
Abstract
Renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system play crucial roles in heart failure with reduced ejection fraction (HFrEF). Clinical trials provide strong evidence of prognostic benefits for combination therapy with angiotensin-converting enzyme inhibitor (ACEI) and β-blocker in the treatment of HFrEF. Angiotensin receptor blocker (ARB) is not superior to ACEI in improving mortality and an alternative for patients who are intolerant to ACEI. Prognostic evidence for triple therapy which combined angiotensin receptor blocker (ARB) and ACEI in addition to β-blocker therapy, is still controversial in HFrEF. Moreover, a recent clinical trial showed that triple therapy did not provide additional benefit compared with ACEI or ARB therapy alone in mildly symptomatic HFrEF. Of note, the triple therapy can even cause harm and renal dysfunction in HF with a history of hypertension. Direct renin inhibitor (DRI) has the theoretical benefit of upstream RAAS inhibition at the point of pathway activation. However, the results from clinical trials do not support upstream renin inhibition by DRI in addition to standard therapy with ACEI in patients with HFrEF. Angiotensin receptor-neprilysin inhibitor (ARNI) which combines a neprilysin inhibitor and ARB valsartan have a unique mode of action targeting both RAAS and the natriuretic peptide systems. In contrast to the evidence in HFrEF, clinical value of combination therapy with RAAS inhibitors and β-blocker is not well established in HF with preserved EF (HFpEF). The heterogeneity of diagnostic criteria and baseline characteristics of HFpEF need further evidence for the combination therapy. However, a recent clinical trial of LCZ696 showed promising results in reducing NT-proBNP in patients with HFpEF.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Angiotensin receptor blocker
- Angiotensin receptor-neprilysin inhibitor
- Angiotensin-converting enzyme
- Direct renin inhibitor
- Ejection fraction
- Heart failure
- Mineralocorticoid receptor antagonist
- Prognosis
- Renin-angiotensin-aldosterone system
- β-blocker
1 Introduction
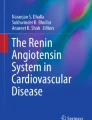
The renin-angiotensin-aldosterone system (RAAS) is a signaling pathway responsible for regulating blood pressure and fluid balance (Garg and Yusuf 1995; Yusuf et al. 2003; Paul et al. 2006; Kobori et al. 2007). (Fig. 1) The RAAS plays a crucial role in heart failure with reduced ejection fraction (HFrEF). Blocking RAAS by angiotensin-converting enzyme inhibitor (ACEI), angiotensin receptor blocker (ARB) and mineralocorticoid receptor antagonist (MRA) improve prognosis in HFrEF and are recommended by professional guidelines (Writing Committee et al. 2013; Ponikowski et al. 2016a) β blocker has ability to reverse the neurohumoral effects of the sympathetic nervous system (Eichhorn et al. 1991) and lowers plasma renin levels (Holmer et al. 1998) with ensuing symptomatic and prognostic benefits, and thus attained recommendation by the guidelines (Writing Committee et al. 2013; Ponikowski et al. 2016a). This section summarizes evidence of combination use with RAAS inhibitors and beta blockers in HF, especially in HFrEF.

Renin-angiotensin-aldosterone pathway. Abbreviations; ACEI angiotensin converting enzyme inhibitor, ARB angiotensin receptor blocker, DRI direct renin inhibitor, MRA Mineralocorticoid receptor antagonist
2 ACEI in HFrEF
The first study demonstrating prognostic benefit by ACEI in HFrEF patents was the CONSENSUS (Cooperative North Scandinavian Enalapril Survival Study) in 1987 (Group CTS 1987; Swedberg and Kjekshus 1988). The CONSENSUS demonstrated that, in 253 HFrEF patients with NYHA (New York Heart Association) class IV, treatment with enalapril (2.5-40 mg/day) significantly reduced the risk of mortality at 6-month (26% in enalapril vs. 44% in placebo) and 1-year (36% vs. 52%). In the CONSENSUS, the reduction in mortality by enalapril was attributed to significantly lower risk of mortality resulting from progression of HFrEF (a reduction of 50%) (Group CTS 1987). The findings from the CONSENSUS was confined to severe HFrEF patients and no data on prognosis were available for patients with mildly symptomatic HF. Following the accomplishment of the CONSENSUS, the SOLVD (Studies of Left Ventricular Dysfunction) trial showed that treatment with enalapril over a mean of 41.4 months reduced the risk of death by 16% (95% confidence interval; 5–26%) among HFrEF patients with mild-to-moderate symptoms (SOLVD Investigators et al. 1991; The SOLVD Investigators 1990). Align with the CONSENSUS, the beneficial effect of enalapril for prognosis in the SOLVD was due to reduction of death from progression of HF. Besides survival benefits, patients receiving enalapril experienced hypotension more frequently than those receiving placebo in both the CONSENSUS and SOLVD.
