
Abstract
The use of Immunosuppression has led to the tremendous improvement in graft survival. However, immunosuppressants have been found to cause a variety of metabolic derangements including but not limited to: insulin resistance and diabetes, hyperlipidemia, hypertension, and weight gain after transplantation. This combination of metabolic risk factors may be associated with increased cardiovascular disease (Grundy et al., Circulation 112(17):2735, 2005). In addition many transplant recipients may have many of these risk factors pre-transplant that are exacerbated by immunosuppression. These facts emphasize the need for rigorous follow-up and management of these risk factors post-transplant.
The most common immune suppressant regimens may include different combinations of these agents: Corticosteroids, Calcineurin inhibitors (CNIs), Mammalian Target of Rapamycin (mTOR) Inhibitors, Antimetabolite.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The cornerstone of heart transplant recipient care comes in the form of meticulous management of immune modulation to ensure immunologically acceptance of the donor organ. Recipient survival requires an equilibrium between acute rejection and the adverse effects from chronic immunosuppression. In this chapter, we will discuss immunosuppression’s effects on nephrotoxicity, hypertension, and metabolic consequences that transplant recipients might face.
2 Immunosuppression and Nephrotoxicity
There are many challenges in managing immune modulation. A significant long-term consequence of immunosuppression is nephrotoxicity. The nephrotoxicity and significant progression of renal dysfunction resulting from these agents has proven to be an Achilles’ heel in heart transplantation. Based on the ISHLT registry data, between the years January 1995 to June 2017, 6.7% of transplant survivors experienced severe renal dysfunction (defined as serum creatinine >2.5 mg/DL, chronic dialysis, or renal transplantation) within the first year, as well as observed in 15.7% of survivors within 5 years, and 22.3% within 10 years (Khush et al. 2019). In the current era, freedom from severe renal dysfunction has improved compared to the previous era (1995–2004), however severe renal dysfunction still provides a significant impact on survival to 1 year. There are many factors that contribute to development of severe renal dysfunction after transplant. The recipient’s pre-transplant creatinine plays a role in which there is an inflection point in which the hazard ratio increases for serum creatinine >1.1 mg/dL. In this section we will be exploring in more detail each of the immunosuppressant classes and their effects on renal function (Khush et al. 2019).
2.1 Corticosteroids
Corticosteroids or glucocorticoids are some of the most widely used immunosuppressant agents. They are non-specific anti-inflammatory agents that work at the level of the nucleus to augment expression of pro-inflammatory proteins. Corticosteroids are associated with many adverse effects with long-term use, however there is no reported direct nephrotoxicity associated with their use.
2.2 Calcineurin Inhibitors
Calcineurin inhibitors have remained at the cornerstone of maintenance immunosuppression since the early 1980s. The current available calcineurin inhibitors (CNIs) are cyclosporine (CsA; Sandimmune, Gengraf, or Neoral) and tacrolimus (Tac; Prograf). Both cyclosporine and tacrolimus block calcium activated calcineurin. Specifically, cyclosporine binds to cyclophilin and tacrolimus to the FK binding protein-12. Each drug and their respective immunophilin binds to calcineurin. Calcineurin is a phosphatase that dephosphorylates multiple molecules including nuclear factor of activated T cells (NFAT), which will subsequently bind premotor regions on several cytokine genes causing up-regulation. Cyclosporine and tacrolimus both inhibit calcineurin, and thus blunt the upregulation of the cytokines including interleukin-2 (IL-2). Additionally, cyclosporine also stimulates transforming growth factor beta (TGFB) production which also contributes to its immunosuppressive effects (Shin et al. 1998).
