
Abstract
Functional connectivity MRI (fcMRI) is a technique that examines the synchrony of repeated functional MRI (fMRI) measurements between two or more brain regions. The underlying concept is that even random “noise” in a brain region will get propagated to other connected brain areas and that this will result in synchronized patterns of activation that are specific to functionally connected brain networks. The fcMRI literature in autism has proliferated rapidly, with general, although not uniform evidence of underconnectivity in distributed brain networks in autism. Studies to date are heterogeneous, some using an underlying cognitive task and others not; some examine specific neural pathways and others examine large networks or the entire brain. Abnormalities are most apparent in distributed networks in association cortex, with the default mode network being the most commonly reported abnormal network. Future studies will greatly benefit from data-sharing initiatives such as the Autism Brain Imaging Data Exchange (ABIDE) and National Database for Autism Research (NDAR). Despite lingering methodological concerns, there is reason for optimism that replicable patterns of abnormal brain connectivity may be established in the near future.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
11.1 Introduction
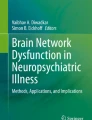
The theory underlying functional connectivity MRI was established in a landmark paper by Bharat Biswal and colleagues (1995). By obtaining serial images of the brain in the absence of any cognitive task, they observed synchrony of intrinsic blood–oxygen-level-dependent (BOLD) signal fluctuations in the primary motor cortex that recapitulated a network seen on motor task-performance studies. Since then, there has been an explosion of interest categorizing a new neuroanatomical paradigm where distributed networks of widely separated but functionally related brain regions have been characterized (Fox and Raichle 2007) (Fig. 11.1).

Synchronized BOLD recordings. The traces below were obtained from left (blue) and right (red) temporo-occipital cortex as shown in the images, representing a 4-min recording of BOLD signal, while the single subject rested with their eyes open in the MRI scanner. Even though the traces are obtained from opposite hemispheres when no task was present, there is strong synchrony between the two regions
The use of functional connectivity methods to study autism has been among the most enthusiastic applications of fcMRI, with over 50 reports of abnormalities in autism in the last decade. Several excellent reviews have now characterized the abnormalities reported in these early studies (Kana et al. 2011; Muller et al. 2011; Schipul et al. 2011; Vissers et al. 2012). In this chapter, a review is presented of reports of abnormal functional connectivity with an emphasis on describing areas of convergent abnormalities across studies and assessing whether the literature can support a unified theory of brain connectivity underlying autism.
11.2 Decreased Functional Connectivity in Autism
The initial report of decreased functional MRI connectivity in autism was published in 2004 by Marcel Just and colleagues (2004), with related reports of decreased connectivity in autism in different neural subsystems by two independent groups shortly thereafter (Villalobos et al. 2005, Welchew et al. 2005).
Just and colleagues presented a series of 17 high-functioning autism subjects, compared with 17 healthy typically developing subjects, in which they examined BOLD fMRI data acquired during a sentence comprehension task. Sentence comprehension blocks were interspersed with eight 24-s “resting” intervals during which subjects visually fixated on an asterisk on the screen, which were excluded from the analysis. Regions of interest (ROI) were selected for which a significant difference in activation was observed between task and control epochs. For each of these ROIs, a time course for the region was extracted from the images, and correlation between the time series (synchrony) was measured for each subject. In ten separate pairs of ROIs showing activation by the task, the synchrony was greater for control subjects than for autism subjects (Just et al. 2004).
Although this observation was made from data obtained during performance of a language task and findings may result to differential task performance rather than any underlying structural connectivity difference, a pattern of widely decreased functional connectivity was established that has now been replicated in many but not all of the studies examining functional connectivity in autism, which will be discussed by neural subsystem below.
11.3 Connectivity in the Default Mode Network
One of the most compelling networks demonstrating decreased connectivity in autism is the default mode network. This network is particularly compelling in autism, because behaviors associated with these brain regions (internal stimuli, internal narrative, self-focus) correspond to symptoms of autism in which individuals may exhibit internal reflection at the expense of awareness of the outside world. Regions of the default mode network also comprise core regions ascribed to the brain’s “theory-of-mind” network associated with self-identification and implicated in autism symptomatology (Baron-Cohen 1995). At least ten studies have examined connectivity or function within the default mode network in autism (Fig. 11.2).

Default mode and attention control networks. The images represent average functional connectivity to four seeds in each network (default mode: posterior cingulate, medial prefrontal, bilateral temporoparietal junction; attention control: bilateral intraparietal sulcus and frontal insula). The default mode network is shown in cool colors and the attention control network is shown in warm colors
By pooling subjects from prior datasets using multiple different tasks, Cherkassky and colleagues amassed 57 autism and 57 matched control subjects and looked at the resting epochs for all of the tasks. They found that in 94 % of the pairs of 12 regions comprising the default mode network, autism subjects had lower functional connectivity.
A contemporaneous study by Kennedy et al. took a different approach (Kennedy et al. 2006). They examined data from autism and control subjects during performance of a Stroop task where subjects were instructed to count words on the screen that were incongruent with the words shown (e.g., “two”). The investigators looked specifically at whether the default mode network regions deactivated during the interspersed resting (fixation) blocks compared to the task and found significantly less deactivation in autism subjects. A subsequent study (Kennedy and Courchesne 2008b) found that the attention control network did not show decreased connectivity in autism, while the default mode network did. A task-based study employing asking subjects to answer true/false questions about self vs. another person found reduced activity in the anterior node of the default mode network (Kennedy and Courchesne 2008a).
The relationship between the default mode network and theory of mind was probed directly by Mason and colleagues (2008) in a paradigm where subjects read passages requiring inferences about internal or emotional states vs. physical causality. They found increased recruitment of the right hemisphere for this task in autism, in particular the right inferior parietal lobule, whereas control subjects activated this region only for inferences about intentional states. The autism group also showed reduced functional connectivity within nodes of the default mode network.
In a study by Kana and colleagues (2009), participants viewed animated images and made judgments about mental states of the characters. They found decreased connectivity during the task between anterior and posterior nodes of the default mode network and hypofunction of theory-of-mind regions that correlated to decreased performance on psychometric testing of theory-of-mind function.