3 ARB in HFrEF
ARBs (angiotensin II receptor blockers) are antagonists of angiotensin II type I receptor, which have less side effects, such as coughs and angioedema, as compared with ACEIs. Evidence of ARB in HFrEF is still limited. Head-to-head comparison between ACEI and ARB was conducted in the ELITE (Evaluation of Losartan in the Elderly) II trial enrolling 3,152 HFrEF (EF ≤ 40%) patients age 60 years or older with NYHA class II-IV. The results of ELITE II demonstrated no significant difference in mortality between ARB losartan and ACEI captopril (Pitt et al. 2000; Willenheimer 2000). In addition, the investigators observed significant fewer adverse event rates in losartan group (Pitt et al. 2000; Willenheimer 2000). Furthermore, the CHARM (Candesartan in Heart failure Assessment of Reduction in Mortality and morbidity)-Alternative trial showed that an ARB candesartan comparing placebo was generally well tolerated and reduced cardiovascular mortality and morbidity in 2,028 HFrEF (EF < 40%) patients who are intolerance to ACE inhibitors (Granger et al. 2003). Based on these results, professional guidelines recommended ARB is considered as an alternative for patients who cannot tolerate ACEI due to cough or angioedema which are adverse effects of ACEI (Writing Committee et al. 2013; Ponikowski et al. 2016a).
4 MRA in HFrEF
Increasing evidence suggested that ACEI did not effectively suppress the production of aldosterone based on the pathophysiological observations (Borghi et al. 1993; Staessen et al. 1981; Struthers 2004; Andrew 2002). Hence, the RALES trial was initialized to evaluate the role of MRA in addition to ACEI in the treatment of advanced HFrEF (Pitt et al. 1999; Weber 1999). Specifically, the RALES (Randomized Aldactone Evaluation Study) aimed to determine whether spironolactone would reduce mortality in patients with advanced HF and an EF < 35%, who were already on standard medical therapy (ACEI, if tolerated, and diuretics). The RALES clearly demonstrated that adding 25 mg of spironolactone to standard therapy reduced all-cause mortality in HFrEF (EF < 35%) patients (Pitt et al. 1999). The success of the RALES with severe HFrEF patients prompted the subsequent EMPHASIS-HF trial (Zannad et al. 2011) which investigated MRA eplerenone in the treatment of moderate HFrEF with mild symptoms, reinforcing the benefits of MRA in HFrEF. Evidence from these trials established ACEI (ARB if in non-tolerated to ACEI) (Writing Committee et al. 2013; Ponikowski et al. 2016a; Cohn and Tognoni 2001) and MRA as standard therapies in HFrEF.
5 β-Blocker in HFrEF
β-blockers have ability to reverse the neurohumoral effects of the sympathetic nervous system (Eichhorn et al. 1991) and lowers plasma renin levels (Holmer et al. 1998) with ensuing symptomatic and prognostic benefits with recommendation by the guidelines (Writing Committee et al. 2013; Ponikowski et al. 2016a). In 1974, Finn Waagstein et al. first reported that practolol dramatically improved patient’s clinical status in a 59-year woman with HFrEF and suggested benefits of a β-blocker, practolol in patients with HFrEF (Waagstein et al. 1974; Waagstein and Rutherford 2017). A subsequent study from his group demonstrated the clinical benefits of the β-blocker in patients with HFrEF (Waagstein et al. 1974, 1975; Waagstein and Hjalmarson 1976).
6 Combination Therapy with ACEI and β-Blocker in HFrEF
Since angiotensin II increase the sympathetic drive, which was proven to be harmful in patients with HF. Combining ACEI/ARB with β blocker could provide summed blockage to the sympathetic nervous system with additional benefit. (Fig. 1) The prognostic value of the combination therapy with ACEI and β-blocker was demonstrated by the US Carvedilol trial (Packer et al. 1996). In NYHA II-IV HFrEF (EF < 40%) patients receiving ACEI, a mean daily dose of 45 ± 27 mg of carvedilol had a 65% lower risk of death than those given placebo during follow-up of 6.5 months and of extended 15 months. (Table 1) The results from the US Carvedilol were clear in terms of survival benefit by carvedilol. However, since carvedilol exerts pharmacologic effects atypical of and in addition to its action on adrenergic receptors, (Yoshikawa et al. 1996; Foody et al. 2002) it was not clear that all β-blockers would prolong survival in HFrEF patients. The beneficial effects of other β-blockers were confirmed in the CIBIS-II (Cardiac Insufficiency Bisoprolol Study II; bisoprolol) and MERIT (Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure; mrtoprolol) (Packer et al. 1999a, b). The value of carvedilol was further confirmed in severe HFrEF by the COPERNICUS (Carvedilol Prospective Randomized Cumulative Survival) trial, which enrolled 2,289 HFrEF (EF < 25%) patients with HF symptom at rest or on minimal exertion (Packer et al. 2001). In the COPERNICUS, the addition of carvedilol to ACEI, diuretics, and digitalis for a mean of 10.4 months decreased the rate of death by 35% (95%CI; 19–48%, P < 0.001) and the rate of death or hospitalization by 24% (13–33%, P < 0.001). (Table 1) The COPERNICUS provided further evidence that suppressing the neurohormonal axis can delay the progression of HF in HFrEF and improve survival in the acute setting.
