
Abstract
In this chapter, radiological relevant injuries of the temporal bone are described and illustrated by selected images: fractures including nowadays used classifications, ossicular injuries and labyrinthine contusion. At the beginning, possibilities and limits of single radiological methods in the diagnostics of the temporal bone trauma are explained. Thereby, CT is still the imaging method of choice.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Compared to the rest of the body, the temporal bone is rarely affected in traumatic injuries. However, fractures of the temporal bone have been described as common (about 10 %) in patients with head trauma (Exadaktylos et al. 2003). Fractures of the temporal bone, which are also called laterobasal fractures, can occur without or with brain injuries. They result from blunt head injuries, which are caused by motor vehicle accidents (45 %), falls (31 %) and assaults (11 %) in the majority of cases (Saraiya and Aygun 2009).
On one side, not each temporal bone fracture presents with clinical symptoms (Turetschek et al. 1997), on the other side, the diagnosis is not uncommonly delayed in polytrauma because life-threatening injuries have priority and limit the clinical evaluation for signs of temporal bone trauma. Apart from the fractured bone, further structures may be more or less often injured in temporal bone trauma: tympanic cavity or labyrinth (hemotympanum, contusio labyrinthi), rupture of the drum, dural laceration, injuries of ossicles, the facial nerve and rarely great arterial or venous vessels.
Most of the temporal bone injuries do not require a surgical intervention. Only in the immediate facial nerve palsy an indication for rapid surgical management is given. Indications for operations in the interval are dislocations of ossicles, perilymphatic fistulas and cerebrospinal fluid (CSF) leaks that persist longer than 2 weeks. Patients with severe sensorineural hearing loss might be considered for a cochlear implant (Gladwell and Viozzi 2008; Turetschek et al. 1997).
Nowadays, CT is the modality of choice for the detection or exclusion of temporal bone fractures and associated complications. MRI is rarely applied for special questions.
In soft tissue injuries of the external ear, acute or chronic noise damage, imaging of the temporal bone plays a less important role.
1 Imaging Techniques
Basically, the imaging technique of temporal bone trauma does not differ from the technique described in Chap.2.
For subtle details, as for instance an injury of the ossicular chain, it is important to achieve a spatial resolution as best as possible in CT. This means a small slice thickness, small collimation in Multi-detector CT and high zoom (low field of view). According to one’s CT device these requirements cannot be exactly accomplished in polytrauma. Usually, injuries of the temporal bone are not life threatening. Temporal bone reconstructions are of secondary importance. The maximum slice thickness for optimal findings should not exceed more than one millimetre. Thin-sliced maximum intensity projections can be helpful in cases with difficult delineation of fracture lines.
Recently, Conebeam CT is achieved in otolaryngology too. Due to its high special resolution and low radiation exposure it is a valuable option for the isolated temporal bone trauma, but only for cases in which a soft tissue window and intravenous application of contrast medium is not needed.
In radiological studies MRI has been described as helpful in the assessment of an injured facial nerve, especially in the pre-operative localisation of the site of facial nerve injury if CT cannot provide this information (Kinoshita et al. 2001; Sartoretti-Schefer et al. 1997). Possible causes of facial nerve injury include oedema, intraneural haematoma, transsection, and bony impingement on the nerve (Gladwell and Viozzi 2008). Requirements for visualisation on MRI are thin-sliced high resolution T2-w, non-contrast and contrast enhanced T1-w sequences. From the clinician’s point of view the benefit of MRI in facial nerve injuries is challenged: often found oedema and enhancement of the entire course of facial nerve can obscure the exact location of the injury; the proof of a nerve transsection is hardly successful (Saraiya and Aygun 2009). Clinical findings of severity of facial nerve paralysis and timing of the palsy are considered as more helpful in determining treatment than MRI (Saraiya and Aygun 2009).
Although the verification of an intra-labyrinthine bleeding does not have a therapeutic consequence it can be required in legal actions. Bleedings are best seen as hyperintensity on thin-sliced non-contrast T1-w or FLAIR images in the methaemoglobin phase between the fourth day and the first month after the trauma.
2 Fracture Classification
Optimal classifications deliver a statement about the pathomechanisms, the extent and severity as well as the prognosis of a disease. They help in therapeutic decisions and facilitate the comparability of scientific studies. A classification fulfilling all these criteria does not exist for temporal bone fractures.
The so-called traditional classification distinguishes according to the course of the fracture in relation to the long axis of the petrous bone between longitudinal, transversal and mixed or complex fractures. This classification allows a conclusion about causative forces and certain clinical signs (Jäger et al. 1997; Kösling and Neumann 2010; Schuknecht and Graetz 2005; Turetschek et al. 1997). However, the association with complications (conductive or sensorineural hearing loss, facial nerve weakness, CSF leak) and prediction of prognosis has been described as poor (Ishman and Friedlan 2004). Distinguishing petrous from non-petrous involvement should demonstrate a better correlation with the occurrence of serious sequelae (Ishman and Friedlan 2004). A similar approach with comparable conclusions has been reported on a third classification dividing otic capsule-sparing and otic capsule-violating fractures (Little and Kesser 2006). Nonetheless, not all authors confirm the superiority of the newer classification (Rafferty et al. 2006).
In the clinical situation, the traditional classification is still the most commonly used classification of temporal bone fractures. With an extended interpretation of fracture lines all temporal bone fractures can be adequately classified. In the following the incidence, clinical and radiological appearance of these fractures as well as their typical complications will be described.
2.1 Longitudinal Fractures
With about 70 % longitudinal fractures are the most common fractures of the temporal bone. They result from laterally directed forces. The fracture runs more or less parallel to the long axis of the petrous bone (Figs. 1, 2). Not uncommonly, the middle ear is involved in this type. Longitudinal fractures can be further differentiated into an anterior and posterior subtype.