This finding of decreased anterior/posterior default mode connectivity was independently reproduced in a resting study by Monk and colleagues (2009) that correlated with poor social function. A similar study in adolescents confirmed decreased connectivity associated with 9 of 11 default mode network regions in autism subjects, with weaker connectivity associated with both poorer social function and higher restricted interests and repetitive behaviors on questionnaires (Weng et al. 2010).
Using a separate analysis technique of independent component analysis, Assaf and colleagues also find significantly weaker functional connectivity between nodes of the default mode network that was correlated with poorer social function on objective and subjective testing (Assaf et al. 2010).
Finally, in a study wherein participants made mental or physical judgments about self vs. others, autism subjects showed relative hypoactivation of the medial prefrontal cortex DMN node with weaker functional connectivity to several other brain regions and medial prefrontal cortex, also correlated with disease severity (Lombardo et al. 2010).
These studies show virtually uniform decreases in internal connectivity within the default mode network associated with hypofunction of particularly the anterior, medial prefrontal node and correlated with disease severity. Nevertheless, as is typical for fMRI studies, results are often in context of failure to deactivate during a task or decreased contrast between two mental states. Many of these results could also be obtained if autism subjects showed tonically greater activity in default mode network regions, although this would be harder to explain in studies without an underlying task. Alternatively, it is possible to explain all of these results not by weak connectivity within the default mode network but rather by overconnectivity between attention control network regions and default mode network regions. Since the default mode network and attention control network exhibit to some extent an inverse relationship in temporal activity profiles (Fox et al. 2005), increased correlation between the two networks may result in weaker segregation of the networks and decreased synchrony between DMN nodes. Further studies may clarify the relationship of functional connectivity between DMN nodes and areas outside the network, such as the attention control network.
11.4 Connectivity in Facial Processing
Functional connectivity in autism for brain regions associated with face processing has been evaluated in many task-based and several functional connectivity studies. It is widely believed that individuals with autism have difficulty or disinterest in visualizing faces, resulting in considerable interest in the neural mechanisms underlying these deficits.
A study by Welchew and colleagues (2005) scanned 26 subjects while viewing fearful facial expressions and found decreased synchrony of the amygdala and parahippocampal gyrus. Similarly, Kleinhans et al. (2008) scanned 40 subjects during a face identification task and found decreased synchrony of the fusiform face area and both the amygdala and posterior cingulate cortex, with reduced FFA–amygdala connectivity associated with poorer social function.
A study by Bird et al. (2006) used the technique of dynamic causal modeling to compare differences in activation in response to face or house visual stimuli when the stimuli were attended to or not attended to. The results indicated decreased top–down attentional modulation of primary visual cortex to extrastriate visual cortex information processing, selective for faces. Given the potential for an attentional bias, Monk and colleagues (2010) used reaction times to control for attentional differences on trials and found that ASD subjects showed greater activation of the right amygdala to emotional faces than TD subjects. Functional connectivity between right amygdala and the anterior temporal lobe was weaker, while amygdala to medial prefrontal cortex was stronger.
11.5 Connectivity in Visual Search and Perception
Several studies have now examined functional connectivity in association with complex visuospatial perception tasks. The domain of visual perception, unlike complex social or empathic brain networks, is often seen as relatively spared or even enhanced in autism. Villalobos and colleagues measured decreased functional connectivity in autism between primary visual cortex and inferior frontal cortex (Brodmann area 44) during a visuomotor task where participants pressed a button following a visual cue (Villalobos et al. 2005). A study obtained during a coherent motion paradigm by Brieber et al. showed no difference in functional connectivity between V1 and V5 or between left and right V5 in autism (Brieber et al. 2010).
One set of experiments used imaging during an embedded figure task where participants were instructed to find “hidden” shapes within a larger, more complex shape. Damarla et al. (2010) found that even though performance did not differ between the groups, there was reduced activation and functional connectivity among frontal and parietal attentional areas than for controls. In a separate study using a different embedded figure task that incorporated distracting information from a three-dimensional stimulus, Liu et al. found that activation patterns for autism subjects differed in that they did not see increased activation for the task in superior and medial frontal regions (Liu et al. 2011). They interpreted this finding as less difficult for the task in autism subjects, possibly because the 3D distracters were less confusing for autism subjects. They observed corresponding decreased functional connectivity between medial frontal and posterior visuospatial ROIs.
Intriguingly, a subsequent study with larger sample size looked at data acquired during a visual search paradigm. After particularly rigorous motion correction that removed individual volumes showing motion for each subject, the data showed increased connectivity between the ventral and dorsal attention networks (subnetworks of the attention control network) and the visual network (Keehn et al. 2012). In a combined study using fMRI to define language and visuospatial ROIs and DTI to measure structural connectivity between the ROIs, autistic subjects also had preferentially higher connectivity between visuospatial regions, but lower connectivity for connections involving frontal language areas (Sahyoun et al. 2010).
Thus, while studies examining functional connectivity in the default mode network appear to show relatively uniform decreases in synchrony between network nodes, studies involving complex visual perception are mixed. During facial processing tasks, connectivity appears decreased both in attentional and visual association cortex. Yet during visual search or abstract feature recognition tasks, autism subjects showed increased functional connectivity between brain attentional regions. This may correspond to performance differences in tasks for which autism subjects excel vs. perform poorly. Alternately, there may be heterogeneity across brain networks in the extent to which connectivity is impaired in autism, consistent with the preserved connectivity seen in the attention control network despite impaired connectivity in the default mode network seen in the results of Kennedy and Courchesne (2008b).
11.6 Connectivity in Executive, Working Memory, and Attentional Regions
A number of studies have now directly examined connectivity during tasks associated with brain attentional, working memory, and executive regions. The first study to examine connectivity directly within the attention control network in autism was by Koshino et al. (2005). Using an n-back task with letters, they found that the left inferior parietal lobule was less synchronized with the rest of the attention control network. A slight increase in right frontoparietal synchrony in autism was not significant. In a second experiment, Koshino et al. (2008) performed an n-back task with face stimuli. They found decreased functional connectivity in autism between frontal regions activated by the task and the bilateral fusiform areas. Frontoparietal connectivity in autism was lower, but this was not statistically significant.