Along with recognition of improved prognosis in HFrEF by combination therapy with β-blocker and ACEI, one question arose on the order of treatments, β-blocker first or ACEI first? To answer this, the CIBIS-III trial was designed comparing initial monotherapy with either bisoprolol or enalapril for 6 months followed by their combination for 6–24 months on mortality and hospitalization (Willenheimer et al. 2005). Regardless of order of initiation treatment, the combination use of a β-blocker to an ACE inhibitor further reduces mortality. Of note, the investigators observed the bisoprolol-first arm was associated with numerically increased risk of worsening HF (HR 1.25 [95%CI 0.87–1.81], P = 0.23). The risk of worsening HF in bisoprolol-first strategy, however, could be improved with greater experience of up titration of the β-blocker.
7 Triple Therapy of ACEI, ARB and β-Blocker in HFrEF
There is no study to test specifically prognostic impact of triple therapy, such as ARB add-on therapy to ACE inhibitor and β-blocker in the large clinical HF trial. However, the role of triple therapy in HF patients has also been evaluated in three trials, the Val-Heft (Valsartan Heart Failure Trial), the CHARM (Candesartan in Heart failure Assessment of Reduction in Mortality and Morbidity)-Added, and the SUPPORT (supplemental benefit of ARB in hypertensive patients with stable heart failure using olmesartan) (Cohn and Tognoni 2001; McMurray et al. 2003; Sakata et al. 2015). (Table 2) In 2001, the Val-Heft evaluated the long-term effects of the addition of an ARB valsartan to standard therapy (approximately 93% in ACEI use; 35% in β-blocker use) in 5,010 HFrEF (EF < 40%) patients with NYHA II-IV who randomly assigned to receive ARB valsartan or placebo. Mortality was similar in the two treatment groups. However, a post-hoc analysis of the Val-Heft revealed that patients who received triple therapy of ACEI, ARB and β-blocker had a significantly increased mortality (P = 0.009), and a trend toward an increase in the composite endpoint defined as cardiac arrest with resuscitation, hospitalization for HF, or administration of intravenous inotropic or vasodilator drugs for 4 h or more without hospitalization (P = 0.10) (Cohn and Tognoni 2001). In contrast, in the CHARM-Added which enrolled 2,548 HFrEF (EF < 40%) patients with NYHA II–IV, triple therapy (56% in β-blocker use) was associated with a reduction in the composite of cardiovascular death or HF hospitalization (0·85 [95% CI 0.75–0.96], P = 0.011), when compared to placebo. In addition, there was no difference in all-cause death (HR 0·88 [0.72–1.08], P = 0.22) (McMurray et al. 2003; Swedberg et al. 1999).
Given the different results between Val-Heft and CHARM-added, the value of ARB add-on therapy to ACEI was controversial. In 2015, the SUPPORT, which investigated whether an additive treatment with an ARB olmesartan, reduces the mortality and morbidity in 1,147 HF patients with a history of hypertension (7% in NYHA class III; 72% in β-blocker use; 81% in ACEI use; 19% of EF ≤ 40%), provided additional information of triple therapy (Sakata et al. 2015; Sakata et al. 2013). The composite event rates of all-cause death, non-fatal acute myocardial infarction, non-fatal stroke, and hospitalization for worsening HF were not different between olmesartan and control groups (HR 1.18 [0.96–1.46], P = 0.112), whereas renal dysfunction developed more frequently in the olmesartan group (HR 1.64 [1.19–2.26], P = 0.003). Furthermore, a post-hoc analysis of the SUPPORT trial suggested that triple therapy may be harmful in patients with HF: among patients already receiving an ACEI and β-blocker, adding olmesartan was associated with increased incidence of the primary endpoint (HR 1.47 [1.11–1.95], P = 0.006), all-cause death (HR 1.50 [1.01–2.23], P = 0.046), and renal dysfunction (HR 1.85 [95% CI 1.24–2.76], P = 0.003) (Sakata et al. 2015). The results of the SUPPORT and Val-Heft indicate no benefit of triple therapy, which is in contract to what was observed in the CHARM-added trial (Cohn and Tognoni 2001; McMurray et al. 2003; Danser and van den Meiracker 2015). This discrepancy could be explained by the differences in patients’ demographics; the majority of the patients in the CHARM-Added had NYHA class III (73%), in contrast to 38% in the Val-Heft, and 7% in the SUPPORT. Thus, although the routine use of triple therapy may be avoided in mildly symptomatic HF with a history of hypertension, it remains to be examined whether the triple combination therapy could be beneficial for HF patients with severe symptoms. A large trial comparing ARB added on to ACEI, β-blocker, and MRA (quad therapy) has not been performed yet (Table 3).