Cyclosporine has been part of the cornerstone of immunosuppression since the early 1980s. Over the years, different formulary have existed including a modified microemulsion formulation of cyclosporine which demonstrated a greater bioavailability and more predictable pharmacogenetics and oil-based preparations (Cooney et al. 1998). Nephrotoxicity is a well-known associated consequence of cyclosporine use. Nephrotoxicity with cyclosporine is a dose-related effect that can either be acute or chronic resulting in arteriolar sclerosis and tubular interstitial fibrosis. In rare instances cyclosporine may also manifest as a hemolytic uremic syndrome (Valantine 2000).
Tacrolimus, formally known as FK506, is the other calcineurin inhibitor that is widely used. There have been a number of studies comparing tacrolimus to cyclosporine, in both the oil-based and micro emulsion formularies. Tacrolimus was compared to oil based cyclosporine, there were similar patient and allograft survival, however the incidence of moderate to severe cellular rejection at 6 months was significant lower in the tacrolimus group compared to the micro-emulsion cyclosporine group (Taylor et al. 1999; Reichart et al. 2001; Grimm et al. 2006; Kobashigawa et al. 2006).
In a cohort study of solid organ transplants, including heart, liver, and lung in the USA, the overall incidence of CKD was 60% in the cyclosporine group and 20% in the tacrolimus group. At a median follow-up of 36 months, 17% had developed CKD stage IV or greater. The risk of CKD increases over time with all of the solid organ transplant and was associated with a 4.6 fold increase in risk of death compared to those without CKD. Twenty-nine percent of patients went on to develop end-stage renal disease requiring renal replacement therapy. Risk factors had included older age, lower pretransplant GFR, female sex, postop AKI, baseline history of diabetes and hypertension as well as hepatitis C viral infection (UTD 12, 14). Other risk factors include concomitant nephrotoxic drug use such as nonsteroidal anti-inflammatory drugs, as well as drugs that inhibits the cytochrome P450 3A4/5 thereby increase exposure to CNI metabolites and drugs that inhibited P glycoprotein mediated efflux of TNI from tubular epithelial cells causing an increase in local renal exposure (UTD 31). Polymorphisms in the genes encoding for CYP 3 A4/5 and P glycoprotein (ABCB1) will also affect the risk of nephrotoxicity (UTD 31).
Both acute and chronic nephrotoxic effects are generally similar with cyclosporine and tacrolimus (UTD 15). A lot of data in this field comes from renal transplant recipient and involves cyclosporine given the wide availability. Acute calcineurin inhibitor nephrotoxicity is due to vasoconstriction of the afferent and arterial, thereby causing a reduction in renal blood flow and glomerular filtration rate (UTD 36). Although the exact mechanism is still unclear, there seems to be a substantial impairment of endothelial cell function with enhanced release of vasoconstrictors like endothelin and thromboxane (UTD 36). Renal plasma flow and GFR reduction correlate with the dose and peak cyclosporine level, which may be associated with increased urinary excretion of endothelin, which decreases when trough drug levels are reached (UTD 38). This increase in vascular resistance may be reflected by an increase in plasma creatinine concentration as well as systemic hypertension (UTD 2). This vasoconstriction prevents and delays recovery from early AKI associated with hypoperfusion and ischemia. It is also possible that these episodes of renal ischemia may contribute to a chronic cyclosporine nephrotoxicity.
In addition to the aforementioned effects on renal function, there are a number of electrolyte and metabolic abnormalities that may result from CNI use. These include hyperkalemia, non-anion gap metabolic acidosis, hypomagnesemia, hyperkalemia, hypophosphatemia, hyperuricemia and gout (UTD 20, 21, 67, 68).
CNI use may cause an elevation in plasma potassium concentration by reducing the efficiency of urinary potassium excretion by decreasing the activity of the renin-angiotensin-aldosterone system and by impairing tubular responsiveness to aldosterone (UTD 69, 70). There are some in vitro studies suggesting that cyclosporine may directly impair the function of the cells in the cortical collecting tubule, with decreased activity of the NA–K–ATPase pump with inhibition of the luminal potassium channel and thereby increasing chloride reabsorption (UTD 70). Tacrolimus has a similar inhibitory effect on the Na–K–ATPase pump (UTD 73).
