
Abstract
Structural magnetic resonance imaging (MRI) studies reported gray matter (GM) loss in bipolar disorder (BD) in cingulate cortices, key regions subserving emotional regulation and cognitive functions in humans. The aim of this study was to further explore cingulate GM volumes in a sizeable group of BD patients with respect to healthy controls, particularly investigating the impact of gender and clinical variables. 39 BD patients (mean Age = 48.6 ± 9.7, 15 males and 24 females) and 39 demographically matched healthy subjects (mean Age = 47.9 ± 9.1, 15 males and 24 females) underwent a 1.5T MRI scan. GM volumes within the cingulate cortex were manually detected, including anterior and posterior regions. BD patients had decreased left anterior cingulate volumes compared with healthy controls (F = 6.7, p = 0.01). Additionally, a significant gender effect was observed, with male patients showing reduced left anterior cingulate cortex (ACC) volumes compared to healthy controls (F = 5.1, p = 0.03). Furthermore, a significant inverse correlation between right ACC volumes and number of hospitalizations were found in the whole group of BD patients (r = − 0.51, p = 0.04) and in male BD patients (r = − 0.88, p = 0.04). Finally, no statistically significant correlations were observed in female BD patients. Our findings further confirm the putative role of the ACC in the pathophysiology of BD. Interestingly, this study also suggested the presence of gender-specific GM volume reductions in ACC in BD, which may also be associated to poor outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bipolar disorder (BD) is defined as a chronic disease affecting around 3% of the population worldwide [1] with the peak age of onset in adolescence and early adult life [2]. Its neurobiology has been widely investigated by several magnetic resonance imaging (MRI) studies, which identified selective structural and functional abnormalities in specific brain areas involved in emotional and cognitive processing [3,4,5,6,7,8], with specific regards to the cingulate cortex [9,10,11]. The cingulate cortex is part of the limbic system, which can be divided into an anterior and a posterior region, subserving cognitive and affective processing, respectively [9, 12, 13]. Interestingly, although the majority of the MRI studies showed gray matter (GM) volume reductions in the cingulate cortex in BD compared to healthy controls, the side of these abnormalities is still not well elucidated. Indeed, some studies suggested a volumetric reduction in right or bilateral anterior cingulate cortex (ACC) [14,15,16] while others found a reduction in left or bilateral posterior cingulate cortex [16,17,18,19,20,21].
Furthermore, gender might play an important role not only in the clinical presentation of BD [22] but possibly also in its structural and functional underpinnings [23]. Indeed, it has been suggested that women had increased risk to develop BD type II disorder and are more likely to have depressive episodes than man [22, 24]. Also, from a neurobiological prospective, it has been reported that women had higher percentage of gray and white matter volumes compared to men [25].
As per the cingulate cortex, two independent investigations showed significant gender effects in this region in BD, with, however, opposite results. Indeed, while Lochhead et al. [20] showed reduced GM volumes in male BD patients, Fornito et al. [26] reported increased thickness in the same group of BD patients. Interestingly, recent meta-analyses also suggested that GM reductions in cingulate cortex (and insula) were more extensive in both male BD patients and patients with schizophrenia [27, 28].
Finally, some evidence also reported that illness severity might have a putative role in cingulate cortex dysfunctions in BD patients. In particular, Min-Seong Koo et al. [29] showed a progression of GM volume deficits in the subgenual cingulate in patients with first episode affective psychosis, after a follow-up of approximately 18 months. Also Doris et al. [29] found an abnormal reduction of GM density, mainly in fronto-limbic cortex, and particularly in cingulate cortex, in poor outcome BD patients compared to healthy controls. In contrast, other MRI studies found that the reduction of GM volumes within the cingulate cortex were already present at the onset of BD [29,30,31,32]. Therefore, based on this evidence, it seems still not clear whether cingulate cortex abnormalities are a state or a trait marker of BD.
In conclusion, based on this evidence, this study aimed to investigate GM volume alterations within the anterior and posterior subdivisions of the cingulate cortex in a group of BD patients and age- and gender-matched healthy controls. Also, we further explored the putative role of gender and illness severity on GM alteration in the cingulate cortex.