8 Comprehensive Blockade with Direct Renin Inhibitor, Aliskiren, ACEI and β-Blocker in HFrEF
The pathophysiological concept of a complete RAAS blockade was further tackled by direct renin inhibitor (DRI) (Rahuel et al. 2000; Wood et al. 2003). DRI provides another pharmacologically distinct means of suppressing the RAAS, with the theoretical advantages of blocking an enzyme with only one known substrate, angiotensinogen, providing the theoretical benefit of upstream RAAS inhibition at the point of pathway activation. (Fig. 1) Adding Aliskiren, a first-in-class orally active DRI on ACEI and β-blocker has shown favorable neurohumoral effects in terms of reducing plasma BNP (brain natriuretic peptide) levels compared with placebo in the ALOFT (Aliskiren Observation of Heart Failure Treatment) study (McMurray et al. 2008) which included HFrEF patients with NYHA II-IV, current or past history of hypertension, and plasma BNP > 100 pg/mL who had been treated with an ACEI and β-blocker (mean age 68 years; mean EF 31%; NYHA II 62%). Furthermore, aliskiren was associated with a significant reduction in urinary aldosterone excretion, supporting the hypothesis that a DRI strategy may reduce aldosterone escape with prognostic benefit. However, the results of the ASTRONAUT (AliSkiren TRial ON Acute heart failure oUTcomes) and ATMOSPHERE (Aliskiren Trial to Minimize OutcomeS in Patients with HEart failuRE) trials did not support this hypothesis in terms of prognosis (Gheorghiade et al. 2013; McMurray et al. 2016). In the ASTRONAUT, HFrEF (EF ≤ 40%,) patients with BNP ≥ 400 pg/mL (or N -terminal pro-BNP [NT-proBNP] ≥1,600 pg/mL), and signs and symptoms of fluid overload were randomized to aliskiren or placebo. Patients assigned aliskiren experienced a significant and sustained drop in blood levels of NT-proBNP through 12 months follow-up (Gheorghiade et al. 2013). However, no statistical difference was observed in the event rates for composite of cardiovascular death or HF hospitalization (aliskiren, 35.0% vs. placebo 37.3%; HR 0.93; 95%CI [0.79–1.09], P = 0.36) at 12 months. In addition, hyperkalemia, renal dysfunction and hypotension were reported more frequently in the aliskiren group. Given by the non-beneficial impact with greater side effect by aliskiren, the ASTRONAUT trial implies that there might be a ceiling to the benefit with RAAS modulation, and further inhibition beyond ACEI does not provide any incremental benefit. This argument was reinforced by the results from the ATMOSPHERE trial. The ATMOSPHERE trial randomized 2,336 patients with NYHA II-IV and elevated BNP to receive enalapril alone, 2,340 to receive aliskiren, and 2,340 to receive combination therapy with aliskiren and enalapril (combination therapy) (McMurray et al. 2016; Krum et al. 2015). The primary composite outcome of all-cause death and HF hospitalization occurred in 32.9% of the combination therapy group, in 34.6% in the enalapril group (HR 0.93; 95%CI [0.85–1.03], P = 0.17) and in 33.8% in the aliskiren group (vs. enalapril, 0.99 [0.90–1.10], P = 0.91). Adverse event rates for aliskiren alone group were similar to those of enalapril alone. However, like the ASTRONAUT trial, in the ATMOSPHERE trial, there was a higher risk of hypotensive symptoms in the combination therapy group than in the enalapril alone group (13.8% vs. 11.0%, P = 0.005), and higher risks of an elevated serum creatinine level (4.1% vs. 2.7%, P = 0.009) and an elevated potassium level (17.1% vs. 12.5%, P < 0.001). The results from the ASTORONOUT and ATMOSPHERE do not support upstream renin inhibition in addition to standard therapy with ACEI in patients with HFrEF.