Cyclosporine can cause tubular injury thereby impairing acid excretion as well as decreasing aldosterone activity with suppression of ammonia excretion by the concomitant hyperkalemia (UTD 2, 70). Cyclosporine may also cause urinary phosphate wasting, as well as abnormalities in calcium and magnesium reabsorption resulting in hypophosphatemia, hypomagnesemia, and hypocalcemia respectively (UTD 2, 78). The CNI effects on glomerular and tubular function can also lead to a decrease in uric acid excretion leading to hyperuricemia (UTD 67).
As mentioned, CNI nephrotoxicity can manifest either as an acute or chronic injury. Other renal effects include tubular dysfunction and rarely a thrombotic microangiopathy which can also lead to acute renal loss. The majority of data published on this topic comes from cyclosporine, however there are similar patterns of renal disease described and tacrolimus, thus implying a drug class effect. (UTD 2–5).
One of the best ways to prevent chronic calcineurin inhibitor induced nephrotoxicity is to minimize the patient’s exposure to CNI agents, and potentially replace them with non-nephrotoxic immunosuppressive agents. Strategies for minimizing CNI exposure are in the section below. There has been a great deal of interest in finding other agents to minimize the nephrotoxic effects of CNI. These include cold fish oil (UTD 85, 86, 90), renin angiotensin system inhibitors, calcium channel blockade, thromboxane synthesis inhibitors (UTD 111), and pentoxifylline (UTD 110), however agents have either unproven or no benefit.
There are some small animal studies that showed ACE inhibitors and angiotensin receptor blockers can prevent cyclosporine-induced interstitial fibrosis and improve renal function, however studies in humans have not demonstrated a clear benefit (UTD 100–102) Similar findings and interval studies are suggestive that aldosterone antagonism with spironolactone may be beneficial, however there are no human studies to support this. (UTD 105).
Unlike RAS inhibition, calcium channel blockers in animal and human data in renal transplants suggest that concomitant administration with cyclosporine may be protective by minimizing the renal vasoconstriction (UTD 92). Although there may be some small benefit in renal vasoconstriction initially in renal transplant recipients, there is no proven benefit in long-term outcomes of graft survival, or chronic vascular and tubulointerstitial injury. There has also been an inability to demonstrate a better outcome in protecting against kidney injury with calcium channel blockers versus ACE inhibitors (UT 50).
2.3 Antimetabolites
The antiproliferative agents otherwise known as antimetabolite provide an additional component of the backbone of maintenance immunosuppression. Their fax can be found by interference of the synthesis of nucleic acids, preventing the proliferation of T and B lymphocytes. The two most commonly encountered antimetabolites in heart transplantation include azathioprine and mycophenolic acid.
2.4 Azathioprine
Azathioprine (Imuran), once hydrolyzed and converted to its purine analog thio-inosine-monophosphate, becomes incorporated into DNA inhibiting the mitotic and proliferative function of activated T and B lymphocytes. This drug used to be a common addition to a calcineurin-based regimen for maintenance immunosuppression. Side effects include leukopenia, hepatotoxicity, and pancreatitis amongst others, however nephrotoxicity is not one of them.
2.5 Mycophenolic Acid
In this current era, mycophenolic acid has replaced azathioprine as the preferred antimetabolite agent. The two major forms are mycophenolate popliteal (MMF; CellCept) or mycophenolate sodium (Myfortic). Mycophenolate mofetil also is a prodrug requiring hydrolysis to its active form of mycophenolic acid (MPA), while mycophenolate sodium (EC–MPS) is an enteric-coated, delayed release salt of mycophenolic acid. In its mycophenolic acid form it becomes a reversible inhibitor inosine monophosphate dehydrogenase, preventing de novo synthesis of guanine nucleotide, and thus selectively inhibiting T and B lymphocyte proliferation. There are a number of benefits to mycophenolic acid over azathioprine including less bone marrow suppression, amongst others that will be discussed in other parts of this book. Both forms of mycophenolic acid discussed are not nephrotoxic.
