
Abstract
Research on predictors of Intimate Partner Violence (IPV) in Sub-Saharan Africa is contradictory, necessitating further investigation. This study sought the prevalence and predictors of IPV among women in Lagos, Nigeria. Questionnaire data from 934 women visiting an obstetrics and gynecology clinic in Lagos were analyzed using multivariable methods. The 1 year prevalence of IPV was 29%, with significant proportions reporting psychological (23%), physical (9%) and sexual (8%) abuse. In-access to information, women’s autonomy and contribution to household expenses independently predicted IPV. The findings provide new incites for IPV prevention in Lagos with implications for further research.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Background
Intimate Partner Violence (IPV) is defined as a pattern of assaultive and coercive behaviors, including physical, sexual and psychological attacks, as well as economic coercion that adults or adolescents use against their intimate partners (Ganley and Schechter 1996). Though intimate partner violence can be seen at all societies, socioeconomic groups, races and sexes, the prevalence may vary depending on these factors (WHO 2002).
Globally, lifetime prevalence rates of IPV among women vary between 10–69%, and population studies indicate that at least one woman in every three has been beaten, coerced into sex, or otherwise abused in her lifetime (WHO 2002; Heise et al. 1999). In developing countries life-time prevalence ranging between 11–52% and yearly prevalence between 4–29% have been reported (Gage 2005; Kishor and Johnson 2004; Jewkes et al. 2002; Ellsberg et al. 1999; Koenig et al. 2003a, b). IPV is documented as the third leading cause of mortality among women aged between 15–44 years and is a major cause of morbidity with health consequences ranging from injuries to reproductive health complications (Lemmey et al. 2001; WHO 2002; Heise 1994; Emenike et al. 2008).
Although studies show that there is not much disparity between prevalence rates in developed and developing countries, developing countries are known to have peculiar risk factors that appear to endorse and perpetuate IPV such as patriarchal social structure (Garcia-Moreno et al. 2005).
Theoretical Framework for Risk Factors of IPV
Several theories have been suggested to explain factors possibly associated with vulnerability and perpetration of IPV. By far the most comprehensive explanation for risk factors of IPV is based on the social ecological framework, where immediate and remote factors associated with IPV perpetration and vulnerability are distinguished at five levels namely individual, relational, organizational, community and policy levels (Little and Kaufman 2002). The first level, intrapersonal or individual, comprises factors, such as biological sex, age, social economic status (SES), substance use, and cultural identity. Studies show that there is a higher vulnerability to IPV among women than men, with consequent graver outcomes for women, including physical injury and impaired reproductive health outcomes (Rennison and Welchans 2000; Emenike et al. 2008). Moreover, being of reproductive age (Fairchild et al. 1998) and engagement in health risk behavior such as alcohol and drug abuse (Heise and Garcia-Moreno 2002; Silverman et al. 2001) are factors associated with increased vulnerability for and perpetration of IPV. While there is a consensus that socio-economic status is related to IPV vulnerability, the direction of association remains a subject of contention. Some studies have found high SES among women to be a protective factor against abuse (Jewkes et al. 2002; Lawoko 2006) while others have suggested the contrary (Chakwana 2004; Zimbabwe Demographic and Health Survey 2006 [ZDHS 2006]). A plausible explanation for this discrepancy could be differences in women’s normative roles between societies. While in some societies women’s structural empowerment (e.g., involvement in income generating activities and education) may be seen to boost family income and therefore reduce risk for poverty-related conflict, in other societies such empowerment may conflict with women’s normative roles (e.g., being housewives and domestic workers), thereby increasing the risk for aggression. Divergence from gender roles thus may be important in eliciting IPV.
At the relational level, gender roles and family bonding seem to play a fundamental role in IPV vulnerability and perpetration (Oetzel and Duran 2004). Gender role refers to a set of perceived behavioral norms associated particularly with males or females, in a given social group or system. Subversion from such norms is likely to increase vulnerability to IPV. Family bonding is another factor at the relational level responsible for IPV exposure. Research shows that women are hesitant to leave abusive relationships due to concern for leaving their children behind, or are unsure of survival and coping if they take the children along (Little and Kaufman 2002; Stephens 1999). Also at the relational level, differences between couples with regard to educational achievement, age and carrier development may increase vulnerability to IPV.