Using a Tower of London task, Just et al. found that frontoparietal functional connectivity was lower in autism, with the regions tested lying more within the ventral attention network (Just et al. 2007). A cognitive control task performed by Solomon et al. (2009) consisted of a task where participants had to remember a cue (colored square) for 8 s and then make a response to an arrow stimulus based on the color of the cue. Since a minority of responses required incongruent responses, the task was also a response inhibition task. Functional connectivity analysis showed reduced frontoparietal connectivity within the attention control network (Solomon et al. 2009). In a study that limited analysis to the frontal eye field and anterior cingulate cortex using an eye movement (saccade to target), task, performance, activation, and ACC–FEF functional connectivity were reduced in the autism sample (Agam et al. 2010).
Several studies have looked at regions associated with stimulus salience or novelty detection including the anterior insula and cingulate cortex (Seeley et al. 2007), a network also associated with response inhibition. In a go–no go task performed by Kana et al. (2007), participants were instructed to press or not press a button in response to a cue, with a minority of cues requiring no action. This task has design similarities with oddball tasks where the “salient” stimuli, those requiring no action, activate brain regions of the salience network. They found decreased responses in the middle cingulate cortex for autism subjects and decreased functional connectivity between cingulate cortex and right inferior parietal lobule. In a similar task in children, Lee et al. found a trend toward decreased functional connectivity between the right frontoinsular and right inferior parietal cortex (Lee et al. 2009).
Few studies have examined connectivity in autism within the attention control network using a resting paradigm. In a resting fMRI study of 25 typically developing adults, Di Martino and colleagues found a significant inverse relationship between cinguloinsular functional connectivity and Social Responsiveness Scale measurements, indicating that traits that resembled the autism phenotype within a neurotypical population are associated with decreased connectivity in the salience network (Di Martino et al. 2009). A resting-state fMRI study in adolescents showed decreased functional connectivity between the anterior and posterior insula (Ebisch et al. 2011).
In summary, connectivity studies within the attention control network show uniformly decreased functional connectivity in autism. Yet this observation could be almost entirely explained by differential task performance in autism subjects since almost all of the studies were performed in datasets obtained during an attentionally demanding task. Yet resting-state studies by Di Martino (Di Martino et al. 2009) and Ebisch (Ebisch et al. 2011) are not driven by external stimuli and also show decreased connectivity at least involving the anterior insula, a region that recurs in imaging studies of autism as abnormal (Uddin and Menon 2009). No studies to date have explicitly characterized connectivity between the attention control and default mode networks.
11.7 Connectivity in Language Regions
In addition to the initial report by Just and colleagues (2004) described above, functional connectivity in the language subsystem in autism has been examined in several subsequent studies. Kana and colleagues (2006) also performed scans during a sentence comprehension task but examined the imagery content in the sentences as a covariate. For high-imagery sentences, controls showed greater activation of language regions. Autism subjects exhibited a trend toward lower frontal–parietal functional connectivity.
A language memory task involving ten ASD and ten control participants evaluated functional connectivity between three seeds in the left occipital, left superior parietal, and left middle frontal regions and the rest of the brain. Increased connectivity between the seeds and scattered areas in the high medial posterior frontal, posterior temporal, and anterior occipital lobes was seen in autism (Noonan et al. 2009).
A study involving data collected during a verbal fluency task performed regression of task activation results and compared differences in connectivity attributable to differential task performance to differences in connectivity associated with spontaneous neuronal synchronization (Jones et al. 2010). Results showed that while functional connectivity involving seeds activated by the language task paradigm showed generally decreased connectivity in autism, this effect was greatest on the spontaneous interregional synchrony after task activity was regressed out of the data.
Given that autistic children sometimes make errors in deictic shifting (incorrect use of pronouns “I” and “you”), Mizuno and colleagues performed a study imaging participants during a linguistic perspective-taking task (Mizuno et al. 2011). Functional connectivity between the right anterior insula and the precuneus was decreased in autism, and within the autism group, this connectivity measurement was positively correlated with task performance (low reaction time). Lai and colleagues examined children during speech and song stimulation and found greater left frontal to left temporoparietal language connectivity during song than speech in autistic children, but no ASD/TD distinction could be made because many of the autistic children underwent propofol sedation for the exam (Lai et al. 2012).
A study by Dinstein and colleagues is the first to evaluate functional connectivity in nonsedated toddlers by imaging during natural sleep (Dinstein et al. 2011). The investigators regressed out task-evoked signals from auditory stimulation and evaluated interhemispheric correlation to find decreased synchrony in autism in the inferior frontal gyrus (Broca’s area) and superior temporal gyrus (Wernicke’s area) compared to controls. Inferior frontal gyrus interhemispheric correlation was negatively associated with communication and social deficits and positively associated with language function. Moreover, weaker interhemispheric correlations in inferior frontal and superior temporal gyrus could identify toddlers with autism with 72 % sensitivity and 84 % specificity (Dinstein et al. 2011).
11.8 Connectivity in Motor Regions
Individuals with autism typically have deficits in fine and gross motor skills, and a single study has evaluated functional connectivity within motor networks. Mostofsky and colleagues performed imaging during a finger-sequencing task and evaluated functional connectivity within bilateral motor cortex, bilateral cerebellum, bilateral thalamus, and supplementary motor area. Every pair of ROIs showed significantly greater functional connectivity in controls except for left vs. right cerebellum (Mostofsky et al. 2009). This corresponded with impaired behavioral performance on motor testing for the autism group.
11.9 Connectivity with Subcortical Nuclei
Studies of cortical/subcortical functional connectivity have examined both thalamocortical and corticostriatal synchrony. Mizuno and colleagues used data collected during a visuomotor coordination task to evaluate thalamocortical connectivity (Mizuno et al. 2006). They found more clusters in the cortex showing higher synchrony with the ipsilateral thalamus for their autism sample than for their control sample, although sample size was limited to eight subjects per group. The authors suggested that thalamocortical connectivity may differ from or be compensatory to the decreased corticocortical connectivity seen in autism in other studies.
Corticostriatal connectivity was evaluated during the same visuomotor task in eight subjects per group, and scattered areas of increased correlation to the left caudate were found in autism, while scattered areas of increased correlation to the right caudate were seen in controls (Turner et al. 2006). A subsequent study (Di Martino et al. 2011) examined 20 subjects per group with three seeds in each caudate and three seeds in each putamen during a resting-state acquisition. They found increased functional connectivity in autism between the striatum and areas of association cortex such as right superior temporal gyrus and bilateral insula as well as increased functional connectivity to the pons. One exception was decreased functional connectivity in autism between the striatum and posterior cingulate cortex.
