
Abstract
Chronic kidney disease (CKD) often accompanies obstructive sleep apnea (OSA). A causative connection of the two disease entities is uncertain. However, eliminating OSA improves the prognosis of CKD patients. In the present study we examined a possible relationship between OSA and CKD, and whether there would be a mutual enhancing interaction in the severity of the two diseases. The study was of a retrospective nature and encompassed 382 patients over the period of 1 January 2014–30 June 2015. The OSA diagnosis was supported by a polysomnographic examination in 363 (95.0%) patients. Blood samples were taken for the determination of kidney function indices. The influence on OSA and CKD of comorbidities also was examined. We found a high probability of a simultaneous occurrence of OSA and CKD; with the odds ratio of 3.94 (95% CI 1.5–10.3%; p = 0.005). The 363 patients with OSA were stratified into 73 (20.1%) mild, 98 (27.0%) moderate, and 192 (52.9%) severe OSA cases according to the apnea-hypopnea index. CKD was found in 43 (58.9%) patients with mild OSA, 73 (74.5%) with moderate OSA, and 137 (71.4%) with severe OSA. Most OSA patients also suffered from hypertension and obesity. For comparison, CKD was detected in 7 (36.8%) out of the 19 patients without OSA (p < 0.003). We conclude that CKD develops significantly more often in patients with OSA than in those without it, and CKD frequency increases with the severity of OSA.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Obstructive sleep apnea (OSA) is a disease caused by repetitive breathing pauses during sleep, which trigger a subthreshold wake-up reaction due to a temporary shortage of oxygen to the organs. This results in various symptoms, such as pronounced daytime sleepiness, cardiovascular impairment, and other potentially serious secondary diseases (Chokorverty 2010). One of those disorders is chronic kidney disease (CKD). A number of studies have shown that OSA is particularly common in patients with advanced CKD (Fleischmann et al. 2010; Iseki et al. 2008). The original guidelines of the Kidney Disease Improving Global Outcomes (KDIGO) state that CKD should be defined based on a reduced glomerular filtration rate (GFR) or markers of kidney damage for at least three months. In addition, the cause of kidney disease, the magnitude of albuminuria, and the degree GFR impairment should be defined (Inker et al. 2014).
The cause-and-effect relationship and the nature of the potential association between the two diseases remains unclear. Thus, a thorough understanding of these two disease entities is essential. One possible feature linking the two diseases is increased arterial blood pressure. Enhanced blood pressure is one of the most important risk factors for the development of CKD (Chang et al. 2016; Sarnak et al. 2003). OSA often results in increased blood pressure (Meng et al. 2016), which could damage the kidneys with time (Archontogeorgis et al. 2016).
In the present study, we attempted to get an insight into the nature of the potential association between CKD and OSA. Further, we wished to examine the possibility of mutually enhancing interaction of disease severity, also taking into account the influence of comorbidities.
2 Methods
The implementation of the study was approved by the Ethics Committee of Witten/Herdecke University in Witten, Germany. Written informed consent by the study participants was waived due to a retrospective nature of the study. All personal information of the population investigated was removed prior to data analysis.
2.1 Study Design and Setting
We reviewed the data of all patients who were screened for OSA in the sleep laboratory of the Department of Pneumology of the HELIOS Clinic in Wuppertal of the Witten/Herdecke University in Germany in the period of 1 January 2014–30 June 2015. The HELIOS Clinic Wuppertal is the largest hospital in the Bergisch Land region lying in the state of North Rhine-Westphalia in Germany, with 967 beds and 26 departments. Each year, this hospital treats around 550 inpatients in the sleep laboratory. The data were collected in Excel file and evaluated after the completion of collection.
2.2 Obstructive Sleep Apnea (OSA)
There were 382 adult patients admitted to the sleep laboratory with a suspicion of having OSA during the study period who underwent a polysomnographic examination (Sleep Diagnostic System ALICE 4, Heinen + Löwenstein, Bad Ems, Germany), a gold standard for OSA diagnosis (Escourrou et al. 2015). OSA was confirmed in 363 (95.0%) patients according to standards of the WHO International Statistical Classification of Diseases (ICD G47.31) (WHO 2016). This classification defines OSA as 10 or more breathing pauses per hour of sleep, each lasting for 10 or more seconds. The patients displayed a number of other typical for OSA symptoms such as are loud snoring, headaches, daytime sleepiness and fatigue, impaired concentration, dry mouth, impotence, and depression (Pagel 2007). The severity of OSA was classified on the basis of apnea-hypopnea index (AHI), i.e., the number of apnea and hypopnea events per hour of sleep, calculated by dividing the number of events by the number of sleep hours. OSA was stratified into mild (AHI 5–14), moderate (AHI 15–29), and severe (AHI ≥30) form of disease (Ho et al. 2015). Comorbidities, other than CKD, and duration of a hospital stay were also compared among the four study groups. Nineteen patients with AHI of less than five, considered free of the disease, were assigned to the control group.