2.6 Proliferation Signal Inhibitors/Mammalian Target of Rapamycin (mTOR) Inhibitors
The fourth class of immunosuppressive agents include the proliferation signal inhibitors (PSI) otherwise known as the mammalian target of rapamycin (mTOR) inhibitors. There are a few indications that have risen to the top in which PSI based regimens have proven ineffective over the more conventional maintenance therapies.
The two drugs in this category of medications include sirolimus (Rapamune) and everolimus (Zortress). Similar to tacrolimus they bind to the FK binding protein, but rather than blocking calcineurin dependent T-cell activation, there is inhibition of a protein kinase in the cytoplasm called the mammalian target of rapamycin (mTOR). TOR phosphorylases proteins that regulate the cell cycle, thus it plays a critical role in transmission of the IL-2 mediated growth and proliferation of T and B lymphocytes. The activation of TOR also plays a role in the proliferation of smooth muscle and endothelial cells and may explain some of the benefits and prevention of graft atherosclerosis and indication of tumor growth in animal models (Heitman et al. 1991; Guba et al. 2002; Poston et al. 1999). Inhibition of mTOR will inhibit T and B-cell proliferation in response to cytokine signaling.
Sirolimus or Rapamune has been compared to a number of standard immunosuppressive agents, notably, as an alternative to azathioprine in a prospective, open label, randomized trial in which there was a lower proportion of moderate to severe acute cellular mediated rejection episodes within 6 months and the sirolimus group out as well has a reduction in cardiac allograft vasculopathy at both 6 months and 2 years (Kirklin et al. 1994). This made sirolimus an attractive agent. Everolimus (Zortress) is an analog of sirolimus, with the main difference being everolimus’s better bioavailability with a shorter terminal half-life (30 h), compared to sirolimus (60 h) (Klawitter et al. 2015).
Compared to CNIs, PSIs are unique and that they inherently have no nephrotoxicity effect but can potentiate the efficacy and nephrotoxicity of CNIs. When a CNI + PSI-based strategy is used, a dose reduction in the CNI of at least 25% is recommended. Sirolimus and everolimus have similar toxicity profiles overall, and though no head-to-head comparison had been made between the two drugs (Keogh et al. 2004).
2.7 Induction Therapy
Induction therapy is a widely available treatment strategy in which early intense immunosuppressant agents are administered in the early post-op period, with a goal of providing immediate immunomodulation. Approximately only 40–50% of heart transplant programs currently employed this strategy of upfront intense immunomodulation when risk of allograft rejection is the highest (Khush et al. 2019). There are a few different immunogenic targets which can be utilized, such as monoclonal antibody against IL-2 receptor antagonism (currently available agent, basiliximab (Simulect)), polyclonal anti-thymocyte antibodies (ATGAM-horse derived lymphocyte immune globulin or Thymoglobulin-rabbit derived lymphocyte immune globulin) and antibodies against the CD52 antigen (currently available agent, Alemtuzumab (Campath-1H)). Induction strategies may benefit those who are at high risk for severe rejection, such as African-American patients, younger patients, those with high levels of preformed antibodies, and in cross matches with a high number of HLA mismatches (Rosenberg et al. 2005). Induction allows for a secondary advantage of delaying initiation or lower doses of other immunosuppressant agents, namely those with significant adverse effects such as those that induce nephrotoxicity or metabolic sequelae (Cantarovich et al. 2004; Higgins et al. 2005). In a small study from Cantarovich et al., they studied postop renal dysfunction in heart transplant recipients receiving ATG induction, which the authors results suggested that delaying cyclosporine initiation post induction had comparable survival at 1 year, with a reduction in post-op renal dysfunction (Higgins et al. 2005). In a Cochrane review from Penninga et.al, reviewing 22 randomized control trials that utilize T-Cell antibody, the authors concluded that there was no clear benefit or harm associated with use of any kind of T-cell antibody induction compared to no induction, with a possible reduction in acute rejection with IL-2 RA compared to no induction. Overall there was no significant difference found for any comparison group for mortality, or adverse events including significant differences in renal function (Penninga et al. 2013).
