(5):423–434
Toji L, Cohen S (1969) The enzymatic termination of polydeoxynucleotides by 2′,3′-dideoxydenosine triphosphate. Proc Natl Acad Sci 63:871–877
Tural C, Ruiz L, Holtzer C, Schapiro J, Viciana P, Gonzalez J, Domingo P, Boucher C, Rey-Joly C, Clotet B (2002) Havana study group. Clinical utility of HIV-1 genotyping and expert advice: the Havana trial. AIDS 16(2):209–218
United States Food and Drug Administration (2014) Antiretroviral drugs used in the treatment of HIV infection. Sept 2014. http://www.fda.gov/ForPatients/Illness/HIVAIDS/Treatment/ucm118915.htm
US Public Health Service (2014) Preexposure prophylaxis for the prevention of HIV infection in the united states—2014 clinical practice guideline. Centers for disease control, URL—http://www.cdc.gov/hiv/pdf/PrEPguidelines2014.pdf
Valencia ME, Barreiro P, Soriano V, Blanco F, Moreno V, Lahoz JG (2003) Avascular necrosis in HIV-infected patients receiving antiretroviral treatment: study of seven cases. HIV Clin Trials 4(2):132–136
Van Damme L, Corneli A, Ahmed K et al (2012) Preexposure prophylaxis for HIV infection among African women. N Engl J Med 367(5):411–422
Wei DG, Chiang V, Fyne E, Balakrishnan M, Barnes T, Graupe M, Hesselgesser J, Irrinki A, Murry JP, Stepan G, Stray KM, Tsai A, Yu H, Spindler J, Kearney M, Spina CA, McMahon D, Lalezari J, Sloan D, Mellors J, Geleziunas R, Cihlar T (2014) Histone deacetylase inhibitor romidepsin induces HIV expression in CD4 T cells from patients on suppressive antiretroviral therapy at concentrations achieved by clinical dosing. PLoS Pathog 10(4):e1004071 (PMCID: PMC3983056)
Wensing AM, Calvez V, Günthard HF, Johnson VA, Paredes R, Pillay D, Shafer RW, Richman DD (2014) 2014 Update of the drug resistance mutations in HIV-1. Top Antivir Med 22(3):642–650 (PubMed PMID: 25101529)
World Health Organization (2014) Global update on the health sector response to HIV. HIV reporting. ISBN 9789241507585
Worm D, Kirk O, Andersen O, Vinten J, Gerstoft J, Katzenstein TL, Nielsen H, Pedersen CR (2002) Clinical lipoatrophy in HIV-1 patients on HAART is not associated with increased abdominal girth, hyperlipidaemia or glucose intolerance. HIV Med 3(4):239–246
Worm SW, Bower M, Reiss P et al (2013) Non-AIDS defining cancers in the D:A: D study–time trends and predictors of survival: a cohort study. BMC Infect Dis 13:471
Yatchoan R, Broder S (1987) Development of antiretroviral therapy for the acquired immunodeficiency syndrome and related disorders; a progress report. N Engl J Med 316:557–564
Youle M, Tyrer M, Fisher M et al (2002) Brief report: two-year outcome of a multidrug regimen in patients who did not respond to a protease inhibitor regimen. J Acquir Immun Defic Syndr 29(1):58–61
Yukl SA, Boritz E, Busch M, Bentsen C, Chun TW, Douek D et al (2013) Challenges in detecting HIV persistence during potentially curative interventions: a study of the Berlin patient. PLoS Pathog 9(5):e1003347
Acknowledgments:
The authors wish to thank the Veterans Administration and the VA San Diego Healthcare System for their continued support for excellence in clinical care of HIV-infected veterans. This work was also supported by the University of California, San Diego, Center for AIDS Research, NIH/DAIDS P30 AI036214, which is in turn supported by the following NIH Institutes and Centers: NIAID, NCI, NIMH, NIDA, NICHD, NHLBI, NIA, NIGMS, and NIDDK. Thanks for assistance, proofing, and comments from Douglas Richman, David Goodsell, Bruce Torbett, and Wei-Wei Chiu.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Looney, D., Ma, A., Johns, S. (2015). HIV Therapy—The State of ART. In: Torbett, B., Goodsell, D., Richman, D. (eds) The Future of HIV-1 Therapeutics. Current Topics in Microbiology and Immunology, vol 389. Springer, Cham. https://doi.org/10.1007/82_2015_440
Download citation
DOI: https://doi.org/10.1007/82_2015_440
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18517-0
Online ISBN: 978-3-319-18518-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)