2.3 Chronic Kidney Disease (CKD)
Blood samples were collected in all patients to determine the indices of kidney function. CKD was defined as a slow, progressive loss of kidney function, with unspecific symptoms, for over three or more months (ICD N18.1–N18.5) according to the guidelines of Kidney Disease Improving Global Outcomes (KDIGO 2013). CKD was divided into six degrees of severity based on the estimated glomerular filtration rate (eGFR): Stage 1 (normal) – GFR above 90 mL/min/1.73 m2; Stage 2 (mildly decreased) – GFR of 60–89 mL/min/1.73 m2; Stage 3a (mildly to moderately decreased) – GFR of 45–59 mL/min/1.73 m2; Stage 3b (moderately to severely decreased) – GFR of 30–44 mL/min/1.73 m2; Stage 4 (severely decreased) – GFR of 15–29 mL/min/1.73 m2; and Stage 5 (kidney failure) – GFR less than 15 mL/min/1.73 m2 (WHO 2016).
The eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula for age, gender, race, and different doses of serum creatinine (Scr) for women and men: eGFR (mL/min/1.73 m2) = a × (Scr/b)c × (0.993)Age (Table 1) (National Kidney Foundation 2002). The serum creatinine (norm 0.5–1.1 mg/dL) was assessed using an Monovette® 4.7 mL blood collection system (Sarstedt AG & Co; Nümbrecht, Germany), including lithium heparin and an enzymatic colorimetric assay kit, and a COBAS® 6000 c501 analyzer (F. Hoffmann-La Roche Ltd; Mannheim, Germany).
2.4 Statistical Elaboration
Categorical data were expressed as percentages and continuous data as means ± standard deviations (SDs). Odds ratio (OR) was calculated to determine the likelihood of OSA and CKD coexistence. The 95% confidence intervals (CI) were calculated for OSA severity. Significance of gender differences and comorbidities was calculated using a 4 by 2 Chi2 test. One-way ANOVA for four independent samples was used to assess differences in age, duration of hospital stays, AHI, eGFR, and in the serum creatinine among the four study groups. A p-value <0.05 defined the statistically significant differences.
3 Results
Of the 382 patients screened for OSA, 73 (19.1%; 95%CI 15.2–23.1%) had mild OSA, 98 (25.7%; 95%CI 21.3–30.0%) had moderate OSA, 192 (50.3%; 95%CI 45.3–55.3%) had severe OSA, and 19 (5.0%; 95%CI 2.8–7.2%) did not have OSA (Table 2). Males comprised a total of 266 (69.6%) patients, and predominated in each study group (Table 2). There were no appreciable age differences among the four groups of patients, although younger patients tended to have less OSA. Significant differences were observed regarding the duration of a hospital stay; hospitalization was longer in patients with severe OSA. The OR for the coexistence of OSA and CKD in all study patients was 3.9 (95%CI 1.5–10.3%; p = 0.005). There was a significant difference in the mean eGFR, with lower values for the patients with severe OSA (Fig. 1 and Table 2). There were significantly fewer cases of OSA in patients with normal eGFR. However, no eGFR-dependent differences were found concerning OSA among the CKD stages in the groups studied. No difference was found in the mean serum creatinine value among the four study groups (Table 2).

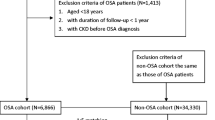
Number of patients with chronic kidney diseases calculated after estimated glomerular filtration rate (eGFR) in patients with obstructive sleep apnea (OSA) categorized according to the apnea-hypopnea index (AHI) and without OSA (AHI <5)
The most frequently observed comorbidities were hypertension and obesity, with rare cases of coronary artery disease, myocardial infarction, asbestosis, Ormond’s disease, sarcoidosis, urinary incontinence, hyperparathyroidism, hypothyroidism, chronic sinusitis, anxiety, stroke, dementia, depression, mania, multiple sclerosis, and polytoxicomania (Table 3).