We hypothesize that BD patients, and especially male patients, would have a significant reduction in GM volumes in the cingulate cortex compared to healthy controls and also that these alterations would be significantly associated with clinical measures evaluating the severity of the illness.
Methods
Participants
Thirty-nine BD patients with a DSM-IV diagnosis and 39, 1:1 age-, gender-, and race-matched, healthy controls were recruited (Tables 1, 2). They were being treated by the South Verona Community-based Mental Health Service (CMHS) and by other clinics reporting to the South-Verona Psychiatric Case Register (PCR) [33]. Diagnoses for BD were obtained using the Item Group Checklist of the Schedule for Clinical Assessment in Neuropsychiatry (IGC-SCAN) and confirmed by the clinical consensus of two staff psychiatrists. The IGC-SCAN was performed by two trained research clinical psychologists with extensive experience in the procedure. We ensured the reliability of the IGC-SCAN diagnoses by holding regular consensus meetings with the psychiatrists treating the patients and a senior investigator. Patients with co-morbid psychiatric disorders, alcohol or substance abuse within the 6 months preceding the study, history of traumatic head injury with loss of consciousness (over 15 min), epilepsy or other neurological diseases were excluded. All but nine patients were receiving antipsychotic medications at the time of scanning and 14 patients were treated with Lithium (currently or in the past). Patients’ clinical information was retrieved from psychiatric interviews, the attending psychiatrist and medical charts. Clinical symptoms were assessed using the Brief Psychiatric Rating Scale (BPRS 24-item version). Finally, the Client Socio-Demographic and Service Receipt Inventory—European Version (CSSRI-EU), a standardized Europe-wide validated instrument to evaluate health-service utilization and medication use for the domain of mental health care and the World Health Organization-Disability Assessment Schedule (WHO-DAS), a 12-item to evaluate difficulties due to health conditions, were administered.
Healthy controls had no DSM-IV axis I disorders as determined by either the SCID non-patient version [34] and they had to be 18–65 years of age with no history of or current psychiatric, neurologic, or substance-related disorder. Exclusion criteria were history of any axis I psychiatric disorder in first-degree relatives and any current medical problems.
All participants provided signed informed consent, after having understood all issues involved in participation in the research. The research was approved by the biomedical Ethics Committee of the Azienda Ospedaliera of Verona.
Acquisition parameters
A 1.5-T GE Signa Imaging System running version Signa 5.4.3 software (General Electric Medical Systems, Milwaukee) was used to acquire the MRI scans. First, explorative sagittal scout series T1-weighted spin-echo (SE) (N sections = 18, TR = 250 ms, TE = 14 ms, flip angle = 90o, FOV = 230 × 230, slice thickness = 5 mm, matrix size = 384 × 512, NEX = 2, t acquisition = 2 min 52 s) was obtained to confirm patients’ head position and image quality and to locate a midline sagittal image. Graphic prescription of the coronal and axial images was obtained through a T1-weighted sagittal scout image. A double echo-spin sequence was used to obtain a proton density and T2-weighted image turbo spin-echo (TSE) (N sections = 20 × 2, TR = 2500 ms, TE = 24/121 ms, flip angle = 180°, FOV = 230 × 230, slice thickness = 5 mm, matrix size = 410 × 512, NEX = 2, turbo factor = 5, t acquisition = 3 min 25 s) in the axial plane to exclude the presence of focal lesions. A subsequent structural MRI analysis was performed on 3D MultiPlanar Recontruction (MPR) T1 coronal acquisitions, in Charcot plane (N sections = 144, TR = 2060 ms, TE = 3.9 ms, flip angle = 15°, FOV = 176 × 235 mm, slice thickness = 1.25 mm, matrix size = 270 × 512, TI = 1100, NEX = 1, t acquisition = 5 min 23 s). All anatomical measurements were conducted on a Dell PC workstation (Dell Computers, Austin, Tex.) using the semi-automated software Scion Image Beta-3 b for Windows (Scion Corporation, Inc., Frederick, Md.).