The third level of the ecological model, the organisational/institutional level, is significant not only in the identification of institutional factors associated with IPV exposure but also in primary and secondary prevention of the problem. Self reports from women indicate that they are content when healthcare professionals address IPV in healthcare settings (Stenson et al. 2001, 2005). Reciprocating this, healthcare professionals themselves acknowledge that routine screening for IPV in healthcare is likely to improve identification of IPV and with it appropriate referral for prevention (Furniss et al. 2007; Bair-Merritt et al. 2006). Thus, the grade to which relevant organizations are willing to address women’s issues may influence the identification and eventual control of IPV in that society.
The fourth level of the ecological model, the community level, purports that IPV vulnerability may result from factors inherent in social relationships at the community level and how such factors may conflict with norms governing intimacy. Certain groups in society, such as ethnic (Chester et al. 1994; Hamby 2000) and religious groups (Levitt and Ware 2006) tend to be more gender restrictive, conditioning women to agree or consent to wife beating. Moreover, patriarchal structure in many societies, particularly in the developing country context, remains a recurrent decimal in the list of known risk factors for IPV (Garcia-Moreno et al. 2005).
The final level of the ecological model, policy, helps to explain how social policies that maintain economic or social inequalities between groups in society could in fact contribute to IPV vulnerability and perpetration. In most developing countries laws protecting victims of IPV are non existent, non-enforced or more lenient than necessary. Moreover, because religious and cultural norms put women in a subordinate position in many societies (Chester et al. 1994; Hamby 2000; Levitt and Ware 2006), there are laws that literally accept punishment of women for deviations from expected religious/cultural gender norms. In Northern Nigeria for example, Section 55 of the Penal Code allows a husband to “discipline” his wife so long as the action does not amount to the “infliction of grievous hurt” (Feminist.com, 2006). Policy thus becomes an important promoter of IPV when it should ideally be used as a remedy against the practice.
IPV in the Sub-Saharan African Context
IPV in Sub-Saharan Africa has been researched from varying perspectives ranging from rights, feminist, cultural and society in transition theories. Few studies have also explored the phenomena from a social or structural empowerment perspective (Okenwa and Lawoko 2009; Lawoko 2006). The role of structural empowerment in vulnerability for IPV, however, remains elusive. Though there is a consensus that structural empowerment factors may be associated with IPV, the direction of association has not been consistently demonstrated. While some studies from the Sub-Saharan African context have supported the notion that poor socioeconomic conditions e.g., less schooling and unemployment (Jewkes et al. 2002; Lawoko 2006) among women may be associated with increased vulnerability; others from the same context have instead indicated increased vulnerability among socially empowered women such as employed women (Chakwana 2004; Zimbabwe Demographic & Health Survey 2006 [ZDHS 2006]). These discrepancies warrant careful scrutiny of social factors associated with IPV vulnerability in each specific Sub-Saharan African country. Moreover, even within the same country, variations in social (e.g., religion) and cultural conditions may exist (e.g., religious and ethnic belonging) and with it differences in IPV exposure and risk factors. Indeed, examples from other developing societies seem to point in that direction. After stratifying their analysis by two main geographical parts of the Bangladesh that differ culturally (one culture more conservative than the other), Koenig et al. (2003a, b) found that financial empowerment of women was significantly related to greater risk of IPV in the more conservative region but with lower risk in the less conservative region.
In summary, these data suggest that IPV vulnerability in Sub-Saharan Africa may differ depending on differences in women’s normative roles and men’s expectations of them between the societies. The direction of association between IPV exposure and social factors is thus likely to vary between countries. Moreover, such differences may even exist between different regions within a given country. These differences could have implications for how to shape prevention strategies for IPV specific to a given society. In this paper, we will study the factors associated with IPV vulnerability among women in Lagos, Nigeria, and based on our findings, suggest appropriate intervention to manage IPV in that region.
Aim and Specific Objectives
Basing largely on the ecological framework of IPV, the overall aim of this paper is to study the association between exposure to IPV and individual, relational and societal factors. More specifically the study will scrutinize exposure to IPV among women in Lagos, Nigeria in relation to individual factors (e.g., age, educational achievement and literacy), relational/familial factors (e.g., financial difficulties in the household and power to make household decisions) and societal factors (e.g., ethnicity and religion).