Longitudinal fracture of the anterior subtype. Fall on the head, after 3 days an incomplete peripheral facial nerve palsy has developed. Fracture lines through the anterior squamous portion of the temporal bone (white arrows) and opacifications (stars) in the mastoid and tympanic cavity especially at the fossa geniculi as expression of bleedings. a, b CT axial; c, d CT coronal

Longitudinal fractures of the posterior subtype. Fall in alcoholised condition (a, b). A cupboard fell on the head (c). Fracture lines through the mastoid (white arrows in a and c) and occipital bone (dotted arrow in a), intracranial air (white dotted arrows in b) and infratentorial subdural haematoma (black dotted arrows in b). The prominent singular canal (black dotted arrow in c) should not be confused with a fracture. a CT sagittal; b brain CT axial; c CT axial
Compared to transverse fractures facial nerve palsy occurs more seldom (10–20 %). Mostly, it is delayed, incomplete and transitory, caused by pressure of an extraneural haematoma on the nerve. Dural lacerations with a CSF leak may occur, but most leaks close spontaneously. As late complication the development of a cholesteatoma is observed. (Gladwell and Viozzi 2008; Jäger et al. 1997; Kösling and Neumann 2010; Rafferty et al. 2006; Schuknecht and Graetz 2005; Turetschek et al. 1997).
Clinical findings:
-
Palpable step in the external auditory canal
-
Perforation of the drum
-
Haemtotympanum
-
Conductive hearing loss
-
Otoliquorrhea; in intact drum ‘false rhinoliquorrhea’ (drainage via the tuba auditiva)
-
Peripheral facial nerve palsy.
Radiological findings:
-
Anterior subtype (more common): fracture line(s) through the anterior and/or middle squamous portion of the temporal bone, the anterior wall of the external auditory canal, the tegmen tympani, toward the geniculate ganglion and possibly along the anterior border of the petrous portion or through the tuba auditiva (Fig. 1), rarely extend into the central skull base
-
Posterior subtype (less common): fracture line(s) through the posterior squamous portion of the temporal bone or through the mastoid process, the posterior wall of the external auditory canal, the second knee of the facial nerve or its mastoid portion and may extend to the surrounding of the foramen lacerum and seldom into the jugular foramen (Fig. 2)
-
Attendant signs in both subtypes: opacifications of the mastoid, cavum tympani and external auditory canal—sometimes with fluid levels as expression of bleedings (Figs. 1, 2); injuries of ossicles (see below); occasionally involvement of the carotid canal; rarely intracranial air as a sign for an open skull base fracture (Fig. 2b).
Differential diagnosis:
Small canals, fine sutures (pseudofractures) (Fig. 2c)—comparison with the contralateral side (when it is unaffected) helps in the differentiation.
Important points:
-
Knowledge of the clinical findings supports the radiological assessment
-
Analyze the roof of the middle ear and mastoid carefully on coronal reconstructions; traumatic gaps may occur with CSF leaks and can lead to cephaloceles and/or meningitis (Fig. 3)
Fig. 3 
Post-traumatic meningoencephalocele. Head trauma many years ago. On CT a broad gap in the roof of the mastoid is visible (arrow in a). MRI demonstrates the prolapse of brain into the mastoid (star). a CT coronal; b MRI T2-w coronal. (b with permission from Kösling and Neumann (2010))
-
The canal of the ICA and facial nerve has to be analysed carefully, but not each fracture line is linked with an injury of the vessel and nerve, respectively
-
Dislocated fragments of the carotid canal should implicate a non-invasive imaging of cerebral arteries or DSA (depending on the available technique, no unique recommendations)
-
Fracture lines through the jugular foramen are extremely rarely accompanied by venous complications (Saraiya and Aygun 2009).