Delimitation of regions of interest within the cingulate cortex
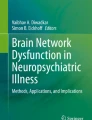
Based on the evidence suggesting the key role of cingulate cortex in the pathophysiology of BD, due to its role in integrating cognitive and emotional functions [35], a region of interest (ROI) approach was employed. Specifically, in the T1-weighted images, ROIs were manually traced and placed, bilaterally, using BRAINS2 software developed at the University of Iowa, by a single operator blind to subjects’ identity and to the other variables of the study (C.P.) (Fig. 1). Intra-class correlation coefficients (ICCs) higher than 0.90 for all the ROIs were obtained by two raters (C.P. and M.B.) blindly tracing 10 randomly selected scans.

Manual tracing of the cingulate cortex in coronal (a–d), sagittal (e) and axial (f) axes
The way the cingulate cortex was delimited has been already described in Kaur et al. [18]. Briefly, the cingulate was divided into four sections, anterior and posterior, right and left. We measured each section separately. All tracings of the cingulate were done in the coronal view and were measured using manual tracing to confirm structural alterations. The first slice traced was two slices anterior to the final slice where the genu was visible. Tracing was continued until the anterior commissure was apparent, and this marked the posterior limit of the ACC. The subsequent slice marked the anterior border of the posterior cingulate. The final slice measured was the one where the cerebral aqueduct appeared within the pons. Cingulate cortex tracing was done for GM only. The volumes of all ROIs were expressed in cm3.
Statistical analyses
All analyses were conducted using SPSS software (SPSS Inc, Chicago). All null hypotheses were rejected at the 0.05 level of significance using two-sided testing. Data were analyzed using factorial analysis of covariance (ANCOVA) to explore group and gender differences in cingulate cortex volumes in BD patients vs healthy controls, with total intra-cranial volumes (ICV) as continuous covariate. Finally, to investigate the possible effects of age and other clinical variables on cingulate cortex volumes, partial correlations with ICV as controlling variable were calculated.
Results
The analysis within the whole sample showed a significantly smaller GM volumes in left ACC in BD patients compared to healthy controls (F = 6.7, p = 0.01) (Table 3). After stratifying the sample by gender we found that only male BD patients showed the same statistically significant reduction in left ACC compared to male healthy controls (F = 5.1, p = 0.03) (Table 3). No differences in any other GM volumes within the cingulate cortex as well as no group by gender or group by gender by hemisphere interactions in any regions of the cingulate cortex were observed (all p > 0.05).
Moreover, in the whole group of BD patients, no statistically significant correlation was found between left (ACC: r = 0.17, p = 0.1; posterior cingulate cortex [PCC]: r = 0.18, p = 0.1) or right (ACC: r = 0.10, p = 0.8; PCC: r = − 0.008, p = 0.9) cingulate cortex and age. Moreover, left or right cingulate cortex did not correlate with any clinical variables, including duration of illness (left ACC: r = − 0.33, p = 0.2; right ACC: r = − 0.44, p = 0.09; left PCC: r = 0.15, p = 0.5; right PCC: r = 0.02, p = 0.9), age of onset (left ACC: r = 0.12, p = 0.6; right ACC: r = 0.44, p = 0.09; left PCC: r = 0.04, p = 0.8; right PCC: r = − 0.02, p = 0.9), duration of antipsychotic therapy (left ACC: r = − 0.29, p = 0.3; right ACC: r = − 0.20, p = 0.4; left PCC: r = 0.32, p = 0.2; right PCC: r = 0.15, p = 0.5), BPRS (left ACC: r = − 0.09, p = 0.7; right ACC: r = − 0.01, p = 0.9; left PCC: r = − 0.85, p = 0.7; right PCC: r = 0.49, p = 0.6), BRMRS (left ACC: r = − 0.11, p = 0.9; right ACC: r = 0.14, p = 0.6; left PCC: r = 0.49, p = 0.06; right PCC: r = 0.44, p = 0.09), and HDRS (left ACC: r = 0.16, p = 0.6; right ACC: r = − 0.27, p = 0.3; left PCC: r = − 0.30, p = 0.2; right PCC: r = − 0.06, p = 0.8) scores, with the exception of number of hospitalizations, which statistically significant correlated with right ACC (r = − 0.51, p = 0.04).