Methods
Study Design and Setting
This study was conducted at the obstetrics and gynaecology department of the Lagos University Teaching Hospital (LUTH), Nigeria utilizing a cross section of the women attending the clinic.
Sampling Procedure and Participants
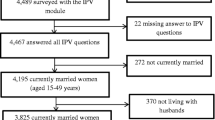
Systematic sampling was used to select a sample of women totaling 934, aged 15–49 years visiting the O&G clinic of LUTH. The sample size necessary was established using a power analysis, assuming a binomial distribution. A sample size of about 900, statistical significance level of alpha = 0.05, and an estimated average yearly probability of IPV occurring in developing countries of 0.125, based on data from several countries would be appropriate to secure a statistical power of over 0.90 considered as very good. Participating woman under the guidance of trained personal responded to a questionnaire comprising of previously validated questions.
Questionnaire
A structured questionnaire covering demographic and health issues was administered to the eligible women. The questionnaire covered; women and husband’s background, reproductive history, utility of family planning methods, fertility preferences, child mortality, awareness of and precaution against sexually transmitted diseases, marriage and sexual behavior, attitudes towards IPV, disclosure of IPV, psychosocial health outcomes, demographic and social status indicators, and domestic violence. For the current paper, the questions of primary interest were those on domestic violence, demographics and social indicators.
Measures Used in Current Study
Dependent Variable
The dependent variable in this study was Intimate Partner Violence (IPV), which was assessed using a modified version of the Conflict Tactic Scale (CTS) (Straus and Gelles 1990). The CTS assesses whether participants have experienced physical, psychological and sexual abuse perpetrated by the current husband/partner during the latest year or ever. For this study, experience of IPV latest year was of primary interest to study the predictors of IPV. Physical abuse was operationalized as being slapped, pushed, punched, choked, burnt on purpose, kicked and assaults using knife, or other weapons. Psychological abuse included being insulted, made to feel bad about self, belittled in front of other people, scared or intimidated, threatened with violence or threats of violence directed towards someone you care about. Sexual abuse included being physically forced to have sexual intercourse when she did not want to; having intercourse out of fear or forced to do sexual degrading or humiliating sexual act. In this study, a victim of IPV was a woman who has experienced at least one of the forms of abuse described above. In the logistic regressions analyses, exposure to IPV during the latest year was used as the dependent variable.
Independent Variables
Independent variables used included the following for which response alternatives are presented in brackets: age; literacy (1 = can read little or nothing, 2 = can read whole sentences); religion (1 = Catholic, 2 = Protestant, 3 = Muslim, 4 = others); ethnicity (1 = Yoruba, 2 = Ibo, 3 = others); employment (1 = yes, 2 = no); working at home (1 = yes, 2 = no) access to information i.e. reads paper, listens to radio, watches TV (1 = almost everyday, 2 = at least once weekly, 3 = less than once weekly, 4 = almost never/not at all); respondent’s and partners use of alcohol; smoking habits; (1 = yes, 2 = no); husband practices polygamy (1 = yes, 2 = no); participation in decision making i.e. say on money use, health care, household purchase etc (1 = complete say, 2 = partial say, 3 = no say); financial participation i.e. contribution to household purchase financial difficulties i.e. problems making ends meet and problems managing monthly expenditures (1 = yes, 2 = no).
Ethical Considerations
Ethical approval for the study was granted by the Nigerian Institute of Medical Research, NIMR after due protocol. Moreover, local clearance to administer the questionnaire was sought and received at the department of obstetrics and gynaecology.
The domestic violence module used was adapted from the Demographic and Health Surveys module and the WHO questionnaire on violence often used for developing countries. These surveys strictly adhere to the standards for ethical and safety recommendations for research on domestic violence set by the World Health Organization (WHO). The recommendations aim to ensure women’s safety and at the same time maximizing disclosure of actual violence, promoted among other things by offering adequate training and support to field workers together with informed consent and guarantee of privacy to respondents (WHO 2001).
Statistical Analyses
The SPSS program version 15.0 was used for imputing and analysis of data. In the univariate analyses, chi-square test was used to assess associations between IPV exposure and the independent variables. Logistic regression was used in the multivariable analysis to assess the independent contribution of the explanatory variables while adjusting for possible confounding. The direction and magnitude of associations were expressed as adjusted odds ratio. The significance level was set at p < 0.05 for all statistical analysis.