2.2 Transversal Fractures
Transversal fractures arise from frontal or occipital directed forces. They are less common (about 20 % of all temporal bone fractures). Fractures pass off perpendicular to the long axis of the petrous bone and can be linked with a damage of the inner ear (Figs. 4, 5). Transversal fractures can be further differentiated into a lateral and medial subtype.

Transversal fracture of the lateral subtype. Traumatic brain injury of first degree. Fracture lines (black arrows) through the otic capsule with involvement of the labyrinth, the fossa geniculi (white dotted arrow in b), the oval window (white dotted arrow in c), the jugular fossa (arrow in d) as well as a described opacification in the antrum. The occipitomastoid suture (white dotted arrows in g) should not be confused with a fracture. a–d CT axial; e CT coronal; f CT coronal thin-sliced maximum intensity projection; g CT axial thin-sliced maximum intensity projection

Transversal fracture of the lateral subtype. Motor vehicle accident, immediate peripheral facial nerve palsy. On CT fracture lines (white arrows) through the labyrinth including the jugular foramen and subtle opacifications around the tympanic segment of the facial nerve (dotted white arrow in a). On MRI an enhancement of the tympanic segment of the facial nerve is visible (dotted white arrow in c). a, b CT axial; c MRI T1-w with contrast medium, axial. (a, c with permission from Kösling and Neumann (2010))
A mostly immediate and complete facial nerve palsy, which is caused by a direct damage of the nerve, is found in about half of cases. From the lateral subtype, labyrinthine fistulas may result. Fibrosing and ossification of the labyrinth are possible serious sequelae (Fig. 6) (Gladwell and Viozzi 2008; Jäger et al. 1997; Kösling and Neumann 2010; Rafferty et al. 2006; Schuknecht and Graetz 2005; Turetschek et al. 1997).

