
Abstract
The Meek technique involves using a Meek-Wall microdermatome producing widely expanded postage stamp autografts, in which prefolded gauzes are used to gain a regular distribution of the autografts. The gauze pleats are pulled out on all the four sides to provide uniform expansion of the islands of grafts. The authors describe their use of the Parkland formula for the percentage of second- and third-degree burns for fluid resuscitation, their technique of debridement, and how the grafts are produced. When faced with large surface area burns and limited donor sites, the Meek technique is a satisfactory method to cover large wounds.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
To overcome the problem of extensive full thickness third-degree burns, the Meek technique was devised by Meek in 1963 [1]. This involved using a Meek-Wall microdermatome producing widely expanded postage stamp autografts, in which prefolded gauzes were used to gain a regular distribution of the autografts [2]. The technique, with an expansion rate of 1:9, was cumbersome and not frequently used. Tanner et al. (1964) [3] devised meshed skin grafts that improved the treatment of severe full thickness burns that replaced the Meek technique. Kreis et al. (1993) [4] modified the Meek technique by using a different device for cutting the grafts and employed aluminum foil backing to help the expansion of the skin grafts. The mean epithelialization rate was 90% (range 70–100%) within 5 weeks. The Meek technique utilizes small pieces of autograft and has proved to be a practical alternative to mesh grafts when donor sites are limited.
The authors describe their use of the Meek technique in a fair number of cases.
2 Technique
The authors reviewed 148 skin grafting surgeries from 2006 to 2015. The mean percentage body surface burned was 65% (range 50–87%), and full thickness injury occurred in 52% (range 40–81%) (Table 1).
Patients with associated inhalation injury were intubated on admission. Wounds were dressed with Flamazine (Smith & Nephew, Canada) that contained 1% silver sulfadiazine. Fluid resuscitation followed the Parkland formula (Table 2) [5]. For example, a person weighing 75 kg with burns to 20% of his or her body surface area would require 4 × 75 × 20 = 6000 mL of fluid replacement within 24 h. The first half of this amount is delivered within 8 h from the burn incident, and the remaining fluid is delivered in the next 16 h [6]. The burn percentage in adults can be estimated by applying the Wallace rule of nines (see total body surface area): 9% for each arm, 18% for each leg, 18% for the front of the torso, 18% for the back of the torso, 9% for the head, and 1% for the perineum [7].
Surgery was performed on the 3rd to 5th post-burn day after stabilization with fluids and electrolytes [8]. The Weck knife and the Humby knife were used to debride until punctuate bleeding occurred and the layer was grossly judged to be viable. When indicated, the entire skin down to the fascia was removed and the Meek technique was employed to close the wound. Epigard alloplastic material was used to temporarily cover debrided wounds when portions of the debrided areas were not able to be covered immediately. This procedure was repeated every 2–5 days, providing the patient’s condition allowed for surgical intervention.
The wounds are excised down to the healthy layers and hemostasis secured (Fig. 1). The extent of skin expansion required was determined by the size of the wound and the size of the available skin for grafting. The harvested autograft skin is placed on 42 × 42 mm dampened cork with the dermis side down and trimmed to the required size (Fig. 2). Then it is placed on the carrier block and passed through a modified Meek-Wall dermatome, which contains 13 parallel blades, spaced 3 mm apart that cut the graft but not the cork (Fig. 3). After the first pass, the cork plate is rotated to 90° and passed through the dermatome once more thus cutting the graft in to 14 × 14 square islands measuring 3 × 3 mm.

Tangential excision of full thickness burn of the whole back. Modified from Almodumeegh A, Heidekrueger PI, Ninkovic M, Rubenbauer J, Hadjipanayi E, Broer PN. The MEEK technique: 10-year experience at a tertiary burn centre. Int Wound J. 2016 In publication

After harvesting the split-thickness skin grafts in a normal fashion, the grafts are manually cut in pieces and stretched over the 42 × 42 mm moistened cork plate with the inner layer facing downward for final cutting. Modified from Almodumeegh A, Heidekrueger PI, Ninkovic M, Rubenbauer J, Hadjipanayi E, Broer PN. The MEEK technique: 10-year experience at a tertiary burn centre. Int Wound J. 2016 In publication

Meshing of the graft is achieved using the modified Meek-Wall dermatome. Modified from Almodumeegh A, Heidekrueger PI, Ninkovic M, Rubenbauer J, Hadjipanayi E, Broer PN. The MEEK technique: 10-year experience at a tertiary burn centre. Int Wound J. 2016 In publication
The cork, with the cut graft in place, is removed. The epidermal side of the graft is sprayed with an adhesive dressing spray (Leukospray, Beiersdorf GmbH, Germany). After about 2–5 min, the sticky surface of the graft is brought into contact with the prefolded (pleated) gauze (Fig. 4), and the pleats are pulled out on all the four sides to provide uniform expansion of the islands (Fig. 5), with ratios varying from 1:3 to 1:9. The gauze is pulled steadily in all directions until it was completely smooth and flattened.

The cork is removed once the minced grafts are transferred to prefolded polyamide gauze backed with aluminum foil. Modified from Almodumeegh A, Heidekrueger PI, Ninkovic M, Rubenbauer J, Hadjipanayi E, Broer PN. The MEEK technique: 10-year experience at a tertiary burn centre. Int Wound J. 2016 In publication

The gauze is pulled steadily and firmly in all directions until it is completely smooth and flattened. Modified from Almodumeegh A, Heidekrueger PI, Ninkovic M, Rubenbauer J, Hadjipanayi E, Broer PN. The MEEK technique: 10-year experience at a tertiary burn centre. Int Wound J. 2016;14(4):601–5
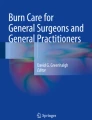
The graft is applied to the wound bed and the gauze tacked down with surgical staples (Fig. 6). The grafted wound is covered with Jelonet gauze (Smith & Nephew, Canada) impregnated with Lavasept-Gel (B. Braun Melsungen AG, Germany) containing polihexanide antimicrobial. The operative sites in the trunk and extremities are additionally dressed with Jelonet and wrapped with elastic bandages. After 3–5 days the dressing are changed every 2 days. Staples are removed after 7–10 days. One percent silver sulfadiazine cream is used to cover the wound if it showed signs of local infection.