4 Discussion
The majority of patients with OSA also suffered from CKD. In contrast, most patients without OSA had normal eGFR values. It can be said that the two diseases may be present together. A causative link between the two diseases has yet to be determined. It can also be assumed that OSA and CKD mutually negatively influence each other, although a few scientific studies have been carried out on this topic. One such study has shown that patients with OSA have an increased risk of developing CKD (Lee et al. 2015). While OSA is determined on the basis of pauses in breathing during sleep, CKD is a disorder in which there is an ongoing damage of renal function, and it is a major health problem worldwide (Kalamas and Niemann 2013). The relation between OSA and CKD is unclear. For this reason, screening kidney function indices values for the detection of CKD is essential for a proper treatment of OSA patients (Galbraith et al. 2016). In the present study, majority of OSA patients had a mild form of CKD, which is line with former findings that OSA patients have increased risk for the occurrence of early stages of CKD (Chu et al. 2016; Sim et al. 2009). Remarkably, the present study failed to demonstrate an increasing number of patients with OSA in advanced stages of CKD, but the most severe OSA coincided with the most severe CKD. The latter might have to do with a sometimes late detection of OSA. In contrast, another study has suggested that OSA is an independent risk factor for the advancement of CKD (Kanbay et al. 2012), which would form a plausibly causative link between the two diseases. This conclusion was based on the enhancing effect of hypopnea in OSA, which leads to oxygen desaturation during sleep, an increase of cytokine levels and insulin resistance. The same factors have been found to play a role in the progression of CKD in patients with OSA (Kanbay et al. 2012). Another study has shown an association between OSA severity and renal dysfunction, conspicuously even in patients without hypertension or diabetes (Chou et al. 2011). In the present study, the number of patients with diabetes was underrepresented in all four groups. Although the proportion of patients with severe OSA was largest, there was no real increase in the incidence of severe OSA alongside CKD severity. Accordingly, there was no association between OSA severity, assessed by AHI, and renal function impairment, assessed by eGFR.
As previously reported, sleep disorders are often observed in dialysis patients in advanced stages of renal disease. The prevalence of OSA in hemodialysis patients is as high as 24%, compared with the 16% in non-dialyzed patients with CKD (Ezzat and Mohab 2015). In the present study, proportion of dialysis patients was low at 1.3%, and all these patients had a severe OSA.
The relationship between OSA and hypertension has long since been known. There are several mechanisms that explain this relationship, primarily repeatable increases in sympathetic activity during apneic episodes. The main features of hypertension in OSA patients are high prevalence, diastolic and nocturnal predominance, and a frequent non-dipper status (Baguet et al. 2009). Therefore, hypertension accompanies OSA, particularly a long-lasting and severe OSA, as was also shown in the present study. Another study has also reported an increase in the frequency of hypertension based on OSA severity (Bayram et al. 2007). Further, in that study hypertension was found in about 37% of 209 OSA positive versus 7% of 54 OSA negative patients, which amounted to a remarkably significant difference. Obesity is another major factor in both OSA and CKD (McClellan and Plantinga 2013; Arens and Marcus 2004); the present findings confirmed a high percentage of the overweight among patients suffering from severe OSA. According to a study of Knorst et al. (2008), body mass index offers the best assessment of the effect of obesity on OSA severity.
A limitation of the present study was that only patients who had the clinical symptoms of OSA were investigated in the sleep laboratory. Patients with CKD, without OSA symptoms, were not examined. The effects on CKD of OSA treatment generally were not investigated either. Finally, a causative link between OSA and CKD was not determined as only a descriptive data evaluation was conducted.
In conclusion, coexistence of OSA and CKD is highly likely as GFR appreciably decreases with increasing OSA severity. CKD frequency increases with the severity of OSA. Hypertension and obesity are the most common comorbidities in OSA and CKD.