Results
One Year Prevalence of IPV
The 1 year prevalence of IPV was high with significant proportions reporting exposure to any form of abuse (29.1%; any form implies at least one of physical, psychological or sexual abuse), physical abuse (8.6%), psychological abuse (22.8%) and sexual abuse (8.3%).
Univariate Associations Between IPV Exposure and Demographics, Financial Difficulties, Decision/Financial Participation, Access to Information and Behavioral Variables
As shown in Table 1, demographic variables were associated with vulnerability to IPV. The proportion exposed to physical violence reduced with increasing education (χ2(2) = 10.1; p < 0.01) and literacy (χ2(1) = 5.3; p < 0.05). Religion was associated with sexual abuse (χ2(3) = 14.2; p < 0.01) and any form of abuse (χ2(3) = 14.6; p < 0.01), with the highest proportions of abused women among catholic. Women having at least one child were more likely to report exposure to psychological abuse (χ2 (1) = 5.6; p < 0.05) and any abuse (χ2 (1) = 5.8; p < 0.05). Polygamy appeared to be a relevant factor in exposure as respondents in polygamous relationships were more likely to report exposure to physical abuse (χ2 (1) = 18.1; p < 0.001). While unemployment increased vulnerability to physical abuse (χ2 (1) = 4.2; p < 0.05), working from home was associated with an increased likelihood of experiencing physical abuse (χ2 (1) = 4.1; p < 0.05) and any kind of violence (χ2 (1) = 4.1; p < 0.05).
Financial difficulties were associated with IPV exposure. Problems making ends meet was associated with an increased likelihood for physical (χ2 (1) = 5.1; p < 0.05), psychological (χ2 (1) = 12.8; p < 0.001), sexual (χ2 (1) = 6.4, p < 0.05) and any form of IPV (χ2 (1) = 11.0, p < 0.01). Likewise, problems managing monthly expenditures was associated with an increased likelihood for physical abuse (χ2 (1) = 7.9; p < 0.01), psychological abuse (χ2 (1) = 7.5; p < 0.01) and the risk for any form of violence (χ2 (1) = 4.4; p < 0.05).
Table 1 also shows that decision participation was related with IPV exposure. Having a say on money use in the household was associated with an increased likelihood for physical (χ2 (2) = 10.3; p < 0.01) and sexual abuse (χ2 (2) = 15.8; p < 0.001). In addition, having a say on household purchases increased likelihood of psychological abuse (χ2 (2) = 6.1; p < 0.05). Women with complete say with regard to visiting family/friends were more often than colleagues without such autonomy exposed to physical (χ2 (2) = 14.9; p < 0.001), psychological (χ2 (2) = 6.9; p < 0.05), sexual; (χ2 (2) = 10.2; p < 0.01) and any form of abuse (χ2 (2) = 11.8; p < 0.01). In addition, women having full autonomy over the number of children to have and when to have them where more likely to report physical violence; (χ2 (2) = 18.0; p < 0.001); sexual violence; (χ2 (2) = 14.2; p < 0.001) and all kinds of violence combined in the past year (χ2 (2) = 18.0, p < 0.001).
Behavioral factors were associated with IPV exposure. Alcohol consumption among women increased exposure to physical (χ2 (1) = 5.4; p < 0.05), sexual (χ2 (1) = 7.8; p < 0.01) and any form of abuse (χ2 (1) = 5.6; p < 0.05). The same trend was observed among women whose husbands consumed alcohol. Women whose husbands consume alcohol were more likely to experience physical (χ2 (1) = 6.1; p < 0.05), sexual (χ2 (1) = 6.2; p < 0.05) and any form of abuse (χ2 (1) = 5.8, p < 0.05) than peers whose husbands did not drink. In the same vein, women with smoker husbands were more likely to experience physical (χ2 (1) = 20.0; p < 0.001), sexual (χ2 (1) = 5.8; p < 0.05) and any form of violence (χ2 (1) = 9.8; p < 0.01).