Similarly, in male BD patients, no statistically significant correlation was found between left (ACC: r = 0.63, p = 0.2; PCC: r = 0.30, p = 0.6) or right (ACC: r = 0.75, p = 0.1; PCC: r = − 0.07, p = 0.9) cingulate cortex and age. Moreover, left or right cingulate cortex did not correlate with any clinical variables, including duration of illness (left ACC: r = − 0.32, p = 0.6; right ACC: r = − 0.60, p = 0.2; left PCC: r = − 0.31, p = 0.6; right PCC: r = − 0.69, p = 0.1), age of onset (left ACC: r = 0.54, p = 0.3; right ACC: r = 0.84, p = 0.07; left PCC: r = 0.40, p = 0.5; right PCC: r = 0.56, p = 0.3), duration of antipsychotic therapy (left ACC: r = − 0.32, p = 0.6; right ACC: r = − 0.60, p = 0.2; left PCC: r = − 0.31, p = 0.6; right PCC: r = − 0.69, p = 0.1), BPRS (left ACC: r = − 0.28, p = 0.6; right ACC: r = 0.17, p = 0.7; left PCC: r = − 0.29, p = 0.6; right PCC: r = 0.84, p = 0.07), BRMRS (left ACC: r = − 0.52, p = 0.3; right ACC: r = − 0.24, p = 0.6; left PCC: r = − 0.69, p = 0.1; right PCC: r = 0.37, p = 0.5), and HDRS (left ACC: r = 0.06, p = 0.9; right ACC: r = − 0.17, p = 0.7; left PCC: r = 0.57, p = 0.3; right PCC: r = 0.11, p = 0.8) scores, with the exception of number of hospitalizations, which statistically significant correlated with right ACC (r = − 0.88, p = 0.04).
Finally, no statistically significant correlations were observed in female BD patients. Specifically, left (ACC: r = − 0.51, p = 0.1; PCC: r = 0.10, p = 0.7) or right (ACC: r = − 010, p = 0.7; PCC: r = − 0.17, p = 0.7) cingulate cortex did not significant correlated with age. Additionally, left or right cingulate cortex did not correlate with any clinical variables, including duration of illness (left ACC: r = − 0.46, p = 0.2; right ACC: r = − 0.32, p = 0.3; left PCC: r = 0.25, p = 0.5; right PCC: r = − 0.16, p = 0.6), age of onset (left ACC: r = − 0.10, p = 0.7; right ACC: r = 0.21, p = 0.5; left PCC: r = − 0.13, p = 0.7; right PCC: r = − 0.30, p = 0.4), duration of antipsychotic therapy (left ACC: r = − 0.20, p = 0.6; right ACC: r = 0.63, p = 0.06; left PCC: r = 0.38, p = 0.3; right PCC: r = 0.50, p = 0.1), number of hospitalizations (left ACC: r = 0.23, p = 0.5; right ACC: r = − 0.44, p = 0.2; left PCC: r = 0.01, p = 0.9; right PCC: r = 0.22, p = 0.5), BPRS (left ACC: r = 0.20, p = 0.6; right ACC: r = − 0.18, p = 0.6; left PCC: r = 0.09, p = 0.8; right PCC: r = 0.50, p = 0.1), BRMRS (left ACC: r = − 0.02, p = 0.9; right ACC: r = 0.31, p = 0.4; left PCC: r = − 0.64, p = 0.6; right PCC: r = 0.51, p = 0.1), and HDRS (left ACC: r = 0.30, p = 0.4; right ACC: r = − 0.43, p = 0.2; left PCC: r = − 0.29, p = 0.4; right PCC: r = 0.10, p = 0.7) scores.
Discussion
GM volume alteration in left ACC: a biological marker of bipolar disorder?