These studies suggest a trend toward increased cortical–subcortical functional connectivity in autism that differs with most of the results seen for corticocortical connectivity. Several possible explanations might account for these differences. Subcortical connectivity may be to some extent compensatory for decreased corticocortical connections. If corticocortical networks are less robust in autism, then corticocortical connections may explain a lesser percentage of the variance of a cortical ROI’s time series, and thalamocortical and corticostriatal “connections” may explain a relatively larger share of the cortical ROI’s temporal fluctuations. Alternately, there are unique features about corticostriatal projections, namely, that direct pathway cortical–caudate projections are predominantly inhibitory (Rubchinsky et al. 2003), whereas corticocortical projections are typically excitatory. Thus, increased corticostriatal synchrony may actually represent decreased inhibition of the caudate by the cortex, still consistent with an underconnectivity hypothesis.
11.10 Local Connectivity
In its most commonly expressed form, the cortical underconnectivity hypothesis posits that autism is associated with short-range overconnectivity and long-range underconnectivity (Belmonte et al. 2004, Just et al. 2004). Yet the division between “short range” and “long range” can get substantially blurred as representing operationally a neuropsychological concept or graph–theoretical term between arbitrary nodes or physical definition about circuitry within a cortical column vs. local U-fibers vs. long-range projection fibers.
The most “short-range” type of connectivity that can be measured by techniques of functional connectivity MRI is synchrony between a voxel and its immediate neighbors, termed “regional homogeneity” (ReHo). Nevertheless this type of synchrony already extends over a scale of 3–5 mm and might seem already “long-range” from the perspective of an electrophysiologist or pathologist. Two studies have evaluated ReHo in autism. Paakki and colleagues measured regional homogeneity acquired during a resting state in adolescents and found a mixed distribution of intergroup differences. ReHo was decreased in autism for right superior temporal sulcus, right inferior and middle frontal gyri, bilateral cerebellar crus, right insula, and right postcentral gyrus, while ReHo was higher in autism for right thalamus, left inferior frontal, left subcallosal, and bilateral cerebellar hemisphere regions (Paakki et al. 2010). A second study by Shukla and colleagues acquired data during a visual search paradigm, with task parameters regressed out of voxelwise data. They found decreased ReHo in autism in superior parietal and anterior prefrontal regions, with increased ReHo in lateral and medial temporal regions, particularly on the right (Shukla et al. 2010). Both studies performed normalization of their ReHo measurements to control for noise, which limits the ability to detect global trends and predisposes toward a finding of a mixed spatial distribution of increased and decreased ReHo. Nevertheless, Shukla et al. (2010) performed an analysis without normalization and obtained similar results.
11.11 Connectivity in the Social Brain
There has been increasing attention in social neuroscience to a set of loci that are particularly active during fMRI studies of social function, empathy, and imitation of others, termed “the social brain.” These regions include the anterior insula, superior temporal sulcus, amygdala, default mode, and language regions (Adolphs 2009). Several recent studies have begun to evaluate whether these regions or data acquired during social or emotive paradigms show particularly abnormal connectivity in autism.
Wicker and colleagues used a task paradigm where participants assessed the emotional valence of dynamic faces and evaluated the data using structural equation modeling for social brain loci (Wicker et al. 2008). They found weaker top–down effective connectivity between temporolimbic structures (amygdala, superior temporal sulcus) and prefrontal cortex. Results also showed increased effective connectivity between dorsolateral prefrontal cortex and fusiform face area.
A study examining data performed during letter detection and semantic decision tasks with task effects regressed out demonstrated increased connectivity between seeds in the right inferior frontal gyrus, superior temporal sulcus, and inferior parietal lobule with areas in the high medial prefrontal cortex and anterior cingulate cortex (Shih et al. 2010). Additional effective connectivity analysis using structural equation modeling showed decreased connectivity between inferior parietal lobule and inferior frontal gyrus in autism participants.
Decreased connectivity between socially relevant brain regions was also observed in a study by Schipul et al. from data performed during a social learning task where participants practiced detecting lying or truth-telling from facial expressions (Schipul et al. 2012). Not only did autism subjects show decreased connectivity between many of the 25 ROIs studied, but smaller increases in functional connectivity were seen during the learning period compared to the typically developing sample.
A recent resting-state analysis examined connectivity between social brain regions and found decreased functional connectivity in autism between nodes of the default mode network as well as between the amygdala and insula (von dem Hagen et al. 2012). Using both independent component analysis and seed-based approaches, von dem Hagen et al.’s study is one of few studies to also look at between-network connectivity in the case of the limbic network and the salience network, which was decreased in autism. A comprehensive analysis of social brain regions demonstrated widespread deacreased connectivity in autism (Gotts et al. 2012).
11.12 Distribution of Connectivity Abnormalities in the Brain
Most of the studies reviewed thus far have targeted specific neural subsystems to demonstrate differential connectivity in autism. The constellation of findings of generally decreased, though not uniformly decreased, connectivity suggests heterogeneity of connectivity differences that may not affect all brain regions equally. Two studies look at whole-brain connectivity differences to directly compare which region pairs show greatest synchrony differences in autism.
A study involving interhemispheric correlation examined resting-state data and compared each voxel with its interhemispheric homologue to assess a voxelwise difference in homotopic connectivity (Anderson et al. 2011c). Results showed heterogeneous connectivity that was weaker in autism for particular brain regions including the anterior insula, inferior parietal lobule, and posterior lateral frontal cortex, all predominantly association cortical regions.
In a study considering over 7,000 ROIs forming a lattice across the gray matter, functional connectivity was compared for every region pair, including over 26 million ROI pairs (Anderson et al. 2011d). This study found that functional connectivity among strongly synchronized, distant ROIs was generally weaker in autism but found that negatively correlated regions were less negatively correlated in autism. Although negatively correlated functional connectivity does not equate directly to underlying inhibitory connections (and may also represent a decrease in shared inputs from other sources), these results may be consistent with findings of Di Martino et al. (2011) that showed increased connectivity in corticostriatal connections that presumably reflect a significant proportion of underlying inhibitory connections. Anderson et al. also found that regions most frequently involved in abnormal connectivity in autism were regions of the default mode network, fusiform gyrus, and anterior insula, all key regions implicated in the pathophysiology of social deficits of autism (Anderson et al. 2011d). The connectivity patterns were sufficient to classify autism with accuracy approaching 90 % for subjects under 20 years of age, where effects were largest (Fig. 11.3).