As also shown on Table 1, access to information was related with IPV exposure. Reading newspapers was associated with physical abuse (χ2(3) = 24.4; p < 0.001) and any form of abuse (χ2(3) = 10.6; p < 0.05), with the highest proportions of abused women observed among those who seldom/never read newspapers.
Logistic Regression of IPV Exposure Using Demographics, Financial Difficulties, Decision/Financial Participation, Behavioral Variables and Access to Information as Independent Variables
As indicated (see below) in Table 2, demographic variables such as age and having children remained significantly associated with IPV after adjusting for possible confounding with other study independent variables. Contrasting with peers 25–44 years of age, women aged 15–24 years were more likely to experience physical abuse, sexual abuse, and any abuse. Having a child increased likelihood of experiencing psychological abuse and any form of abuse. All other variables in Table 2 did not impact significantly on likelihood of IPV when possible confounding was adjusted for.
From Table 3, it can be seen that financial difficulties i.e. problems managing monthly expenditure remained significantly associated with IPV after adjusting for possible confounding with other study independent variables. Having such problems increased likelihood of experiencing physical abuse. All other variables in Table 3 did not impact significantly on likelihood of IPV when possible confounding was adjusted for.
Decision and financial participation variables i.e. say on money use, say on visiting and contribution to household expenses remained significantly associated with IPV after adjusting for possible confounding with other study independent variables (Table 4). Having full autonomy on decisions regarding spending household money increased likelihood of sexual abuse. Contribution to household expenditure increased likelihood of physical, psychological, sexual and any form of abuse. All other variables in Table 4 did not impact significantly on likelihood of IPV when possible confounding was adjusted.
As indicated in Table 5, none of the behavioral variables impacted significantly on likelihood of IPV when possible confounding was adjusted for.
As indicated in Table 6, access to information (i.e., reading newspaper and watching TV) remained significantly associated with IPV after adjusting for possible confounding with other study independent variables. Inability to read newspaper increased likelihood of physical abuse, while limited access to TV increased likelihood of psychological and sexual abuse. All other variables in Table 6 did not impact significantly on likelihood of IPV when possible confounding was adjusted for.
Discussion
This study aimed primarily at estimating the 1 year prevalence and scrutinizing risk factors for Intimate Partner Violence (IPV) against women in Lagos, Nigeria. Potential risk factors investigated were categorized under demographics, financial difficulties, financial participation, decision participation, behavioral factors and access to information. Results revealed a yearly prevalence of IPV ranging between 8–29%, corroborating results from other Sub-Saharan African countries (Jewkes et al. 2002; Koenig et al. 2003a, b). Consistent with previous observations (Obi and Ozumba 2007; Ezechi et al. 2004), the most common form of violence in this sample was psychological abuse (22.8%). The high yearly prevalence of IPV among women in this clinical sample demonstrates the need for screening for IPV in healthcare settings with the aim of making appropriate referral for IPV victims. Indeed, research emerging from the developed countries suggests that female clients (Stenson et al. 2001, 2005) and their healthcare providers (Furniss et al. 2007; Bair-Merritt et al. 2006) endorse screening for IPV in healthcare as a remedy for its eventual management.
The study of risk factors for IPV has received considerable attention in the literature and the current data adds to the growing literature indicating that demographic factors such as low age and having children are independently associated with increased vulnerability to IPV. That having children increases IPV vulnerability could be explained by the social bonding theory. Some authors (Little and Kaufman 2002; Romans et al. 2006) have observed that family bonding is significant in women’s choice to remain in abusive relationships. In the Sub-Saharan African context where the husband remains the breadwinner, this problem is particularly cumbersome as women worry about their children’s welfare when considering separation.
Women’s behaviors (i.e., alcohol consumption) increased vulnerability to IPV. Moreover, women whose partners used alcohol or smoked were more likely to experience abuse. These findings are in line with previous work in the field (Silverman et al. 2001). The multivariate analysis could not however confirm these factors as independent risk factors of IPV, suggesting that possible confounding with other study variables may have been an issue. Future research in the field may need to consider careful analysis of variables possibly confounding or mediating the relationship between IPV exposure and behavioral factors.