Sequelae of transversal fracture. Deafness after accident at work. On CT fracture lines (white arrows) and partial ossification of the labyrinth (dotted black arrows) are visible—on MRI there is a partial signal loss in the labyrinth (white dotted arrow). a CT axial; b CT coronal; c MRI T2*-w axial
Clinical findings:
-
Sensorineural hearing loss or deafness
-
Damage of the vestibular organ (vertigo, vomiting and spontaneous nystagmus to the contralateral side)
-
Peripheral facial nerve palsy.
Radiological findings:
-
Lateral subtype (more common): fracture line(s) laterally of the internal auditory canal through petrous bone often with involvement of the labyrinth, the medial wall of the tympanic cavity (windows may be affected) and the facial nerve (predominately the fossa geniculi or labyrinthine segment, rarely the tympanic segment) (Figs. 4, 5).
Attendant signs: pneumolabyrinth (Fig. 4a–c) and fluid level in the sinus tympani as an indirect sign of a labyrinthine fistula; opacifications of tympanic cavity and mastoid according to haemorrhage (Fig. 4a–c); intracranial air; rarely injuries of ossicles; inclusion of jugular foramen (Fig. 4d)
-
Medial subtype (rare): fracture line from the posterior cranial fossa through the internal auditory canal to the middle cranial fossa (foramen spinosum and ovale may be included), in severe injuries to the anterior skull base and midface
-
Attendant signs in both subtypes: possibly inclusion of the carotid canal.
Differential diagnosis:
Small canals, fine sutures (pseudofractures) (Fig. 4g)—comparison with the contralateral side (when it is unaffected) helps in the differentiation.
Important points:
-
Knowledge of the clinical findings supports the radiological assessment
-
The canal of the ICA and facial nerve has to be analysed carefully, but not each fracture line is linked with an injury of the vessel and nerve, respectively
-
Dislocated fragments of the carotid canal should implicate a non-invasive imaging of cerebral arteries or DSA (depending on the available technique, no uniform recommendations)
-
Fracture lines through the jugular foramen are extremely rarely accompanied by venous complications (Saraiya and Aygun 2009)
-
MRI can provide additional information regarding a facial nerve injury (see Sect. 1) (Fig. 5c)
-
Persistent severe sensorineural hearing loss after trauma may be an indication for cochlear implant.
2.3 Mixed Fractures
Mixed or complex fractures show characteristics of longitudinal as well as transversal fractures (Fig. 7). They are seen more frequently in severe head injuries and can be combined with considerable dislocation or impression of fragments. (Kösling and Neumann 2010; Rafferty et al. 2006; Turetschek et al. 1997).

Complex fractures. Open traumatic brain injury after fall (a–d). Polytrauma (e, f). In the first case (a–d) longitudinal (white arrows) and transversal (dotted black arrows) fracture lines can be recognised. In the second case (e, f) there is an impression fracture (white arrows). a–c, e, f CT axial; d CT coronal
3 Ossicular Injuries
Blows to the temporal, occipital or parietal region are the main mechanisms of ossicular injuries. Often, the ossicular chain is damaged in longitudinal or mixed fractures of the temporal bone (Fig. 8). Other causes as transverse fractures, explosion trauma and direct mechanical impairment are uncommon.

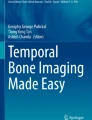
Ossicular injuries. a Incudomalleolar joint separation (white dotted arrow) and complex temporal bone fracture (black arrows). b Incudostadpedial joint separation (white dotted arrow) and longitudinal temporal bone fracture (black arrows). c Stapediovestibular dislocation (black dotted arrow) and pneumolabyrinth (arrowhead). d Dislocation of the incus with y-sign, fracture of malleus (black dotted arrow) and longitudinal temporal bone fracture (white arrow) causing a gap in the roof of tympanic cavity. The comparison with the contralateral side is helpful. a–c CT axial; d CT coronal. (b, c with permission from Kösling and Neumann (2010))
Mainly ossicular injuries occur as dislocations; fractures are rarely found. Due to a diverse ligamentary attachment and orientation the single ossicles are affected with different frequency. (Kösling and Neumann 2010; Lourenco et al. 1995; Meriot et al. 1997).
Clinical findings:
-
Persistent conductive (or rarely mixed) hearing loss after trauma
-
Rarely vertigo and/or tinnitus
-
Rarely rupture of tympanic membrane.
Radiological findings:
-
Incudomalleolar joint separation (common): gap between the body of incus and head of malleus, best seen on axial images (Fig. 8a)
-
Incudostapedial joint separation (common): widening of the distance between the head of the stapes and the lenticular process of the incus, best seen on axial images (Fig. 8b)
-
Dislocation of the incus (due to weak ligamentary attachment more common than a dislocation of malleus): Y-sign (Lourenco et al. 1995) of the incudomalleolar complex on coronal images (Fig. 8d)
-
Dislocation of the incudomalleolar complex: in intact incudomalleolar joint the incus and malleus may dislocate together in different direction, partly there is a consecutive rupture of the incudostapedialjoint
-
Stapediovestibular dislocation (rare): dislocation of the stapes into vestibulum, often accompanied by a perilymphatic fistula (Fig. 8c)
-
Fractures of single ossicles (very rare): especially fractures of the stapes are hardly detectable on CT (Fig. 8d).
Differential diagnosis:
-
Normal finding (for avoidance best spatial resolution is needed)
-
Malformation (other clinical situation).
Important points:
-
In haemtotympanum the assessment of the stapes may be aggravated
-
Comparison with the contralateral side (when it is unaffected) helps in the detection of an incorrect position of ossicles
-
The oval window region has to be analysed carefully
-
Air in the labyrinth is an indirect sign of a perilymphatic fistula (Fig. 8c)
-
Tympanoscopy is the golden standard for the assessment of the ossicular chain; with optimised CT technique or Conebeam CT most, but not all ossicular injuries can be diagnosed non-invasively.
4 Contusio Labyrinthi
The contusio labyrinthi is a traumatic lesion of the inner ear of different degree without a temporal bone fracture. On the basis of CT the diagnosis can be made only indirectly if CT is negative regarding fractures and the patient has typical clinical findings of a disturbed inner ear function. Opacifications of pneumatised areas can be seen occasionally.
A direct verification is enabled through MRI by demonstration of an intra-labyrinthine bleeding (see Sect. 1) (Fig. 9). Less common as in transverse fractures, fibrosing and ossification of the labyrinth can develop (Jäger et al. 1997; Kösling and Neumann 2010).