Classification of typically developing and autism subjects using whole-brain functional connectivity MRI data. Accuracy was about 90 % for subjects under 20 years of age. Classifier score methods are described in Anderson et al. (2011a)
11.13 Behavioral Correlations and Modulating Variables
A growing body of literature is now investigating modulatory factors that could affect functional connectivity in autism. A study looking at the effects of beta-blockers in an autism population measured functional connectivity in predefined ROIs (Narayanan et al. 2010) before and after administration of propranolol, nadolol, and placebo. They found that functional connectivity between the four ROIs (averaged for all ROI pairs) was higher for propranolol than placebo or nadolol. These findings highlight the importance of consideration of participants’ medical regimens given the potential for asymmetric medication in autism and typically developing groups in other studies.
The relationship between functional connectivity in autism and genotype for the growing list of potential genetic susceptibility loci remains largely unknown. The first study directly investigating this relationship tested effects of genotype for locus contactin-associated protein-like 2 (CNTNAP2) was tested by Scott-Van Zeeland and colleagues (2010), who found increased functional connectivity for a medial prefrontal cortex seed to the posterior cingulate cortex (Default Mode Network) in the nonrisk group than for the risk group of the allele.
Although not directly measuring functional connectivity, resting-state BOLD low-frequency fluctuations were analyzed in a study by Lai and colleagues (2010) by examining the Hurst exponent of time series. The Hurst exponent is closely related to fractal dimension, measuring temporal complexity of a time series. This study found greater randomness in the time series of autism participants across a wide range of brain regions.
11.14 Effects of Age
From childhood through adolescence, a series of changes have been described in normal development (Fair et al. 2007) that consist of a relative strengthening of long-range functional connectivity within coherent networks (integration) as well as increasing distinctness of different functional networks (segregation). These changes are diminished in autism throughout the prior studies reviewed, best illustrated by impaired functional connectivity within the default mode network and decreased negative correlations across a large set of brain regions (Anderson et al. 2011d).
The reduced effects of segregation and integration in autism were explicitly tested in a study by Rudie et al. that evaluated a cohort of adolescent autism and typically developing subjects during a task of emotional face processing. Task effects were regressed out, and functional connectivity was measured under a range of postprocessing strategies between the bilateral amygdala and right frontal operculum and the rest of the brain. Areas where the seeds were positively correlated tended to be more so in typically developing subjects, while areas that were negatively correlated were even more negatively correlated in control subjects (Rudie et al. 2012).
In a cohort of 41 typically developing and 39 autism participants, Wiggins and colleagues measured synchrony of resting-state BOLD images in the anterior and posterior hubs of the default mode network using a seed-independent self-organizing map technique (Wiggins et al. 2011). They found not only that anterior and posterior hubs were less correlated in autism but that this correlation increased less with age than for typically developing subjects. This also corresponds with findings of Anderson and colleagues that functional connectivity is most abnormal in children and adolescents with autism, with a trend toward normalization relative to typical development by about age 20 (Anderson et al. 2011d).
11.15 Methodological Considerations
Despite strong convergent findings across more than 50 primary reports, there are good reasons to maintain tentativity about findings of altered functional connectivity in autism. Over the time period these studies were performed, there has been considerable maturation of functional connectivity methods. One such example is evolving methods used for correction of nuisance signals such as heart rate and respiration. A common technique used in many but not all of the studies above is global signal regression, where the mean BOLD time series for a mask including the entire brain is regressed from each voxel’s time series. This has been shown to generate spurious functional anticorrelations (Fox et al. 2009, Murphy et al. 2009). Although it is possible that this technique could differentially affect patient groups, for example, if a network was spatially larger in one group compared to the other (Anderson et al. 2011b), this was not found to be the case in one study that tested functional connectivity with and without global regression (Rudie et al. 2012) (Table 11.1).
Most of the studies performed to date use data collected during a cognitive task, and it is possible that functional connectivity effects can be driven by task performance that is asymmetric between groups. For example, if an autism population exhibits less activation of the fusiform face area during a facial processing task, then it will be synchronously active during the task with other task-engaged areas to a lesser extent than a control population. Studies using resting-state acquisitions may avoid stimulus-driven changes in connectivity, but it is important to note that the “resting state” is simply another task, albeit less constrained. Subjects can perform vastly different cognitive tasks during the resting state that may have little basis in structural connectivity in the brain. Research continues to evolve on the reliability and biological interpretation of functional connectivity differences.
Likely more significant are the effects of small amounts of uncorrected motion that might have persisted in datasets differentially between patient populations. Such small amounts of motion have been shown to significantly lessen effect sizes of functional connectivity differences during development such as segregation and integration (Power et al. 2012), and these changes are similar to the main effects seen in autism: decreased long-range connectivity. Moreover, correction methods such as despiking or individual frame removal (Power et al. 2012; Van Dijk et al. 2012) were employed in almost none of the studies reviewed. One of the only studies to use more recent techniques for rigorous motion correction was one in which increased connectivity was found, albeit in a domain where autism subjects do not typically show behavioral impairments (Keehn et al. 2012).
Sample sizes have also been small across most of the published studies. Functional connectivity measurements have a large amount of inherent noise, requiring long imaging times or large number of subjects to converge to precise estimates (Anderson et al. 2011a, Ferguson and Anderson 2011). Given the need for characterizing differences in functional connectivity across brain regions, subject age, and other covariates, the multiple comparison problem becomes extreme, and full characterization of connectivity disturbances in autism will likely require much larger pools of data than have been previously used. Fortunately, there have been recent efforts to organize data sharing among laboratories to allow combined datasets with much greater power. The Autism Brain Imaging Data Exchange (http://www.childmind.org/en/healthy-brain-network/abide) has attracted 15 contributing sites, with resting-state data from over 1,000 subjects, with public release of data anticipated for fall 2012. A separate data-sharing initiative, the National Database for Autism Research (http://ndar.nih.gov), has also begun collection of publicly available fMRI data to allow multisite analyses.