9 Comprehensive Blockade for RAAS and Natriuretic Peptide System in HFrEF
LCZ696 (sacubitril/valsartan) is a new class of agents called angiotensin receptor-neprilysin inhibitors (ARNIs) which combines a neprilysin inhibitor and an ARB valsartan. LCZ696 has a unique mode of action targeting both RAAS and the natriuretic peptide systems because sacubitril inhibits the neprilysin, which increases the level of natriuretic peptides rather than leading to additional blockage. (Fig. 1) Recent data from the PARADIGM-HF (Prospective Comparison of Angiotensin Receptor-Neprilysin Inhibitor with Angiotensin-Converting Enzyme Inhibitor to Determine Impact on Global Mortality and Morbidity in Heart Failure) trial suggests more comprehensive RAAS modulation with other RAAS axis blocking agents may have led to clinical benefit in HF patients and reduced EF (McMurray et al. 2014; McMurray et al. 2013). The PARADIGM-HF randomized 8,399 NYHA II-IV HFrEF (≤40% and ≤35% were used at different time points in the trial) patients to LCZ696 or enalapril. With a median follow-up of 27 months, the trial was stopped early due to a positive interval efficacy analysis. The LCZ696 added to standard therapy with 93% of patients already taking β-blocker and 54% taking MRA led to a reduction in the primary composite outcome of cardiovascular death or HF hospitalization (21.8% vs. 26.5%; HR 0.80 95%CI [0.73–0.87], P < 0.001) as well as each of the individual components of the composite outcome. Of note, LCZ696 had a significant reduction in all-cause death (17.0% vs. 19.8%; HR 0.84 95%CI [0.76–0.93], P < 0.001). LCZ696 was generally well tolerated except for a higher rate of hypotension and there was no difference in the rates of angioedema. Following the PARADIGM-HF, the US Food and Drug Administration approved LCZ696 for the treatment of HF. Furthermore, professional HF guidelines endorse LCZ696 as a class I recommendation for the management of symptomatic HFrEF (Ponikowski et al. 2016b; Jessup et al. 2016). Although this high-quality clinical study is the largest and the most globally represented trial in HFrEF patients, concerns have been raised regarding the generalizability of the trial results in real-world HF population due to inclusion/exclusion criteria, run-in period and lower dose of enalapril in the control arm (Yandrapalli et al. 2017; Yancy et al. 2017).
10 RAAS Inhibitor, β-Blocker and Those Combination in HF and Preserved EF (HFpEF)
Approximately half of HF patients have an EF of 50% or higher (heart failure and preserved ejection fraction; HFpEF) (Owan et al. 2006). The randomized trials with RAASI [ACEI (Cleland et al. 2006) or ARB (Massie et al. 2008)] monotherapy failed to show prognostic benefits in HFpEF patients. For instance, a prespecified subgroup analysis of I-PRESERVED (Irbesartan in Heart Failure with Preserved Ejection Fraction Study) suggested that ARB monotherapy did not provide beneficial impact on prognosis in HFpEF (HR0.87[0.75–1.02], P for interaction of ARB to β-blocker = 0.14) Moreover, the effect of β-blockers monotherapy has not been evaluated in an adequately powered study with HFpEF patients (Conraads et al. 2012; Liu et al. 2014; van Veldhuisen et al. 2009; Yamamoto et al. 2013). In addition, evidence of combination therapy of RAAS inhibitor and β-blocker is predominant in HFrEF. However, several data exist on combination therapy for prognosis in HFpEF by three large clinical trials; CHARM-preserved, I-PRESERVED, and SUPPORT (Yusuf et al. 2003; Massie et al. 2008; Miura et al. 2016).
The CHARM-Preserved enrolled 3,025 patients with HFpEF (EF > 40%) and NYHA II-IV, and a history of hospitalization for a cardiac reason. In the CHARM-Preserved, there was no difference in the primary outcome of cardiovascular death or HF hospitalization between the candesartan and placebo groups (22% vs. 24%; HR 0.89 [95%CI 0.77–1.03], P = 0·118) (Yusuf et al. 2003). However, a signal was observed toward lower event rate for HF hospitalization in candesartan (0.85 [0.72–1.01], P = 0·072). Similar results were observed in the I-PRESERVED including 4,128 symptomatic HF (NYHA II-IV) patients with HFpEF (EF ≥ 45%) who were 60 years or older (Massie et al. 2008; Carson et al. 2005). In the I-Preserved, ARB Irbesartan did not improve the outcome defined by the composite of death from any cause or hospitalization for a cardiovascular cause (heart failure, myocardial infarction, unstable angina, arrhythmia, or stroke) in HFpEF. Post-hoc analysis from the SUPPORT, in HFpEF, the addition of olmesartan to β-blocker was significantly associated with lower event rate for all-cause death (HR 0.32 [0.12–0.90] P = 0.03), whereas addition to ACEI (1.85 [0.87–3.96], P = 0.11) or that to combination of ACEI and β-blocker (1.65 [0.93–2.94], P = 0.09) was not (Miura et al. 2016). In 2014, the TOPCAT (Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist) trial including patients with EF ≥45%, who had to have either a HF hospitalization within 12 months before randomization or, if not, an elevated brain natriuretic peptide (BNP; BNP ≥100 pg/mL or N-terminal pro-BNP ≥360 pg/mL) within 60 days before randomization, showed no difference between MRA spironolactone and placebo groups in the primary composite outcome of cardiovascular death, aborted cardiac arrest, or HF hospitalization (Pitt et al. 2014; Desai et al. 2011). However, in post-hoc analysis of the TOPCAT trial, spironolactone was associated with a significant reduction in the primary outcome for those in the United States, Canada, Brazil, and Argentina but not those in Russia/Georgia (Pfeffer et al. 2015). These lines of evidence call for further trials to assess clinical effect of combination therapy of RAAS inhibitor and β-blocker in HFpEF (Desai and Jhund 2016). To assess efficacy and safety of LCZ696 in HFpEF, the PARAMOUNT (Prospective comparison of ARNI with ARB on Management Of heart failUre with preserved ejectioN fracTion) trial was conducted in HFpEF (≥45%) patients with NYHA II-III, and NT-proBNP>400 pg/mL comparing LCZ696 (200 mg) with valsartan (160 mg) for 36 weeks (Solomon et al. 2012). NT-proBNP was significantly reduced at 12 weeks in the LCZ696 group compared with the valsartan group suggesting that LCZ696 may improve prognosis in HFpEF (Solomon et al. 2012). In near future, PARAGON-HF (Prospective Comparison of ARNI with ARB Global Outcomes in HF With Preserved Ejection Fraction) trial (Solomon et al. 2017; Filippatos et al. 2015) will provide evidence of whether LCZ696 is prognostically superior to ARB alone in patients with chronic symptomatic HFpEF (EF ≥ 45%).