(a) The skin graft is applied onto the wound bed, and the edges of gauze are tacked down with surgical staples. (b) The appearance of the grafted wound at the 10th day after the procedure. The viability of the graft was assessed as satisfactory. Modified from Almodumeegh A, Heidekrueger PI, Ninkovic M, Rubenbauer J, Hadjipanayi E, Broer PN. The MEEK technique: 10-year experience at a tertiary burn centre. Int Wound J. 2016;14(4):601–5
The mean area graft per procedure was 20% (range 15–25%). The viability of the graft as assessed on the 7–10th day was generally in the range of 60–90% (Fig. 6). The average number of operations required was 1–3 (Table 1). When the initial graft application failed, infection or hematoma was most commonly responsible. Although blood replacement was prescribed as needed at surgery, transfusions seldom exceeded two units per session. Functional and aesthetic outcomes of wounds treated with Meek grafts were satisfactory in most instances.
Infection was noted in five patients. There were seven deaths, four dying from respiratory failure due to severe inhalation injury and three dying from septic shock.
3 Discussion
Meshed split-thickness skin grafting has been an accepted method of treatment for severely burned patients at most burn centers [8,9,10]. However, especially in large area burns, lack of autograft skin may become a limiting factor. In order to prevent wound infection and septicemia, remaining areas of eschar should be excised even if they cannot be covered with autografts immediately [11, 12]. Our experience utilizing the Meek technique in large burn areas suggests that it provides a reliable method to achieve wound healing with expanded autografts. The main advantage is that the Meek technique allows a greater expansion ratio as compared to mesh grafts [12]. The small autografts can be easily applied in contrast to the oftentimes challenging handling of higher expansion (1:6 or 1:9) mesh grafts [4, 13].
Infection, as noted in five of our cases, can be a common cause for graft failure. Similar to others, we found that the thickness of skin grafts used for wound coverage does not seem to affect the incidence of infection. Indeed, small postage stamp skin grafts appear to be more resistant to invasion by microorganisms, and we also observed that spacing and distribution of the micrografts allowed for faster and more uniform epithelialization [12,13,14].
In our experience, the cosmetic result following the Meek graft technique is comparable with that of widely expanded mesh grafts. A major downside of the micrografting technique is the fact that it is expensive and needs more staff in the operating room to be carried out [14].
Conclusions
When faced with large surface area burns and limited donor sites, the Meek technique is a satisfactory method to cover large wounds. While labor extensive, paying attention to the outlined principles allows achieving good functional and aesthetic results in this challenging patient population.
References
Meek CP (1958) Successful microdermagrafting using the Meek wall microdermatome. Ann J Surg 96:557–558
Meek CP (1963) Extensive severe burn treated with enzymatic debridement and micro dermagrafting: case report. Am Surg 29(1):61–64
Tanner JC, Vandeput JF, Olley JF (1964) The Mesh skin graft. Plast Reconstr Surg 34:287–292
Kreis RW, Mackie DP, Vloemans AW, Hermans RP, Hockstram MJ (1993) Widely expanded postage stamp skin grafts using a modified Meek technique in combination with an allograft overlay. Burns 19(2):142–145
Parkland formula. http://www.josephsunny.com/medsoft/parkland.html. Accessed 3 July 2017
Williams C (2008) Fluid resuscitation in burn patients 1: using formulas. Nurs Times 104(14):28–29
Explore Burns Mdcalc, Fluid Requirements, and more! https://www.pinterest/pin/440649144772194432/. Accessed 3 July 2017
Alexander JW, Macmillan BG, Law E, Kittur DS (1981) Treatment of severe burns with widely meshed skin autografts and meshed allograft overlay. J Trauma 21:433
Gang RK, Arturson G, Hakelius L (1981) The effect of split skin allografts on wound epithelialization from autologous patch grafts. Scand J Plast Reconstr Surg 15:1–4
Minanov O, Peterson HD (1997) Burn injury. In: Georgiade GS, Riefkohl R, Scott Levin L (eds) Plastic maxillofacial and reconstructive surgery, 3rd edn. Williams & Wilkins, Baltimore, p 203
Macmillan BG (1958) Early excision of more than 25% of body surface in the extensively burned patients. Arch Surg 77:369
Raff T, Hartman B, Wagner H, German G (1996) Experience with modified Meek technique. Burns 38(4):142–146
Kreis RW, Mackie DP, Hermans RP, Vloemans AR (1994) Expansion technique for skin grafts: comparison between mesh and meek island (Sandwich) grafts. Burns 20(1):539–542
Zermani RGC, Zarabini A, Trivisonno A (1997) Micrografting in the treatment of severely burned patients. Burns 23:604–607
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this chapter
Cite this chapter
Heidekrueger, P.I., Broer, P.N., Ninkovic, M. (2017). The Meek Technique in the Treatment of Burns. In: Shiffman, M., Low, M. (eds) Burns, Infections and Wound Management. Recent Clinical Techniques, Results, and Research in Wounds, vol 2. Springer, Cham. https://doi.org/10.1007/15695_2017_29
Download citation
DOI: https://doi.org/10.1007/15695_2017_29
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-10685-0
Online ISBN: 978-3-030-10686-7
eBook Packages: MedicineMedicine (R0)