3 Immunosuppression: Hypertension and Metabolic Disease
The use of Immunosuppression has led to the tremendous improvement in graft survival. However, immunosuppressants have been found to cause a variety of metabolic derangements including but not limited to: insulin resistance and diabetes, hyperlipidemia, hypertension, and weight gain after transplantation. This combination of metabolic risk factors may be associated with increased cardiovascular disease (Grundy et al. 2005). In addition many transplant recipients may have many of these risk factors pre-transplant that are exacerbated by immunosuppression. These facts emphasize the need for rigorous follow-up and management of these risk factors post-transplant.
The most common immune suppressant regimens may include different combinations of these agents: Corticosteroids, Calcineurin inhibitors (CNIs), Mammalian Target of Rapamycin (mTOR) Inhibitors, Antimetabolite.
3.1 Corticosteroids
Corticosteroids have been an integral part of immunosuppression regimens since the beginnings of clinical transplantation (Bell et al. 1971). They are usually started at high doses and titrated off over a variable time frame ranging from 1 to 6 months. Steroids can lead to insulin resistance, hypertension, hyperlipidemia, and weight gain due to enhanced appetite. The steroid effect on glucose levels is dose dependent and generally improves as steroids are tapered off. Steroids stimulate insulin resistance by decreasing beta cell insulin production and increase in gluconeogenesis and a decrease in glucose utilization (Watt 2011). Steroids are also thought to cause hypertension due to sodium and water retention due to the mineralocorticoid effect and by vasoconstriction due to the glucocorticoid effect on smooth muscle (Goodwin et al. 2008). Long-term use of steroids is also associated with hyperlipidemia. Steroids can lead to an increase in both low-density lipoprotein (LDL) and high-density lipoprotein (HDL) levels and have a minimal effect on triglycerides. The mechanism by which LDL increase takes place is thought to involve the increased production of very low-density lipoprotein (VLDL) cholesterol and increased activity of 3-hydroxy-3-methyl-glutaryl-coenzyme A, and decreased LDL receptor function. The increase in HDL is attributed to the increase in lipoprotein lipase activity and a decrease in hepatic triglyceride lipase activity (Lau et al. 2010).
3.2 Calcineurin Inhibitors (CNIs)
CNIS are associated with hypertension, hyperlipidemia, and impaired glucose metabolism (Moien-Afshari et al. 2003). Tacrolimus (Tac) has a lower incidence of hypertension and hyperlipidemia when compared to cyclosporine (CsA). However Tac has been linked to higher levels of new onset diabetes and impaired glucose intolerance (Pham et al. 1996; Reichart et al. 1998; Eisen and Ross 2004).
CNIs have been thought to cause hyperlipidemia through decreasing bile acid synthesis from cholesterol and reducing cholesterol transport into the intestines leading to increased serum levels. In addition, cyclosporine can bind to LDL cholesterol receptor leading to the increase level of circulating LDL cholesterol (Muñoz 1995). The diabetogenic effects of cyclosporine and tacrolimus include toxic effects on pancreatic B cells which were more prominent with CsA, and inhibition of basal insulin secretin which is more prominent with TAC in the acute phase. Taken together these effects result in reduced insulin synthesis, secretion, and increased insulin resistance (Øzbay et al. 2011).
The cause of hypertension secondary to CNIs is multifactorial. Systemic vasoconstriction combined with a decrease in glomerular filtration and enhanced sodium reabsorption in the renal tubules are thought to be the main culprits (Watt 2011). This vasoconstriction is thought to be related to the impaired balance of vasodilatory mediators (prostacyclin and nitric oxide) vs vasoconstricting mediators (endothelin, thromboxane A2, and the renin-angiotensin system) (Vaziri et al. 1998).