Contusio labyrinthi. Deafness after accident at work, 4 weeks after trauma. Increased signal intensity of the cochlea (arrow). MRI T1-w without contrast medium, axial. (with permission from Kösling and Neumann (2010))
References
Exadaktylos AK, Sclabas GM, Nuyens M et al (2003) The clinical correlation of temporal bone fractures and spiral computed tomographic scan: a prospective and consecutive study at a level I trauma center. J Trauma 55:704–706
Gladwell M, Viozzi C (2008) Temporal bone fractures: a review for the oral and maxillofacial surgeon. J Oral Maxillofac Surg 66:513–522
Ishman SL, Friedlan DR (2004) Temporal bone fractures: traditional classification and clinical relevance. Laryngoscope 114:1734–1741
Jäger L, Strupp M, Brandt T et al (1997) Imaging of labyrinth and vestibular nerve. Nervenarzt 86:443–458
Kinoshita T, Ishii K, Okitsu T et al (2001) Facial nerve palsy: evaluation by contrast-enhanced MR imaging. Clin Radiol 56:926–932
Kösling S, Neumann K (2010) Schläfenbein und hintere Schädelbasis. Traumatisch bedingte Erkrankungen. In: Kösling S, Bootz F (eds) Bildgebung HNO-Heilkunde. Springer, Berlin, pp 59–69
Little SC, Kesser BW (2006) Radiographic classification of temporal bone fractures. Arch Otolaryngol Head Neck Surg 132:1300–1304
Lourenco MTC, Yeakley JW, Ghorayeb BY (1995) The “Y” sign of lateral dislocation of the incus. Am J Otol 16:387–392
Meriot P, Veillon F, Garcia JF et al (1997) CT appearances of ossicular injuries. RadioGraphics 17:1445–1454
Rafferty MA, Mc Conn Walsh R, Walsh MA (2006) A comparison of temporal bone fracture classification systems. Clin Otolaryngol 31:287–291
Saraiya PV, Aygun N (2009) Temporal bone fractures. Emerg Radiol 16:255–265
Sartoretti-Schefer S, Scherler M, Wichmann W et al (1997) Contrast enhanced MR of the facial nerve in patients with posttraumatic peripheral facial nerve palsy. Am J Neuroradiol 18:1115–1125
Schuknecht B, Graetz K (2005) Radiologic assessment of maxillofacial, mandibular, and skull base trauma. Eur Radiol 15:560–568
Turetschek K, Czerny C, Wunderbaldinger et al (1997) Temporal bone trauma and imaging. Radiologe 37:977–982
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Kösling, S., Noll, A. (2013). Temporal Bone Trauma. In: Lemmerling, M., De Foer, B. (eds) Temporal Bone Imaging. Medical Radiology(). Springer, Berlin, Heidelberg. https://doi.org/10.1007/174_2013_908
Download citation
DOI: https://doi.org/10.1007/174_2013_908
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-17895-5
Online ISBN: 978-3-642-17896-2
eBook Packages: MedicineMedicine (R0)