Finally, most of the studies performed have characterized functional connectivity in adults. Yet studies that have included children and adolescents have found that connectivity differences tend to be greater in younger subjects, with normalization to the typically developing population beginning around age 20 (Anderson et al. 2011d, Wiggins et al. 2011). Studies in young children are difficult because subjects in the first decade of life are difficult to scan without sleep or sedation and such scans can dramatically affect functional connectivity. Nevertheless, continued exploration of functional connectivity in younger patients is important to characterize the evolution of brain development in autism if diagnosis or prognosis is to be attempted in a clinically relevant time frame by MRI.
11.16 Open Questions
With a broad overview of published results, several important open questions arise.
-
At what age do functional connectivity abnormalities in autism develop?
-
Can functional connectivity be used to characterize the heterogeneity of the autism population by subtyping, predicting prognosis, or establishing endophenotypes?
-
What treatment strategies can be constrained or tested by our knowledge of abnormal connectivity in the autism brain?
-
How do observed functional connectivity patterns affect behavior, stability of distributed brain networks, and cognitive performance?
-
Are functional connectivity patterns genetically determined or the product of experience and training, and can these patterns be modified by interventions?
-
What is the relationship between excitatory and inhibitory neural connections and resulting functional connectivity in autism?
-
At what spatial distances in the brain is “local overconnectivity” present, if at all?
-
What abnormalities are present in between-network functional connectivity in autism?
11.17 Conclusion
Studies of functional connectivity in autism show variable support for a generalized underconnectivity hypothesis in autism. The majority of published studies show deficits in inter-regional brain synchronization involving the default mode network, homotopic left–right connections, and social brain regions that correspond to many of the clinical deficits seen in autism patients. As with the larger functional MRI task-based literature, deficits are most apparent in neural systems associated with impaired function in autism. Connections between networks also show abnormalities, particularly between the default mode and attention control networks. Notable exceptions where overconnectivity in autism has also been reported include the corticostriatal network. Future work will help establish whether these findings may yet be merged into a consistent theory of connectivity anomalies that take into account the spatial distribution of connectivity abnormalities in a heterogeneous population by integrating data from multisite imaging data-sharing initiatives with the power to provide definitive answers to these questions.
References
Adolphs R (2009) The social brain: neural basis of social knowledge. Annu Rev Psychol 60:693–716
Agam Y, Joseph RM, Barton JJ, Manoach DS (2010) Reduced cognitive control of response inhibition by the anterior cingulate cortex in autism spectrum disorders. Neuroimage 52:336–347
Anderson JS, Ferguson MA, Lopez-Larson M, Yurgelun-Todd D (2011a) Reproducibility of single-subject functional connectivity measurements. AJNR Am J Neuroradiol 32:548–555
Anderson JS, Druzgal TJ, Lopez-Larson M, Jeong EK, Desai K, Yurgelun-Todd D (2011b) Network anticorrelations, global regression, and phase-shifted soft tissue correction. Hum Brain Mapp 32:919–934
Anderson JS, Druzgal TJ, Froehlich A, Dubray MB, Lange N, Alexander AL, Abildskov T, Nielsen JA, Cariello AN, Cooperrider JR, Bigler ED, Lainhart JE (2011c) Decreased interhemispheric functional connectivity in autism. Cereb Cortex 21:1134–1146
Anderson JS, Nielsen JA, Froehlich AL, Dubray MB, Druzgal TJ, Cariello AN, Cooperrider JR, Zielinski BA, Ravichandran C, Fletcher PT, Alexander AL, Bigler ED, Lange N, Lainhart JE (2011d) Functional connectivity magnetic resonance imaging classification of autism. Brain 134:3742–3754
Assaf M, Jagannathan K, Calhoun VD, Miller L, Stevens MC, Sahl R, O’Boyle JG, Schultz RT, Pearlson GD (2010) Abnormal functional connectivity of default mode sub-networks in autism spectrum disorder patients. Neuroimage 53:247–256
Baron-Cohen S (1995) Mindblindness: an essay on autism and theory of mind. MIT Press, Cambridge, MA
Belmonte MK, Allen G, Beckel-Mitchener A, Boulanger LM, Carper RA, Webb SJ (2004) Autism and abnormal development of brain connectivity. J Neurosci 24:9228–9231
Bird G, Catmur C, Silani G, Frith C, Frith U (2006) Attention does not modulate neural responses to social stimuli in autism spectrum disorders. Neuroimage 31:1614–1624
Biswal B, Yetkin FZ, Haughton VM, Hyde JS (1995) Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med 34:537–541
Brieber S, Herpertz-Dahlmann B, Fink GR, Kamp-Becker I, Remschmidt H, Konrad K (2010) Coherent motion processing in autism spectrum disorder (ASD): an fMRI study. Neuropsychologia 48:1644–1651
Cherkassky VL, et al (2006) Functional connectivity in a baseline resting-state network in autism. Neuroreport 17:1687–1690
Damarla SR, Keller TA, Kana RK, Cherkassky VL, Williams DL, Minshew NJ, Just MA (2010) Cortical underconnectivity coupled with preserved visuospatial cognition in autism: evidence from an fMRI study of an embedded figures task. Autism Res 3:273–279
Di Martino A, Shehzad Z, Kelly C, Roy AK, Gee DG, Uddin LQ, Gotimer K, Klein DF, Castellanos FX, Milham MP (2009) Relationship between cingulo-insular functional connectivity and autistic traits in neurotypical adults. Am J Psychiatry 166:891–899
Di Martino A, Kelly C, Grzadzinski R, Zuo XN, Mennes M, Mairena MA, Lord C, Castellanos FX, Milham MP (2011) Aberrant striatal functional connectivity in children with autism. Biol Psychiatry 69:847–856