For those maintained on CsA considerations should be given when switching over to Tac if hyperlipidemia and hypertension are an issue. In addition, exposure to CNIs should be minimized to the lowest optimal level needed to maintain allograft to avoid the metabolic consequences discussed.
Because of all the potential metabolic side effects of both agents, efforts to minimize calcineurin inhibitor dosing are ideal. If the dominant issues are hyperlipidemia and hypertension, the conversion from cyclosporine to tacrolimus may result in improvements of these comorbidities.
3.3 Mammalian Target of Rapamycin (mTOR) Inhibitors: (Rapamycin/Sirolimus)
Sirolimus is a potent immunosuppressive drug capable of significantly reducing acute graft rejecting. However, hyperlipidemia is a major adverse event associated with Sirolimus. Sirolimus is thought to induce or exacerbate hyperlipidemia in a reversible and dose-dependent manner. It can increase total cholesterol and LDL with a much more potent effect on triglycerides. The mechanism leading to hypertriglyceridemia is thought to be multifactorial. Sirolimus can interfere with insulin-dependent adipocyte triglyceride storage. There is an increase in apolipoprotein B100 (associated with VLDL and LDL cholesterol), an increase in C III levels (which is a lipoprotein lipase inhibitor), and an increase in apolipoprotein C II (a lipoprotein lipase activator for triglyceride hydrolysis) (Morrisett et al. 2002).
Sirolimus also effects glucose metabolism and can cause glucose intolerance through unrestrained activation of hepatic gluconeogenesis. This can lead to the occurrence of a diabetes-like syndrome in patients (Houde et al. 2010).
3.4 Antimetabolites: MMF (CellCept)
Although very little data exist for the specific effects of MMF on metabolic comorbidities. Thus, this agent should be considered as an additional immunosuppressive agent that could allow dose reductions of the background immunosuppression (calcineurin or mTOR inhibitors) in patients with hypertension and metabolic disease.
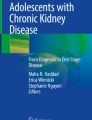
Immunosuppression: hypertension and metabolic disease | ||
|---|---|---|
Immunosuppressant | Effect | Comments |
Corticosteroids | Hyperlipidemia HTN Insulin resistance Weight gain | – With prolonged use: ↑LDL, ↑HDL, TG↔ – Salt, water retention and Vasoconstirction – Dose dependent, reversible with taper off – Enhanced appetite |
Calcineurin inhibitors Tacrolimus (Tac) Cyclosporin (CsA) | Hyperlipidemia HTN Reduced insulin synthesis and increased resistance | – CsA > tac – CsA > tac – Tac > CsA |
mTOR inhibitors Sirolimus | Hypertriglyceridemia Glucose intolerance and insulin resistance | |
Antimetabolites MMF (CellCept) | No significant effect | |
References
Bell PR, Briggs JD, Calman KC, Paton AM, Wood RF, Macpherson SG, Kyle K (1971) Reversal of acute clinical and experimental organ rejection using large doses of intravenous prednisolone. Lancet 1(7705):876–880. https://doi.org/10.1016/s0140-6736(71)92441-x
Cantarovich M, Giannetti N, Barkun J, Cecere R (2004) Antithymocyte globulin induction allows a prolonged delay in the initiation of cyclosporine in heart transplant patients with postoperative renal dysfunction. Transplantation 78:779
Cooney GF, Jeevanandam V, Choudhury S et al (1998) Comparative bioavailability of Neoral and Sandimmune in cardiac transplant recipients over 1 year. Transplant Proc 30(5):1892–1894