Our results showed significant GM volume reductions in left ACC in BD patients compared to healthy controls. In general, the involvement of ACC in the regulation of emotion and executive functions has been widely demonstrated [36, 37] Therefore, it is not surprising that our results are in line with previous evidence showing GM volume reduction in the ACC in BD [3, 38,39,40] even at the onset of the disease [15, 18, 41,42,43]. In this direction, postmortem assessments of ACC tissue confirmed the reduction of GM volumes in BD and revealed that this abnormality could be associated with a reduction in glia, with no equivalent loss of neurons [38].
Furthermore, the left-sided deficit in the ACC observed in our study is in line with previous structural MRI studies [9, 16, 17, 44,45,46]. It has been hypothesized that left ACC abnormalities are linked to the cognitive decline and to the disrupted emotional processing often observed in BD [45, 47,48,49], based on the role of left hemisphere on rational, verbal and analytical performances in humans [50].
After stratifying the sample by gender, we confirmed the GM volume reduction in left ACC only in male BD patients compared to male healthy controls. Also in this case, our study is in agreement with the evidence reporting gender-related differences in BD in specific brain regions, including fronto-insular cortex and lateral ventricles [51,52,53]. However, although gender-related differences between males and females in cingulate cortex has been shown in healthy individuals [25, 54], evidence for gender differences in cingulate cortex in BD is still scarce. Nonetheless, our results are partially in line with two MRI studies reporting a significant GM volume reduction in left ACC [20] as well increased thickness in subcallosal cingulate cortex [26] in males BD patients. Finally, although our results did not show any significant group by gender or group by gender by hemisphere interaction, it might be the case that the group differences observed in left ACC could have been driven mostly by males. This is plausible because it has been reported that male patients have a worse manifestation of the illness, with earlier onset and more manic episodes [55], which might, therefore, predispose to more neurodegenerative events [56, 57]. Nonetheless, future studies with larger samples are needed to better clarify the involvement of the cingulate cortex in the pathophysiology of BD.
Correlation between ACC alterations and clinical variables
In our study, we found an inverse correlation between right ACC volumes and number of hospitalizations in BD patients, especially in males. In this context, our result seems to be in line with a previous study on poor outcome bipolar illness [28]. Indeed, the authors found a significant reduction of cingulate GM density in poor outcome BD patients with a high mean number of hospital admissions. Since, in general, it has been reported that hospitalizations correlate with higher number of episodes, longer duration of illness and a worse prognosis in BD [57,58,59,60,61], they may be associated to poor prognosis as well as to cingulate shrinkage.
Limitations
These results should be considered in light of few major limitations. First, our study group was relatively small although comparable with most of the prior studies, limiting the power of our analyses. Indeed, the relatively small sample size did not allow the correction for multiple comparisons for the analyses where we stratified the sample by gender, which must be, therefore, considered as exploratory. Therefore, further studies on larger samples are warranted to corroborate the specificity of GM reductions in the ACC found in our group of males BD patients. Second, patients were chronically treated, which did not allow us to fully exclude the impact of medication or chronicity on cingulate volumes. However, no significant effects of duration of treatment and length of illness were reported on volume measures. Finally, the small sample size employed in this study did not allow the investigation of the effect of Lithium on cortical GM. Although few patients (N = 14) were taking Lithium during or before the MRI scan, they could have affected the group analyses. Indeed, it has been suggested that the chronic lithium treatment may confer neuroprotection and it associated with regional increases in selective brain regions, including ACC [62].
Conclusions
Our study found decreased GM volumes in left ACC in BD patients compared to healthy controls, further supporting the hypothesis that ACC can be considered a neural underpinning of BD. Moreover, our results also indicated the presence of male-related volume reductions in ACC in BD. Finally, right ACC volumes inversely correlated with number of hospitalizations, particularly in male patients, being potentially predictive of poor prognosis. Future larger longitudinal studies enrolling BD patients at the earlier phases of the illness are needed to better understand the trajectories of ACC changes separately in males and females and their relationship with clinical outcome over time.
Change history
15 June 2018
In the original publication of the article, the title was incorrect. The correct title should read as given below.