The role of social and structural empowerment indicators in eliciting of IPV remains an area of controversy when viewed in general in the Sub-Saharan African context. Our results provide evidence suggesting that empowerment indicators, such as education, literacy, employment, and family financial stability, may be a protective factor against IPV, corroborating some data from the Sub-Saharan African context (Jewkes et al. 2002; Lawoko 2006; Lawoko et al. 2007) but contradicting others (Chakwana 2004; Zimbabwe Demographic and Health Survey 2006 [ZDHS 2006]). However, the multivariate analysis could not confirm education, literacy, employment as independent risk factors for IPV. This suggests that further investigation of possible confounding variables in future research may provide deeper insight on the relationship between IPV and these empowerment indicators. On the other hand, other empowerment indicators such as participation in household decisions and contribution to household expenses increased women’s vulnerability to IPV even after adjustment for possible confounding in the multivariate analyses, inconsistent with some previous findings (Aimakhu et al. 2004; Obi and Ozumba 2007) but supporting others (e.g., Koenig et al. 2003a, b). These results may be a reflection of circumstances where women’s involvement in domestic affairs that are traditionally seen as men’s roles in some societies (e.g., decision making and breadwinning) is likely to cause spousal conflicts, reflected here in the form of domestic violence. Overall, these findings suggest that the relationship between IPV and social and structural empowerment indicators is complex. For these reasons, each empowerment indicator and their role in IPV deserve an assessment on their own right in each unique society. With regard to the Lagos, Nigerian context, it seems that while social empowerment of women outside the home (e.g., education and employment) may provide protection against IPV, empowerment in the domestic arena (i.e. participation in domestic decisions and participation in domestic expenses) may increase IPV vulnerability.
There is a consensus in the literature that access to information via mass media is likely to reduce vulnerability to IPV (Okenwa and Lawoko 2009) and the current data seems to point in that direction, as exposure to newspapers and television reduced vulnerability to IPV. Whether it is exposure to mass media per se or whether the mass media addresses issues relating to women’s empowerment however has so far been an area of peripheral discussion. Future research on the content of information channeled via mass media may provide further insight in understanding the mechanism linking limited mass media exposure to IPV vulnerability.
The current results have important implications for prevention of IPV in Lagos and similar socio-cultural context. Enlightening women through education and mass media exposure may come a long way in reducing IPV. It appears that women-focused interventions on their own may not be appropriate in some cases. Interventions directed toward empowering of women in their autonomy and participation in the domestic arena need to consider a re-orientation towards the women’s partners. A concerted campaign to change men’s attitudes towards women’s domestic participation is warranted. Such campaign could emphasis the benefits of women’s involvement and participation in empowering the family unit as a whole. The women themselves need to review their own attitudes toward abuse. Comparative studies between men and women have suggested that women tend to endorse wife beating to a higher degree than the men themselves.
The study also has important implications for research. As the multivariate analysis could not firmly confirm the association between IPV on the one hand and education, literacy, employment and alcohol consumption on the other, it follows that further research assessing possible confounders or mediators linking these variables to IPV exposure is warranted.
The strength of this study lies in its careful methodology, strict adherence to ethical issues regarding data collection on IPV in accordance with WHO recommendations and careful interpretation of the finding reported herein. The weaknesses of the study however deserve to be acknowledged on their own right. First, the study only inquired if women had been abused and did not incorporate women’s own use of violence. Whether the respondent had been abused in retaliation to violence from the respondent herself is not known. Future research needs to distinguish between female victims only and female victims and who may also be perpetrators. Second, our study was based on clinical samples. Even though the findings seem congruent with research from non-clinical samples, generalization to and comparisons with non-clinical samples needs to be done with caution. Moreover, all women who participated in the study happened to have at least a primary education, suggesting some form of selection bias. It seems that women with no education at all may be grossly underrepresented as attendants of the LUTH clinic. Considering that Nigeria has an adult urban literacy rate of about 71%, we would have expected to capture some cases of non-educated women in our data. The findings of this study should therefore be interpreted to represent women presenting at an urban university hospital. In addition, the religion and ethnicity variables have an option “others” which clumps together all other religions (i.e., apart from Protestants, Catholics and Muslims) and all other tribes (apart from Yoruba and Ibo). As there were few from the smaller tribes, this was a strategy to increase the statistical power of the analysis with regard to these variables. The level of homogeneity in the option “other” can thus be questioned and may have affected the results with regards to these variables. For these reasons, we have refrained from deep interpretation and discussion of these two variables. Finally, the cross-sectional design of this study does not allow for causal interpretation. Studies with a more powerful design (e.g., longitudinal studies) are warranted to confirm causal links. All in all, as most of our results are in line with previous research in the field, the study carries a good grade of validity despite the weaknesses outlined herein.