11 Conclusions
With concrete evidence, RAAS blockade by combination with ACEI and β-blocker is a gold standard in the treatment of HFrEF. ARB clearly represent an alternative of treatment for patients who are intolerant to ACEI. Triple therapy with ACEI, ARB and β-blocker does not provide additional benefit in mildly symptomatic HFrEF. Furthermore, triple therapy can even cause harm and renal dysfunction in HF with a history of hypertension. Sacubitril inhibits the neprilysin which increases the level of natriuretic peptides rather than leads to additional blockage, and reduces NT-proBNP levels greater than an ARB in HFpEF. Whether this effect would translate into improved outcomes, is tested by PARAGON-HF trial. Given by the heterogeneity of diagnostic criteria and baseline characteristics of HFpEF, clinical benefit of combination therapy with RAASIs and β-blocker is controversial, and we need further evidence in HFpEF.
References
Andrew P (2002) Renin-angiotensin-aldosterone activation in heart failure, aldosterone escape. Chest 122(2):755
Borghi C, Boschi S, Ambrosioni E, Melandri G, Branzi A, Magnani B (1993) Evidence of a partial escape of renin-angiotensin-aldosterone blockade in patients with acute myocardial infarction treated with ACE inhibitors. J Clin Pharmacol 33(1):40–45
Carson P, Massie BM, McKelvie R, McMurray J, Komajda M, Zile M et al (2005) The irbesartan in heart failure with preserved systolic function (I-PRESERVE) trial: rationale and design. J Card Fail 11(8):576–585
Cleland JG, Tendera M, Adamus J, Freemantle N, Polonski L, Taylor J et al (2006) The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur Heart J 27(19):2338–2345
Cohn JN, Tognoni G (2001) Valsartan heart failure trial I. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N Engl J Med 345(23):1667–1675
Conraads VM, Metra M, Kamp O, De Keulenaer GW, Pieske B, Zamorano J et al (2012) Effects of the long-term administration of nebivolol on the clinical symptoms, exercise capacity, and left ventricular function of patients with diastolic dysfunction: results of the ELANDD study. Eur J Heart Fail 14(2):219–225
Danser AH, van den Meiracker AH (2015) Heart failure: new data do not SUPPORT triple RAAS blockade. Nat Rev Nephrol 11(5):260–262
Desai AS, Jhund PS (2016) After TOPCAT: what to do now in heart failure with preserved ejection fraction. Eur Heart J 37(41):3135–3140
Desai AS, Lewis EF, Li R, Solomon SD, Assmann SF, Boineau R et al (2011) Rationale and design of the treatment of preserved cardiac function heart failure with an aldosterone antagonist trial: a randomized, controlled study of spironolactone in patients with symptomatic heart failure and preserved ejection fraction. Am Heart J 162(6):966–972.e10
Eichhorn EJ, McGhie AL, Bedotto JB, Corbett JR, Malloy CR, Hatfield BA et al (1991) Effects of bucindolol on neurohormonal activation in congestive heart failure. Am J Cardiol 67(1):67–73
Filippatos G, Farmakis D, Parissis J, Lekakis J (2015) Drug therapy for patients with systolic heart failure after the PARADIGM-HF trial: in need of a new paradigm of LCZ696 implementation in clinical practice. BMC Med 13:35
Foody JM, Farrell MH, Krumholz HM (2002) Beta-blocker therapy in heart failure: scientific review. JAMA 287(7):883–889
Garg R, Yusuf S (1995) Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative group on ACE inhibitor trials. JAMA 273(18):1450–1456
Gheorghiade M, Bohm M, Greene SJ, Fonarow GC, Lewis EF, Zannad F et al (2013) Effect of aliskiren on postdischarge mortality and heart failure readmissions among patients hospitalized for heart failure: the ASTRONAUT randomized trial. JAMA 309(11):1125–1135
Granger CB, McMurray JJ, Yusuf S, Held P, Michelson EL, Olofsson B et al (2003) Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-alternative trial. Lancet 362(9386):772–776
Group CTS (1987) Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med 316(23):1429–1435
Holmer SR, Hense HW, Danser AH, Mayer B, Riegger GA, Schunkert H (1998) Beta adrenergic blockers lower renin in patients treated with ACE inhibitors and diuretics. Heart 80(1):45–48
Jessup M, Marwick TH, Ponikowski P, Voors AA, Yancy CW (2016) 2016 ESC and ACC/AHA/HFSA heart failure guideline update – what is new and why is it important? Nat Rev Cardiol 13(10):623–628
Kobori H, Nangaku M, Navar LG, Nishiyama A (2007) The intrarenal renin-angiotensin system: from physiology to the pathobiology of hypertension and kidney disease. Pharmacol Rev 59(3):251–287
Krum H, McMurray JJ, Abraham WT, Dickstein K, Kober L, Desai AS et al (2015) The Aliskiren trial to minimize OutcomeS in patients with HEart failure trial (ATMOSPHERE): revised statistical analysis plan and baseline characteristics. Eur J Heart Fail 17(10):1075–1083