References
Kessler RC, Chiu WT, Demler O et al (2005) Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry 62:617
Fagiolini A, Forgione R, Maccari M et al (2013) Prevalence, chronicity, burden and borders of bipolar disorder. J Affect Disord 148:161–169
Maggioni E, Bellani M, Altamura AC, Brambilla P (2016) Neuroanatomical voxel-based profile of schizophrenia and bipolar disorder. Epidemiol Psychiatr Sci 25:312–316
Houenou J, Perlini C, Brambilla P (2015) Epidemiological and clinical aspects will guide the neuroimaging research in bipolar disorder. Epidemiol Psychiatr Sci 24:117–120
Bellani M, Boschello F, Delvecchio G et al (2016) DTI and myelin plasticity in bipolar disorder: integrating neuroimaging and neuropathological findings. Front psychiatry 7:21
Hozer F, Houenou J (2016) Can neuroimaging disentangle bipolar disorder? J Affect Disord 195:199–214
Wolfers T, Buitelaar JK, Beckmann CF et al (2015) From estimating activation locality to predicting disorder: a review of pattern recognition for neuroimaging-based psychiatric diagnostics. Neurosci Biobehav Rev 57:328–349
Nery FG, Monkul ES, Lafer B (2013) Gray matter abnormalities as brain structural vulnerability factors for bipolar disorder: a review of neuroimaging studies of individuals at high genetic risk for bipolar disorder. Aust New Zeal J Psychiatry 47:1124–1135
Fountoulakis KN, Giannakopoulos P, Kövari E, Bouras C (2008) Assessing the role of cingulate cortex in bipolar disorder: Neuropathological, structural and functional imaging data. Brain Res Rev 59:9–21
Soares JC, Mann JJ (1997) The functional neuroanatomy of mood disorders. J Psychiatr Res 31:393–432
Marlinge E, Bellivier F, Houenou J (2014) White matter alterations in bipolar disorder: potential for drug discovery and development. Bipolar Disord 16:97–112
Vogt BA, Nimchinsky EA, Vogt LJ, Hof PR (1995) Human cingulate cortex: surface features, flat maps, and cytoarchitecture. J Comp Neurol 359:490–506
Zimmerman ME, DelBello MP, Getz GE et al (2006) Anterior cingulate subregion volumes and executive function in bipolar disorder. Bipolar Disord 8:281–288
Bruno SD, Barker GJ, Cercignani M et al (2004) A study of bipolar disorder using magnetization transfer imaging and voxel-based morphometry. Brain 127:2433–2440
Farrow TFD, Whitford TJ, Williams LM et al (2005) Diagnosis-related regional gray matter loss over two years in first episode schizophrenia and bipolar disorder. Biol Psychiatry 58:713–723
Sassi RB, Brambilla P, Hatch JP et al (2004) Reduced left anterior cingulate volumes in untreated bipolar patients. Biol Psychiatry 56:467–475
Atmaca M, Ozdemir H, Cetinkaya S et al (2007) Cingulate gyrus volumetry in drug free bipolar patients and patients treated with valproate or valproate and quetiapine. J Psychiatr Res 41:821–827
Kaur S, Sassi RB, Axelson D et al (2005) Cingulate cortex anatomical abnormalities in children and adolescents with bipolar disorder. Am J Psychiatry 162:1637–1643
Lim KO, Rosenbloom MJ, Faustman WO et al (1999) Cortical gray matter deficit in patients with bipolar disorder. Schizophr Res 40:219–227
Lochhead RA, Parsey RV, Oquendo MA, Mann JJ (2004) Regional brain gray matter volume differences in patients with bipolar disorder as assessed by optimized voxel-based morphometry. Biol Psychiatry 55:1154–1162
Nugent AC, Milham MP, Bain EE et al (2006) Cortical abnormalities in bipolar disorder investigated with MRI and voxel-based morphometry. Neuroimage 30:485–497
Diflorio A, Jones I (2010) Is sex important? Gender differences in bipolar disorder. Int Rev Psychiatry 22:437–452