References
Aimakhu, C. O., Olayemi, O., Iwe, C. A., Oluyemi, F. A., Ojoko, I. E., Shoretire, K. A., et al. (2004). Current causes and management of violence against women in Nigeria. Journal of Obstetrics & Gynaecology, 24(1), 58–63. doi:10.1080/01443610310001620314.
Bair-Merritt, M. H., Mollen, C. J., Yau, P. L., & Fein, J. A. (2006). Health care providers’ opinions on intimate partner violence resources and screening in a pediatric emergency department. Pediatric Emergency Care, 22(3), 150–153. doi:10.1097/01.pec.0000202455.26861.4b.
Chakwana, C. D. (2004). Domestic violence. Malawi Demographic and health survey report. pp. 265–280.
Chester, B., Robin, R. N., Koll, M. P., Lopez, J., & Goldman, D. (1994). Grandmother dishonored: violence against women by male partners in American aboriginal communities. Violence and Victims, 9(3), 249–258.
Ellsberg, M. C., Pena, R., Herrera, A., Liljestrand, J., & Winkvist, A. (1999). Wife abuse among women of childbearing age in Nicaragua. American Journal of Public Health, 89(2), 241–244. doi:10.2105/AJPH.89.2.241.
Emenike, E., Lawoko, S., & Dalal, K. (2008). Intimate Partner Violence and Reproductive health of women in Kenya. International Nursing Review, 55(1), 97–102. doi:10.1111/j.1466-7657.2007.00580.x.
Ezechi, O. C., Kalu, B. K., Ezechi, L. O., Nwokoro, C. A., Ndububa, V. I., & Okeke, G. C. (2004). Prevalence and pattern of domestic violence against pregnant Nigerian women. Journal of Obstetrics & Gynaecology, 24(6), 652–656. doi:10.1080/01443610400007901.
Fairchild, D. G., Fairchild, M. W., & Stoner, S. (1998). Prevalence of adult domestic violence among women seeking routine care in a Native American health care facility. American Journal of Public Health, 88(10), 1515–1517. doi:10.2105/AJPH.88.10.1515.
Furniss, K., McCaffrey, M., Parnell, V., & Rovi, S. (2007). Nurses and barriers to screening for intimate partner violence. MCN. The American Journal of Maternal Child Nursing, 32(4), 238–243. doi:10.1097/01.NMC.0000281964.45905.89.
Gage, A. (2005). Women’s experience of intimate partner violence in Haiti. Social Science & Medicine, 61(2), 343–364. doi:10.1016/j.socscimed.2004.11.078.
Ganley, A. L., & Schechter, S. (1996). Domestic Violence: A National Curriculum for Child Protective Services. San Francisco, CA: Family Violence Prevention Fund.
Garcia-Moreno, C., Jansen, H. E., Ellsberg, M., Heise, L., & Watts, C. H. (2005). The WHO multi-country study on women’s health and domestic violence against women: initial findings on prevalence, health consequences and women’s responses.
Hamby, S. L. (2000). The importance of community in a feminist analysis of domestic violence among American Indians. American Journal of Community Psychology, 28, 649–669. doi:10.1023/A:1005145720371.
Heise, L. (1994). Gender-based abuse: the global epidemic. Cadernos de Saude Publica, 10, 135–145. doi:10.1590/S0102-311X1994000500009.
Heise, L., & Garcia-Moreno, C. (2002). Violence by intimate partners. In: Krug E, Dahlberg L. L., Heise, L. L. (1988). Violence against women: an integrated ecological framework. Violence Against Women, 3, 262–290.
Heise, L., Ellsberg, M., & Gottenmoeller, M. (1999). Ending violence against women. Population Reports Series, L(11).
Jewkes, R., Penn-Kekana, L., & Levin, J. (2002). Risk factors for domestic violence: findings from a South African cross-sectional study. Social Science & Medicine, 55, 1603–1720. doi:10.1016/S0277-9536(01)00294-5.