Eisen H, Ross H (2004) Optimizing the immunosuppressive regimen in heart transplantation. J Heart Lung Transplant 23(5 Suppl):S207–S213. https://doi.org/10.1016/j.healun.2004.03.010
Goodwin JE, Zhang J, Geller DS (2008) A critical role for vascular smooth muscle in acute glucocorticoid-induced hypertension. J Am Soc Nephrol 19(7):1291–1299. https://doi.org/10.1681/ASN.2007080911
Grimm M, Rinaldi M, Yonan NA et al (2006) Superior prevention of acute rejection by tacrolimus vs. cyclosporine in heart transplant recipients—a large European trial. Am J Transplant 6(6):1387–1397
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC Jr, Spertus JA, Costa F, American Heart Association, National Heart, Lung, and Blood Institute (2005) Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 112(17):2735–2752. Erratum in: Circulation. 2005 Oct 25;112(17): e297. Erratum in: Circulation. 2005 Oct 25;112(17): e298. https://doi.org/10.1161/CIRCULATIONAHA.105.169404
Guba M, von Breitenbuch P, Steinbauer M et al (2002) Rapamycin inhibits primary and metastatic tumor growth by antiangiogenesis: involvement of vascular endothelial growth factor. Nat Med 8(2):128–135
Heitman J, Movva NR, Hall MN (1991) Targets for cell cycle arrest by the immunosuppressant rapamycin in yeast. Science 253(5022):905–909
Higgins R, Kirklin JK, Brown RN et al (2005) To induce or not to induce: do patients at greatest risk for fatal rejection benefit from cytolytic induction therapy? J Heart Lung Transplant 24:392
Houde VP, Brûlé S, Festuccia WT, Blanchard PG, Bellmann K, Deshaies Y, Marette A (2010) Chronic rapamycin treatment causes glucose intolerance and hyperlipidemia by upregulating hepatic gluconeogenesis and impairing lipid deposition in adipose tissue. Diabetes 59(6):1338–1348. https://doi.org/10.2337/db09-1324
Keogh A, Richardson M, Ruygrok P et al (2004) Sirolimus in de novo heart transplant recipients reduces acute rejection and prevents coronary artery disease at 2 years: a randomized clinical trial. Circulation 110:2694
Khush KK, Cherikh WS, Chambers DC et al (2019) The international thoracic organ transplant registry of the International Society for Heart and Lung Transplantation: thirty-sixth adult heart transplantation report - 2019; focus theme: donor and recipient size match [published correction appears in J Heart Lung Transplant. 2020 Jan;39(1):91]. J Heart Lung Transplant 38(10):1056–1066. https://doi.org/10.1016/j.healun.2019.08.004
Kirklin JK, Bourge RC, Naftel DC et al (1994) Treatment of recurrent heart rejection with mycophenolate mofetil (RS-61443): initial clinical experience. J Heart Lung Transplant 13(3):444–450
Klawitter J, Nashan B, Christians U (2015) Everolimus and sirolimus in transplantation-related but different. Expert Opin Drug Saf 14(7):1055–1070. https://doi.org/10.1517/14740338.2015.1040388
Kobashigawa JA, Patel J, Furukawa H et al (2006) Five-year results of a randomized, single-center study of tacrolimus vs microemulsion cyclosporine in heart transplant patients. J Heart Lung Transplant 25(4):434–439
Lau KK, Tancredi DJ, Perez RV, Butani L (2010) Unusual pattern of dyslipidemia in children receiving steroid minimization immunosuppression after renal transplantation. Clin J Am Soc Nephrol 5(8):1506–1512. https://doi.org/10.2215/CJN.08431109
Moien-Afshari F, McManus BM, Laher I (2003) Immunosuppression and transplant vascular disease: benefits and adverse effects. Pharmacol Ther 100(2):141–156. https://doi.org/10.1016/j.pharmthera.2003.08.002