Jogia J, Dima D, Frangou S (2012) Sex differences in bipolar disorder: a review of neuroimaging findings and new evidence. Bipolar Disord 14:461–471
Altshuler LL, Kupka RW, Hellemann G et al (2010) Gender and depressive symptoms in 711 patients with bipolar disorder evaluated prospectively in the stanley foundation bipolar treatment outcome network. Am J Psychiatry 167:708–715
Cosgrove KP, Mazure CM, Staley JK (2007) Evolving knowledge of sex differences in brain structure, function, and chemistry. Biol Psychiatry 62:847–855
Fornito A, Yucel M, Wood SJ et al (2009) Anterior cingulate cortex abnormalities associated with a first psychotic episode in bipolar disorder. Br J Psychiatry 194:426–433
Bora E, Fornito A, Yücel M, Pantelis C (2012) The effects of gender on grey matter abnormalities in major psychoses: a comparative voxelwise meta-analysis of schizophrenia and bipolar disorder. Psychol Med 42:295–307
Crow TJ, Chance SA, Priddle TH et al (2013) Laterality interacts with sex across the schizophrenia/bipolarity continuum: an interpretation of meta-analyses of structural MRI. Psychiatry Res 210:1232–1244
Doris A, Belton E, Ebmeier KP et al (2004) Reduction of cingulate gray matter density in poor outcome bipolar illness. Psychiatry Res 130:153–159
Dazzan P, Soulsby B, Mechelli A et al (2012) Volumetric abnormalities predating the onset of schizophrenia and affective psychoses: an MRI study in subjects at ultrahigh risk of psychosis. Schizophr Bull 38:1083–1091
MORGAN KD, DAZZAN P, ORR KG et al (2007) Grey matter abnormalities in first-episode schizophrenia and affective psychosis. Br J Psychiatry 191:s111–s116
Gogtay N, Ordonez A, Herman DH et al (2007) Dynamic mapping of cortical development before and after the onset of pediatric bipolar illness. J Child Psychol Psychiatry 48:852–862
Pina-Camacho L, Del Rey-Mejías Á, Janssen J et al (2016) Age at first episode modulates diagnosis-related structural brain abnormalities in psychosis. Schizophr Bull 42:344–357
Tansella M, Burti L (2003) Integrating evaluative research and community-based mental health care in Verona, Italy. Br J Psychiatry 183:167–169
Emsell L, McDonald C (2009) The structural neuroimaging of bipolar disorder. Int Rev Psychiatry 21:297–313
Gasquoine PG (2013) Localization of function in anterior cingulate cortex: from psychosurgery to functional neuroimaging. Neurosci Biobehav Rev 37:340–348
Rive MM, van Rooijen G, Veltman DJ et al (2013) Neural correlates of dysfunctional emotion regulation in major depressive disorder. a systematic review of neuroimaging studies. Neurosci Biobehav Rev 37:2529–2553
Drevets WC, Price JL, Simpson JR et al (1997) Subgenual prefrontal cortex abnormalities in mood disorders. Nature 386:824–827
Molina V, Galindo G, Cortés B et al (2011) Different gray matter patterns in chronic schizophrenia and chronic bipolar disorder patients identified using voxel-based morphometry. Eur Arch Psychiatry Clin Neurosci 261:313–322
Fornito A, Malhi GS, Lagopoulos J et al (2008) Anatomical abnormalities of the anterior cingulate and paracingulate cortex in patients with bipolar I disorder. Psychiatry Res Neuroimaging 162:123–132
Hirayasu Y, Shenton ME, Salisbury DF et al (1999) Subgenual cingulate cortex volume in first-episode psychosis. Am J Psychiatry 156:1091–1093
Adler CM, DelBello MP, Jarvis K et al (2007) Voxel-based study of structural changes in first-episode patients with bipolar disorder. Biol Psychiatry 61:776–781
Kubicki M, Shenton ME, Salisbury DF et al (2002) Voxel-based morphometric analysis of gray matter in first episode schizophrenia. Neuroimage 17:1711–1719