Dinstein I, Pierce K, Eyler L, Solso S, Malach R, Behrmann M, Courchesne E (2011) Disrupted neural synchronization in toddlers with autism. Neuron 70:1218–1225
Ebisch SJ, Gallese V, Willems RM, Mantini D, Groen WB, Romani GL, Buitelaar JK, Bekkering H (2011) Altered intrinsic functional connectivity of anterior and posterior insula regions in high-functioning participants with autism spectrum disorder. Hum Brain Mapp 32:1013–1028
Fair DA, Dosenbach NU, Church JA, Cohen AL, Brahmbhatt S, Miezin FM, Barch DM, Raichle ME, Petersen SE, Schlaggar BL (2007) Development of distinct control networks through segregation and integration. Proc Natl Acad Sci USA 104:13507–13512
Ferguson MA, Anderson JS (2011) Dynamical stability of intrinsic connectivity networks. Neuroimage 59:4022–4031
Fox MD, Raichle ME (2007) Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat Rev Neurosci 8:700–711
Fox MD, Snyder AZ, Vincent JL, Corbetta M, Van Essen DC, Raichle ME (2005) The human brain is intrinsically organized into dynamic, anticorrelated functional networks. Proc Natl Acad Sci USA 102:9673–9678
Fox MD, Zhang D, Snyder AZ, Raichle ME (2009) The global signal and observed anticorrelated resting state brain networks. J Neurophysiol 101:3270–3283
Gotts SJ, et al (2012) Fractionation of social brain circuits in autism spectrum disorders. Brain 135:2711–2725
Jones TB, Bandettini PA, Kenworthy L, Case LK, Milleville SC, Martin A, Birn RM (2010) Sources of group differences in functional connectivity: an investigation applied to autism spectrum disorder. Neuroimage 49:401–414
Just MA, Cherkassky VL, Keller TA, Minshew NJ (2004) Cortical activation and synchronization during sentence comprehension in high-functioning autism: evidence of underconnectivity. Brain 127:1811–1821
Just MA, Cherkassky VL, Keller TA, Kana RK, Minshew NJ (2007) Functional and anatomical cortical underconnectivity in autism: evidence from an FMRI study of an executive function task and corpus callosum morphometry. Cereb Cortex 17:951–961
Kana RK, Keller TA, Cherkassky VL, Minshew NJ, Just MA (2006) Sentence comprehension in autism: thinking in pictures with decreased functional connectivity. Brain 129:2484–2493
Kana RK, Keller TA, Minshew NJ, Just MA (2007) Inhibitory control in high-functioning autism: decreased activation and underconnectivity in inhibition networks. Biol Psychiatry 62:198–206
Kana RK, Keller TA, Cherkassky VL, Minshew NJ, Just MA (2009) Atypical frontal-posterior synchronization of Theory of Mind regions in autism during mental state attribution. Soc Neurosci 4:135–152
Kana RK, Libero LE, Moore MS (2011) Disrupted cortical connectivity theory as an explanatory model for autism spectrum disorders. Phys Life Rev 8:410–437
Keehn B, Shih P, Brenner LA, Townsend J, Muller RA (2012) Functional connectivity for an “Island of sparing” in autism spectrum disorder: an fMRI study of visual search. Hum Brain Mapp. doi:10.1002/hbm.22084
Kennedy DP, Courchesne E (2008a) Functional abnormalities of the default network during self- and other-reflection in autism. Soc Cogn Affect Neurosci 3:177–190
Kennedy DP, Courchesne E (2008b) The intrinsic functional organization of the brain is altered in autism. Neuroimage 39:1877–1885
Kennedy DP, Redcay E, Courchesne E (2006) Failing to deactivate: resting functional abnormalities in autism. Proc Natl Acad Sci USA 103:8275–8280
Kleinhans NM, Richards T, Sterling L, Stegbauer KC, Mahurin R, Johnson LC, Greenson J, Dawson G, Aylward E (2008) Abnormal functional connectivity in autism spectrum disorders during face processing. Brain 131:1000–1012
Koshino H, Carpenter PA, Minshew NJ, Cherkassky VL, Keller TA, Just MA (2005) Functional connectivity in an fMRI working memory task in high-functioning autism. Neuroimage 24:810–821
Koshino H, Kana RK, Keller TA, Cherkassky VL, Minshew NJ, Just MA (2008) fMRI investigation of working memory for faces in autism: visual coding and underconnectivity with frontal areas. Cereb Cortex 18:289–300
Lai MC, Lombardo MV, Chakrabarti B, Sadek SA, Pasco G, Wheelwright SJ, Bullmore ET, Baron-Cohen S, Suckling J (2010) A shift to randomness of brain oscillations in people with autism. Biol Psychiatry 68:1092–1099
Lai G, Pantazatos SP, Schneider H, Hirsch J (2012) Neural systems for speech and song in autism. Brain 135:961–975
Lee PS, Yerys BE, Della Rosa A, Foss-Feig J, Barnes KA, James JD, VanMeter J, Vaidya CJ, Gaillard WD, Kenworthy LE (2009) Functional connectivity of the inferior frontal cortex changes with age in children with autism spectrum disorders: a fcMRI study of response inhibition. Cereb Cortex 19:1787–1794
Liu Y, Cherkassky VL, Minshew NJ, Just MA (2011) Autonomy of lower-level perception from global processing in autism: evidence from brain activation and functional connectivity. Neuropsychologia 49:2105–2111
Lombardo MV, Chakrabarti B, Bullmore ET, Sadek SA, Pasco G, Wheelwright SJ, Suckling J, Baron-Cohen S (2010) Atypical neural self-representation in autism. Brain 133:611–624
Mason RA, Williams DL, Kana RK, Minshew N, Just MA (2008) Theory of Mind disruption and recruitment of the right hemisphere during narrative comprehension in autism. Neuropsychologia 46:269–280
Mizuno A, Villalobos ME, Davies MM, Dahl BC, Muller RA (2006) Partially enhanced thalamocortical functional connectivity in autism. Brain Res 1104:160–174
Mizuno A, Liu Y, Williams DL, Keller TA, Minshew NJ, Just MA (2011) The neural basis of deictic shifting in linguistic perspective-taking in high-functioning autism. Brain 134:2422–2435
Monk CS, Peltier SJ, Wiggins JL, Weng SJ, Carrasco M, Risi S, Lord C (2009) Abnormalities of intrinsic functional connectivity in autism spectrum disorders. Neuroimage 47:764–772
Monk CS, Weng SJ, Wiggins JL, Kurapati N, Louro HM, Carrasco M, Maslowsky J, Risi S, Lord C (2010) Neural circuitry of emotional face processing in autism spectrum disorders. J Psychiatry Neurosci 35:105–114