Liu F, Chen Y, Feng X, Teng Z, Yuan Y, Bin J (2014) Effects of beta-blockers on heart failure with preserved ejection fraction: a meta-analysis. PLoS One 9(3):e90555
Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR et al (2008) Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med 359(23):2456–2467
McMurray JJ, Ostergren J, Swedberg K, Granger CB, Held P, Michelson EL et al (2003) Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function taking angiotensin-converting-enzyme inhibitors: the CHARM-Added trial. Lancet 362(9386):767–771
McMurray JJ, Pitt B, Latini R, Maggioni AP, Solomon SD, Keefe DL et al (2008) Effects of the oral direct renin inhibitor aliskiren in patients with symptomatic heart failure. Circ Heart Fail 1(1):17–24
McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR et al (2013) Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial (PARADIGM-HF). Eur J Heart Fail 15(9):1062–1073
McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR et al (2014) Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 371(11):993–1004
McMurray JJ, Krum H, Abraham WT, Dickstein K, Kober LV, Desai AS et al (2016) Aliskiren, Enalapril, or Aliskiren and Enalapril in heart failure. N Engl J Med 374(16):1521–1532
Miura M, Sakata Y, Miyata S, Shiba N, Takahashi J, Nochioka K et al (2016) Influence of left ventricular ejection fraction on the effects of supplemental use of angiotensin receptor blocker Olmesartan in hypertensive patients with heart failure. Circ J 80(10):2155–2164
Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM (2006) Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 355(3):251–259
Packer M, Bristow MR, Cohn JN, Colucci WS, Fowler MB, Gilbert EM et al (1996) The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. U.S. Carvedilol heart failure study group. N Engl J Med 334(21):1349–1355
Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P et al (1999a) The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet 353(9146):9–13
Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P et al (1999b) Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 353(9169):2001–2007
Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, Mohacsi P et al (2001) Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 344(22):1651–1658
Paul M, Poyan Mehr A, Kreutz R (2006) Physiology of local renin-angiotensin systems. Physiol Rev 86(3):747–803
Pfeffer MA, Claggett B, Assmann SF, Boineau R, Anand IS, Clausell N et al (2015) Regional variation in patients and outcomes in the treatment of preserved cardiac function heart failure with an aldosterone antagonist (TOPCAT) trial. Circulation 131(1):34–42
Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A et al (1999) The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone evaluation study investigators. N Engl J Med 341(10):709–717
Pitt B, Poole-Wilson PA, Segal R, Martinez FA, Dickstein K, Camm AJ et al (2000) Effect of losartan compared with captopril on mortality in patients with symptomatic heart failure: randomised trial--the losartan heart failure survival study ELITE II. Lancet 355(9215):1582–1587
Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B et al (2014) Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 370(15):1383–1392
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ et al (2016a) 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 37(27):2129–2200
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ et al (2016b) 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 18(8):891–975
Rahuel J, Rasetti V, Maibaum J, Rueger H, Goschke R, Cohen NC et al (2000) Structure-based drug design: the discovery of novel nonpeptide orally active inhibitors of human renin. Chem Biol 7(7):493–504
Sakata Y, Nochioka K, Miura M, Takada T, Tadaki S, Miyata S et al (2013) Supplemental benefit of an angiotensin receptor blocker in hypertensive patients with stable heart failure using olmesartan (SUPPORT) trial--rationale and design. J Cardiol 62(1):31–36
Sakata Y, Shiba N, Takahashi J, Miyata S, Nochioka K, Miura M et al (2015) Clinical impacts of additive use of olmesartan in hypertensive patients with chronic heart failure: the supplemental benefit of an angiotensin receptor blocker in hypertensive patients with stable heart failure using olmesartan (SUPPORT) trial. Eur Heart J 36(15):915–923
Solomon SD, Zile M, Pieske B, Voors A, Shah A, Kraigher-Krainer E et al (2012) The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet 380(9851):1387–1395
Solomon SD, Rizkala AR, Gong J, Wang W, Anand IS, Ge J et al (2017) Angiotensin receptor neprilysin inhibition in heart failure with preserved ejection fraction: rationale and design of the PARAGON-HF trial. JACC Heart Fail 5(7):471–482