Kishor, S., & Johnson, K. (2004). Profiling violence: A multi-country study. Measures DHS, ORC Marco; pp. 53–63.
Koenig, M. A., Ahmed, S., Hossain, M. B., & Khorshed, A. B. (2003a). Women’s status and domestic violence in rural Bangladesh: individual and community-level effects. Demography, 40, 269–288. doi:10.1353/dem.2003.0014.
Koenig, M. A., Lutalo, T., Zhao, F., Nalugoda, F., Wabwire-Mangen, F., Kiwanuka, N., et al. (2003b). Domestic violence in rural Uganda: evidence from a community-based study. Bulletin of the World Health Organization, 81, 53–60.
Lawoko, S. (2006). Factors associated with attitudes towards violence: a study of women in Zambia. Violence and Victims, 21, 645–656. doi:10.1891/vivi.21.5.645.
Lawoko, S., Dalal, K., Jiayou, L., & Jansson, B. (2007). Social inequality in intimate partner violence: a study of women in Kenya. Violence and Victims, 22(6), 773–784. doi:10.1891/088667007782793101.
Lemmey, D., McFarlane, J., Wilson, P., & Malecha, A. (2001). Intimate partner violence.Mothers’ perspectives of effects on their children. MCN The American Journal of Maternal Child Nursing, 26(2), 98–103.
Levitt, H. M., & Ware, K. (2006). “Anything with two heads is a monster”: religious leaders’ perspectives on marital equality and domestic violence. Violence against Women, 12(12), 1169–90.
Little, L., & Kaufman, K. G. (2002). Using ecological theory to understand intimate partner violence and child maltreatment. Journal of Community Health Nursing, 19, 133–145.
Obi, S. N., & Ozumba, B. C. (2007). Factors associated with domestic violence in south-east Nigeria. Journal of Obstetrics and Gynaecology, 27(1), 75–78.
Oetzel, J., & Duran, B. (2004). Intimate partner violence in American Indian and/or Alaska Native communities: a social ecological framework of determinants and interventions. American Indian and Alaska Native Mental Health Research, 11, 49–68.
Okenwa, L., & Lawoko, S. (2009). Social indicators and Intimate Partner Violence: A study of women in Zambia. Violence and Victims.
Rennison, C. M., & Welchans, S. (2000). Criminal victimization 1999: Changes.
Romans, S., Forte, T., Cohen, M. M., Du Mont, J., & Hyman, I. (2006). Who is most at risk for intimate partner violence?: a Canadian population-based study. Journal of Interpersonal Violence, 22(12), 1495.
Silverman, J., Raj, A., Mucci, L., & Hathaway, J. (2001). Dating violence against adolescent girls and associated substance use, unhealthy weight control, sexual risk behaviour, pregnancy, and suicidality. Journal of the American Medical Association, 286(22), 572–579.
Stenson, K., Saarinen, H., Heimer, G., & Sidenvall, B. (2001). Women’s attitudes to being asked about exposure to violence. Midwifery, 17(1), 2–10.
Stenson, K., Sidenvall, B., & Heimer, G. (2005). Midwives’ experiences of routine antenatal questioning relating to men’s violence against women. Midwifery, 21(4), 311–21.
Stephens, D. L. (1999). Battered women’s views of their children. Journal of Interpersonal Violence, 14, 731–746.
Straus, M. A., & Gelles, R. J. (1990). Physical violence in American families: Risk factors and adaptations to violence in 8,145 families. New Brunswick, NJ: Transaction.
World Health Organisation. (2001). Putting women first: ethical and safety recommendations for research on domestic violence against women. Geneva, Switzerland: World Health Organisation.
World Health Organization. (2002). World report on violence and health. Geneva: Switzerland.
Zimbabwe Demographic and Health Survey (2006). Domestic violence. ZDHS 2006.
Electronic References
Speaking out against global violence: -domestic violence. Retrieved June 01, 2006 from: http://www.feminist.com/violence/spot/
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Okenwa, L.E., Lawoko, S. & Jansson, B. Exposure to Intimate Partner Violence Amongst Women of Reproductive Age in Lagos, Nigeria: Prevalence and Predictors. J Fam Viol 24, 517–530 (2009). https://doi.org/10.1007/s10896-009-9250-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10896-009-9250-7