Mostofsky SH, Powell SK, Simmonds DJ, Goldberg MC, Caffo B, Pekar JJ (2009) Decreased connectivity and cerebellar activity in autism during motor task performance. Brain 132:2413–2425
Muller RA, Shih P, Keehn B, Deyoe JR, Leyden KM, Shukla DK (2011) Underconnected, but how? A survey of functional connectivity MRI studies in autism spectrum disorders. Cereb Cortex 21:2233–2243
Murphy K, Birn RM, Handwerker DA, Jones TB, Bandettini PA (2009) The impact of global signal regression on resting state correlations: are anti-correlated networks introduced? Neuroimage 44:893–905
Narayanan A, White CA, Saklayen S, Scaduto MJ, Carpenter AL, Abduljalil A, Schmalbrock P, Beversdorf DQ (2010) Effect of propranolol on functional connectivity in autism spectrum disorder–a pilot study. Brain Imaging Behav 4:189–197
Noonan SK, Haist F, Muller RA (2009) Aberrant functional connectivity in autism: evidence from low-frequency BOLD signal fluctuations. Brain Res 1262:48–63
Paakki JJ, Rahko J, Long XY, Moilanen I, Tervonen O, Nikkinen J, Starck T, Remes J, Tuula H, Haapsamo H, Jussila K, Kuusikko-Gauffin S, Mattila ML, Zang YF, Kiviniemi V (2010) Alterations in regional homogeneity of resting-state brain activity in autism spectrum disorders. Brain Res 1329:169–179
Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE (2012) Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. Neuroimage 59:2142–2154
Rubchinsky LL, Kopell N, Sigvardt KA (2003) Modeling facilitation and inhibition of competing motor programs in basal ganglia subthalamic nucleus-pallidal circuits. Proc Natl Acad Sci USA 100:14427–14432
Rudie JD, Shehzad Z, Hernandez LM, Colich NL, Bookheimer SY, Iacoboni M, Dapretto M (2012) Reduced functional integration and segregation of distributed neural systems underlying social and emotional information processing in autism spectrum disorders. Cereb Cortex 22:1025–1037
Sahyoun CP, Belliveau JW, Soulieres I, Schwartz S, Mody M (2010) Neuroimaging of the functional and structural networks underlying visuospatial vs. linguistic reasoning in high-functioning autism. Neuropsychologia 48:86–95
Schipul SE, Keller TA, Just MA (2011) Inter-regional brain communication and its disturbance in autism. Front Syst Neurosci 5:10
Schipul SE, Williams DL, Keller TA, Minshew NJ, Just MA (2012) Distinctive neural processes during learning in autism. Cereb Cortex 22:937–950
Scott-Van Zeeland AA, Abrahams BS, Alvarez-Retuerto AI, Sonnenblick LI, Rudie JD, Ghahremani D, Mumford JA, Poldrack RA, Dapretto M, Geschwind DH, Bookheimer SY (2010) Altered functional connectivity in frontal lobe circuits is associated with variation in the autism risk gene CNTNAP2. Sci Transl Med 2:56ra80
Seeley WW, Menon V, Schatzberg AF, Keller J, Glover GH, Kenna H, Reiss AL, Greicius MD (2007) Dissociable intrinsic connectivity networks for salience processing and executive control. J Neurosci 27:2349–2356
Shih P, Shen M, Ottl B, Keehn B, Gaffrey MS, Muller RA (2010) Atypical network connectivity for imitation in autism spectrum disorder. Neuropsychologia 48:2931–2939
Shukla DK, Keehn B, Muller RA (2010) Regional homogeneity of fMRI time series in autism spectrum disorders. Neurosci Lett 476:46–51
Solomon M, Ozonoff SJ, Ursu S, Ravizza S, Cummings N, Ly S, Carter CS (2009) The neural substrates of cognitive control deficits in autism spectrum disorders. Neuropsychologia 47:2515–2526
Turner KC, Frost L, Linsenbardt D, McIlroy JR, Muller RA (2006) Atypically diffuse functional connectivity between caudate nuclei and cerebral cortex in autism. Behav Brain Funct 2:34
Uddin LQ, Menon V (2009) The anterior insula in autism: under-connected and under-examined. Neurosci Biobehav Rev 33:1198–1203
Van Dijk KR, Sabuncu MR, Buckner RL (2012) The influence of head motion on intrinsic functional connectivity MRI. Neuroimage 59:431–438
Villalobos ME, Mizuno A, Dahl BC, Kemmotsu N, Muller RA (2005) Reduced functional connectivity between V1 and inferior frontal cortex associated with visuomotor performance in autism. Neuroimage 25:916–925
Vissers ME, Cohen MX, Geurts HM (2012) Brain connectivity and high functioning autism: a promising path of research that needs refined models, methodological convergence, and stronger behavioral links. Neurosci Biobehav Rev 36:604–625
von dem Hagen EA, Stoyanova RS, Baron-Cohen S, Calder AJ (2012) Reduced functional connectivity within and between ‘social’ resting state networks in autism spectrum conditions. Soc Cogn Affect Neurosci. doi:10.1093/scan/nss053
Welchew DE, Ashwin C, Berkouk K, Salvador R, Suckling J, Baron-Cohen S, Bullmore E (2005) Functional disconnectivity of the medial temporal lobe in Asperger’s syndrome. Biol Psychiatry 57:991–998
Weng SJ, Wiggins JL, Peltier SJ, Carrasco M, Risi S, Lord C, Monk CS (2010) Alterations of resting state functional connectivity in the default network in adolescents with autism spectrum disorders. Brain Res 1313:202–214
Wicker B, Fonlupt P, Hubert B, Tardif C, Gepner B, Deruelle C (2008) Abnormal cerebral effective connectivity during explicit emotional processing in adults with autism spectrum disorder. Soc Cogn Affect Neurosci 3:135–143
Wiggins JL, Peltier SJ, Ashinoff S, Weng SJ, Carrasco M, Welsh RC, Lord C, Monk CS (2011) Using a self-organizing map algorithm to detect age-related changes in functional connectivity during rest in autism spectrum disorders. Brain Res 1380:187–197 Biography
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer New York
About this chapter
Cite this chapter
Anderson, J.S. (2013). Functional Connectivity MRI in Autism. In: Casanova, M., El-Baz, A., Suri, J. (eds) Imaging the Brain in Autism. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-6843-1_11
Download citation
DOI: https://doi.org/10.1007/978-1-4614-6843-1_11
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-6842-4
Online ISBN: 978-1-4614-6843-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)