SOLVD Investigators, Yusuf S, Pitt B, Davis CE, Hood WB, Cohn JN (1991) Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med 325(5):293–302
Staessen J, Lijnen P, Fagard R, Verschueren LJ, Amery A (1981) Rise in plasma concentration of aldosterone during long-term angiotensin II suppression. J Endocrinol 91(3):457–465
Struthers AD (2004) The clinical implications of aldosterone escape in congestive heart failure. Eur J Heart Fail 6(5):539–545
Swedberg K, Kjekshus J (1988) Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). Am J Cardiol 62(2):60A–66A
Swedberg K, Pfeffer M, Granger C, Held P, McMurray J, Ohlin G et al (1999) Candesartan in heart failure--assessment of reduction in mortality and morbidity (CHARM): rationale and design. Charm-programme investigators. J Card Fail 5(3):276–282
The SOLVD Investigators (1990) Studies of left ventricular dysfunction (SOLVD)--rationale, design and methods: two trials that evaluate the effect of enalapril in patients with reduced ejection fraction. Am J Cardiol 66(3):315–322
van Veldhuisen DJ, Cohen-Solal A, Bohm M, Anker SD, Babalis D, Roughton M et al (2009) Beta-blockade with nebivolol in elderly heart failure patients with impaired and preserved left ventricular ejection fraction: data from SENIORS (Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors with heart failure). J Am Coll Cardiol 53(23):2150–2158
Waagstein F, Hjalmarson AC (1976) Effect of cardioselective beta-blockade on heart function and chest pain in acute myocardial infarction. Acta Med Scand Suppl 587:193–200
Waagstein F, Rutherford JD (2017) The evolution of the use of beta-blockers to treat heart failure: a conversation with Finn Waagstein, MD. Circulation 136(10):889–893
Waagstein F, Hjalmarson AC, Wasir HS (1974) Apex cardiogram and systolic time intervals in acute myocardial infarction and effects of practolol. Br Heart J 36(11):1109–1121
Waagstein F, Hjalmarson A, Varnauskas E, Wallentin I (1975) Effect of chronic beta-adrenergic receptor blockade in congestive cardiomyopathy. Br Heart J 37(10):1022–1036
Weber KT (1999) Aldosterone and spironolactone in heart failure. N Engl J Med 341(10):753–755
Willenheimer R (2000) Angiotensin receptor blockers in heart failure after the ELITE II trial. Curr Control Trials Cardiovasc Med 1(2):79–82
Willenheimer R, van Veldhuisen DJ, Silke B, Erdmann E, Follath F, Krum H et al (2005) Effect on survival and hospitalization of initiating treatment for chronic heart failure with bisoprolol followed by enalapril, as compared with the opposite sequence: results of the randomized Cardiac Insufficiency Bisoprolol Study (CIBIS) III. Circulation 112(16):2426–2435
Wood JM, Maibaum J, Rahuel J, Grutter MG, Cohen NC, Rasetti V et al (2003) Structure-based design of aliskiren, a novel orally effective renin inhibitor. Biochem Biophys Res Commun 308(4):698–705
Writing Committee M, Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr et al (2013) 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation 128(16):e240–e327
Yamamoto K, Origasa H, Hori M, Investigators JD (2013) Effects of carvedilol on heart failure with preserved ejection fraction: the Japanese Diastolic Heart Failure Study (J-DHF). Eur J Heart Fail 15(1):110–118
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Colvin MM et al (2017) 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the heart failure society of America. Circulation 136(6):e137–ee61
Yandrapalli S, Andries G, Biswas M, Khera S (2017) Profile of sacubitril/valsartan in the treatment of heart failure: patient selection and perspectives. Vasc Health Risk Manag 13:369–382
Yoshikawa T, Port JD, Asano K, Chidiak P, Bouvier M, Dutcher D et al (1996) Cardiac adrenergic receptor effects of carvedilol. Eur Heart J 17(Suppl B):8–16
Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ et al (2003) Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-preserved trial. Lancet 362(9386):777–781
Zannad F, McMurray JJ, Krum H, van Veldhuisen DJ, Swedberg K, Shi H et al (2011) Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med 364(1):11–21
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Nochioka, K., Sakata, Y., Shimokawa, H. (2018). Combination Therapy of Renin Angiotensin System Inhibitors and β-Blockers in Patients with Heart Failure. In: Islam, M. (eds) Heart Failure: From Research to Clinical Practice. Advances in Experimental Medicine and Biology(), vol 1067. Springer, Cham. https://doi.org/10.1007/5584_2018_179
Download citation
DOI: https://doi.org/10.1007/5584_2018_179
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-78279-9
Online ISBN: 978-3-319-78280-5
eBook Packages: MedicineMedicine (R0)