Lyoo IK, Kim MJ, Stoll AL et al (2004) Frontal lobe gray matter density decreases in bipolar I disorder. Biol Psychiatry 55:648–651
Lyoo IK, Sung YH, Dager SR et al (2006) Regional cerebral cortical thinning in bipolar disorder. Bipolar Disord 8:65–74
Wise T, Radua J, Via E et al (2016) Common and distinct patterns of grey-matter volume alteration in major depression and bipolar disorder: evidence from voxel-based meta-analysis. Mol Psychiatry 22:1455–1463
Lennox BR, Jacob R, Calder AJ et al (2004) Behavioural and neurocognitive responses to sad facial affect are attenuated in patients with mania. Psychol Med 34:795–802
Gruber SA, Rogowska J, Yurgelun-Todd DA (2004) Decreased activation of the anterior cingulate in bipolar patients: an fMRI study. J Affect Disord 82:191–201
Yoshimura Y, Okamoto Y, Onoda K et al (2014) Psychosocial functioning is correlated with activation in the anterior cingulate cortex and left lateral prefrontal cortex during a verbal fluency task in euthymic bipolar disorder: a preliminary fMRI study. Psychiatry Clin Neurosci 68:188–196
Roland PE (1993) Brain activation. Wiley-Liss, New York
Monkul ES, Malhi GS, Soares JC (2005) Anatomical MRI abnormalities in bipolar disorder: do they exist and do they progress? Aust N Z J Psychiatry 39:222–226
Brambilla P, Glahn DC, Balestrieri M, Soares JC (2005) Magnetic resonance findings in bipolar disorder. Psychiatr Clin North Am 28:443–467
Mann SL, Hazlett EA, Byne W et al (2011) Anterior and posterior cingulate cortex volume in healthy adults: effects of aging and gender differences. Brain Res 1401:18–29
Kawa I, Carter JD, Joyce PR et al (2005) Gender differences in bipolar disorder: age of onset, course, comorbidity, and symptom presentation. Bipolar Disord 7:119–125
Arnold LM (2003) Gender differences in bipolar disorder. Psychiatr Clin North Am 26:595–620
Hochman E, Valevski A, Onn R et al (2016) Seasonal pattern of manic episode admissions among bipolar I disorder patients is associated with male gender and presence of psychotic features. J Affect Disord 190:123–127
DelBello M, Strakowski SM, Zimmerman ME et al (1999) MRI analysis of the cerebellum in bipolar disorder a pilot study. Neuropsychopharmacology 21:63–68
Brambilla P, Harenski K, Nicoletti M et al (2001) Differential effects of age on brain gray matter in bipolar patients and healthy individuals. Neuropsychobiology 43:242–247
Mills NP, DelBello MP, Adler CM, Strakowski SM (2005) MRI analysis of cerebellar vermal abnormalities in bipolar disorder. Am J Psychiatry 162:1530–1533
Robinson LJ, Thompson JM, Gallagher P et al (2006) A meta-analysis of cognitive deficits in euthymic patients with bipolar disorder. J Affect Disord 93:105–115
Moorhead TWJ, McKirdy J, Sussmann JED et al (2007) Progressive gray matter loss in patients with bipolar disorder. Biol Psychiatry 62:894–900
Silverstone PH, Wu RH, O’Donnell T, U et al (2003) Chronic treatment with lithium, but not sodium valproate, increases cortical N-acetyl-aspartate concentrations in euthymic bipolar patients. Int Clin Psychopharmacol 18(2):73–79
Acknowledgements
This study was partially supported by grants from the Italian Ministry of Health to PB and GD (RF-2011-02352308) and to MB (GR-2010-2319022). We thank Gianluca Rambaldelli for managing the dataset.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Delvecchio, G., Ciappolino, V., Perlini, C. et al. Cingulate abnormalities in bipolar disorder relate to gender and outcome: a voxel-based morphometry study. Eur Arch Psychiatry Clin Neurosci 269, 777–784 (2019). https://doi.org/10.1007/s00406-018-0887-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00406-018-0887-1