References
Archontogeorgis K, Nena E, Tsigalou C, Voulgaris A, Xanthoudaki M, Froudarakis M, Steiropoulos P (2016) Cystatin C levels in middle-aged patients with obstructive sleep apnea syndrome. Pulm Med 2016:8081723
Arens R, Marcus CL (2004) Pathophysiology of upper airway obstruction: a developmental perspective. Sleep 27:997–1019
Baguet JP, Barone-Rochette G, Pépin JL (2009) Hypertension and obstructive sleep apnoea syndrome: current perspectives. J Hum Hypertens 23:431–443
Bayram NA, Ciftçi B, Güven SF, Bayram H, Diker E (2007) Relationship between the severity of obstructive sleep apnea and hypertension. Anadolu Kardiyol Derg 7:378–382. (Article in Turkish)
Chang CP, Li TC, Hang LW, Lin JJ, Chou CY, Tsai JJ, Ko PY, Chang CT (2016) The relationships of sleep apnea, hypertension, and resistant hypertension on chronic kidney disease. Medicine (Baltimore) 95:e3859. doi:10.1097/MD.0000000000003859
Chokorverty S (2010) Overview of sleep and sleep disorders. Indian J Med Res 131:126–140
Chou YT, Lee PH, Yang CT, Lin CL, Veasey S, Chuang LP, Lin SW, Lin YS, Chen NH (2011) Obstructive sleep apnea: a stand-alone risk factor for chronic kidney disease. Nephrol Dial Transplant 26:2244–2250
Chu H, Shih CJ, Ou SM, Chou KT, Lo YH, Chen YT (2016) Association of sleep apnoea with chronic kidney disease in a large cohort from Taiwan. Respirology 21:754–760
Escourrou P, Grote L, Penzel T, Mcnicholas WT, Verbraecken J, Tkacova R, Riha RL, Hedner J, ESADA Study Group (2015) The diagnostic method has a strong influence on classification of obstructive sleep apnea. J Sleep Res 24:730–738
Ezzat H, Mohab A (2015) Prevalence of sleep disorders among ESRD patients. Ren Fail 37:1013–1019
Fleischmann G, Fillafer G, Matterer H, Skrabal F, Kotanko P (2010) Prevalence of chronic kidney disease in patients with suspected sleep apnoea. Nephrol Dial Transplant 25:181–186
Galbraith LE, Ronksley PE, Barnieh LJ, Kappel J, Manns BJ, Samuel SM, Jun M, Weaver R, Valk N, Hemmelgarn BR (2016) The see kidney disease targeted screening program for CKD. Clin J Am Soc Nephrol 11:964–972
Ho V, Crainiceanu CM, Punjabi NM, Redline S, Gottlieb DJ (2015) Calibration model for apnea-hypopnea indices: impact of alternative criteria for hypopneas. Sleep 38:1887–1892
Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, Kurella Tamura M, Feldman HI (2014) KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis 63:713–735
Iseki K, Tohyama K, Matsumoto T, Nakamura H (2008) High prevalence of chronic kidney disease among patients with sleep related breathing disorder (SRBD). Hypertens Res 31:249–255
Kalamas AG, Niemann CU (2013) Patients with chronic kidney disease. Med Clin North Am 97:1109–1122
Kanbay A, Buyukoglan H, Ozdogan N, Kaya E, Oymak FS, Gulmez I, Demir R, Kokturk O, Covic A (2012) Obstructive sleep apnea syndrome is related to the progression of chronic kidney disease. Int Urol Nephrol 44:535–539
KDIGO (2013) Kidney Disease: Improving Global Outcomes. CKD Work Group: Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 3:1–150
Knorst MM, Souza FJ, Martinez D (2008) Obstructive sleep apnea-hypopnea syndrome: association with gender, obesity, and sleepiness-related factors. J Bras Pneumol 34:490–496. (Article in Portuguese)
Lee YC, Hung SY, Wang HK et al (2015) Sleep apnea and the risk of chronic kidney disease: a nationwide population-based cohort study. Sleep 38:213–221
McClellan WM, Plantinga LC (2013) A public health perspective on CKD and obesity. Nephrol Dial Transplant 28(Suppl 4):iv37-42
Meng F, Ma J, Wang W, Lin B (2016) Obstructive sleep apnea syndrome is a risk factor of hypertension. Minerva Med 107:294–299
National Kidney Foundation (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39:S1–266
Pagel JF (2007) Obstructive sleep apnea (OSA) in primary care: evidence-based practice. J Am Board Fam Med 20:392–398
Sarnak MJ, Levey AS, Schoolwerth AC et al (2003) Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 108:2154–2169
Sim JJ, Rasgon SA, Kujubu DA, Kumar VA, Liu IL, Shi JM, Pham TT, Derose SF (2009) Sleep apnea in early and advanced chronic kidney disease: Kaiser Permanente Southern California cohort. Chest 135:710–716
WHO (2016) International Classification of Diseases (ICD). http://www.who.int/classification/icd/en/. Accessed on 22 Dec 2016
Conflicts of Interest
The authors declare no competing interests in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Yayan, J., Rasche, K., Vlachou, A. (2017). Obstructive Sleep Apnea and Chronic Kidney Disease. In: Pokorski, M. (eds) Clinical Management of Pulmonary Disorders and Diseases. Advances in Experimental Medicine and Biology(), vol 1022. Springer, Cham. https://doi.org/10.1007/5584_2017_35
Download citation
DOI: https://doi.org/10.1007/5584_2017_35
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-69544-0
Online ISBN: 978-3-319-69545-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)