Morrisett JD, Abdel-Fattah G, Hoogeveen R, Mitchell E, Ballantyne CM, Pownall HJ, Opekun AR, Jaffe JS, Oppermann S, Kahan BD (2002) Effects of sirolimus on plasma lipids, lipoprotein levels, and fatty acid metabolism in renal transplant patients. J Lipid Res 43(8):1170–1180
Muñoz SJ (1995) Hyperlipidemia and other coronary risk factors after orthotopic liver transplantation: pathogenesis, diagnosis, and management. Liver Transpl Surg 1(5 Suppl 1):29–38
Øzbay LA, Smidt K, Mortensen DM, Carstens J, Jørgensen KA, Rungby J (2011) Cyclosporin and tacrolimus impair insulin secretion and transcriptional regulation in INS-1E beta-cells. Br J Pharmacol 162(1):136–146. https://doi.org/10.1111/j.1476-5381.2010.01018.x
Penninga L, Møller CH, Gustafsson F et al (2013) Immunosuppressive T-cell antibody induction for heart transplant recipients. Cochrane Database Syst Rev (12):CD008842
Pham SM, Kormos RL, Hattler BG, Kawai A, Tsamandas AC, Demetris AJ, Murali S, Fricker FJ, Chang HC, Jain AB, Starzl TE, Hardesty RL, Griffith BP (1996) A prospective trial of tacrolimus (FK 506) in clinical heart transplantation: intermediate-term results. J Thorac Cardiovasc Surg 111(4):764–772. https://doi.org/10.1016/s0022-5223(96)70336-7
Poston RS, Billingham M, Hoyt EG et al (1999) Rapamycin reverses chronic graft vascular disease in a novel cardiac allograft model. Circulation 100(1):67–74
Reichart B, Meiser B, Viganò M, Rinaldi M, Martinelli L, Yacoub M, Banner NR, Gandjbakhch I, Dorent R, Hetzer R, Hummel M (1998) European multicenter tacrolimus (FK506) heart pilot study: one-year results--European tacrolimus multicenter heart study group. J Heart Lung Transplant 17(8):775–781
Reichart B, Meiser B, Viganò M et al (2001) European multicenter tacrolimus heart pilot study: three year follow-up. J Heart Lung Transplant 20(2):249–250
Rosenberg PB, Vriesendorp AE, Drazner MH et al (2005) Induction therapy with basiliximab allows delayed initiation of cyclosporine and preserves renal function after cardiac transplantation. J Heart Lung Transplant 24:1327
Shin GT, Khanna A, Ding R et al (1998) In vivo expression of transforming growth factor-beta1 in humans: stimulation by cyclosporine. Transplantation 65(3):313–318
Taylor DO, Barr ML, Radovancevic B et al (1999) A randomized, multicenter comparison of tacrolimus and cyclosporine immunosuppressive regimens in cardiac transplantation: decreased hyperlipidemia and hypertension with tacrolimus. J Heart Lung Transplant 18(4):336–345
Valantine H (2000) Neoral use in the cardiac transplant recipient. Transplant Proc 32(3A Suppl):27S–44S
Vaziri ND, Ni Z, Zhang YP, Ruzics EP, Maleki P, Ding Y (1998) Depressed renal and vascular nitric oxide synthase expression in cyclosporine-induced hypertension. Kidney Int 54(2):482–491. https://doi.org/10.1046/j.1523-1755.1998.00014.x
Watt KD (2011) Metabolic syndrome: is immunosuppression to blame? Liver Transpl 17:S38–S42. https://doi.org/10.1002/lt.22386
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Hoosain, J., Hamad, E. (2021). Adverse Effects of Immunosuppression: Nephrotoxicity, Hypertension, and Metabolic Disease. In: Eisen, H.J. (eds) Pharmacology of Immunosuppression. Handbook of Experimental Pharmacology, vol 272. Springer, Cham. https://doi.org/10.1007/164_2021_547
Download citation
DOI: https://doi.org/10.1007/164_2021_547
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-05117-3
Online ISBN: 978-3-031-05118-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)